12747545
Descripción
Test por Plymouth Med, actualizado hace más de 1 año
|
|
Creado por Plymouth Med
hace alrededor de 6 años
|
|
Pregunta 1
Pregunta
BG:
48 year old female with 2 children
Hypertension- well controlled with Amlodipine
-Irritable bowel syndrome (15 year history) on Mebeverine
-Menorrhagia- vaginal hysterectomy 2 years ago
2 month Hx worsening bowels-
Alternating diarrhoea/constipation
Associated lower abdominal pain
Exam:
alert, afebrile, BP 132/70, HR 70, reg
Abdomen: mildly distended but soft non-tender (SNT), no masses, bowel sounds present
FHx: Sister- breast cancer aged 48
Aunt- breast cancer aged 61
What is the next management step would you advise for this patient?
Respuesta
-
Admit urgently
-
Pelvic Exam
-
Refer urgently
-
Reassure probably just IBS
-
Refer routinely and keep a close eye
-
Cardiorespiratory exame
-
Urine anaylsis
-
FBC
Pregunta 2
Pregunta
BG: 53 year old male, Vetenarian,
MHx – hypertension
PC: Agreed routine review to discuss blood results
Notable results:
Bili 131 (15-73)
GGT 432 (15-73)
ALP 505 (30-130)
ALT 3017 (21-72)
Eventually got hold of him 10 days later- he was on holiday!
Whilst away admitted to a couple days when urine slightly darker and stools paler but since resolved
Approx 5 units/week alcohol
Reviewed in clinic:
No abdo pain, no stigmata liver disease
Exam: obs stable, sclera slightly jaundiced, abdomen soft, nontender, no hepatosplenomegaly
What is(are) the most appropriate next step(s)?
Respuesta
-
Refer routinely
-
Refer urgently
-
Admit urgently
-
Full Liver Screen
-
Repeat LFTS
-
Caeruloplasmin Serum levels
-
Autoimmune profile
-
Hepatitis Screen
-
Repeat Blood tests
-
Gallbladder ultrasound
Pregunta 3
Pregunta
Same Patient:
blood tests repeated: Improving LFTs-except ALT still elevated
Liver Screen: all negative but Hepatits Screen:
Hep A: IgG + and IgM -
Hep E: IgG + and IgM +
What is a correct interpretation of these results?
Respuesta
-
IgM + means that newly exposed to the pathogen
-
IgG+ means that newly exposed to the pathogen
-
IgM- that newly exposed to the pathogen
Pregunta 4
Pregunta
What are possible differential diagnoses of raised ALT?
Respuesta
-
Alcoholic liver disease
-
Wilsons
-
Viral hepatitis
-
Celiac
-
Alpha 1 Antitrypsin deficiency
-
Hemochromatosis
-
Certain drugs
-
Nonalcoholic fatty liver disease
-
Nelson's disease
-
Renal Failure
Pregunta 5
Pregunta
Abdominal Examination findings:
Pain in the foregut ( [blank_start]esophagus[blank_end] to mid-duodenum, liver, [blank_start]gallbladder[blank_end], spleen, 1/2 [blank_start]pancreas[blank_end]) can be felt in the [blank_start]epigastric[blank_end] region.
Pain in the midgut (mid-duodenum to [blank_start]proximal[blank_end] 2/3 transverse colon and 1/2 [blank_start]pancreas[blank_end]) can be felt in the [blank_start]umbilical[blank_end] region.
Pain in the hindgut ([blank_start]distal[blank_end] 2/3 of transverse colon to 1/2 of [blank_start]anal[blank_end] [blank_start]canal[blank_end]) is usually in the [blank_start]pubic[blank_end] region.
Respuesta
-
esophagus
-
gallbladder
-
pancreas
-
pancreas
-
proximal
-
distal
-
anal
-
canal
-
umbilical
-
epigastric
-
pubic
Pregunta 6
Pregunta
Any gynae problem, always do a pregnancy test first.
Respuesta
- True
- False
Pregunta 7
Pregunta
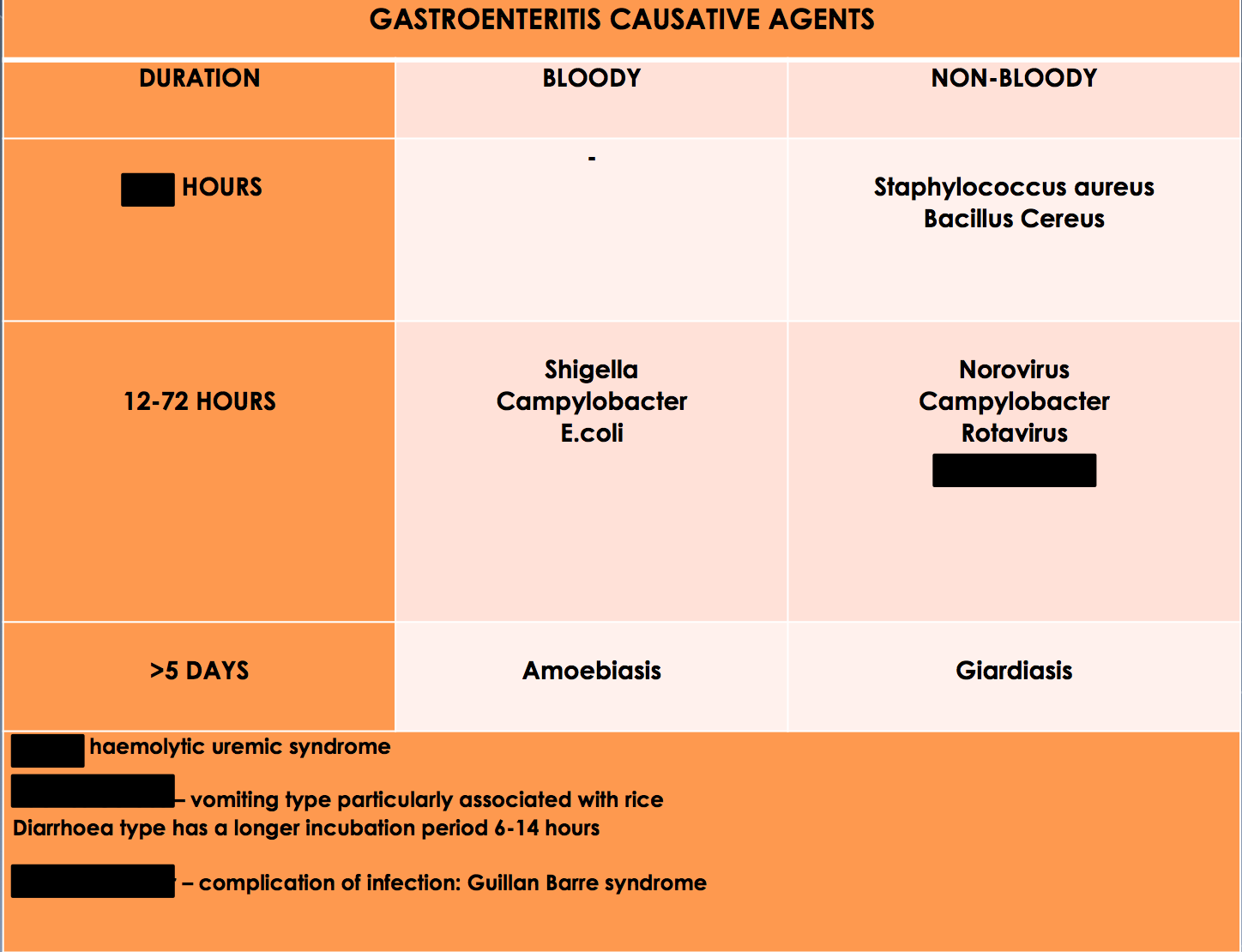
24 year old presents complaining of a 2 day history of abdominal pain, vomiting and diarrhoea. He had made some stir fried rice for dinner 3 days ago and forgot to put it in the fridge. He has had no recent travel and is otherwise fit and well. A diagnosis of gastroenteritis is made.
What is your most likely causative organism?
Respuesta
-
Campylobacter
-
Cholera
-
E. Coli
-
Bacillus Cereus
Pregunta 8
Pregunta
Always seek urgent specialist advice whenever a child or elderly are reported to have has a single episode of bloody diarrhoea
Respuesta
- True
- False
Pregunta 9
Pregunta
Management of acute diarrhea and gastroenteritis:
Conservative: Fluids and [blank_start]electrolytes[blank_end]
Medical: [blank_start]Antibiotics[blank_end] (if [blank_start]systematically[blank_end] unwell) and whould be based off of [blank_start]stool[blank_end] culture results
Respuesta
-
electrolytes
-
Antibiotics
-
systematically
-
stool
Pregunta 10
Pregunta
A 27 year old lady presents to you with a 6 month history of abdominal pain and bloating after meals. Her pain is relieved after defecation. She is also suffering from alternating diarrhoea and constipation and feels like she hasn’t emptied her bowels properly. She is very distressed about her symptoms as it is affecting her personal and work life.
What is your main differential?
Respuesta
-
Hyperthyroidism
-
Irritable Bowel Syndrome
-
Endometriosis
-
Inflammatory Bowel Disease
Pregunta 11
Pregunta
[blank_start]Irritable[blank_end] [blank_start]bowel[blank_end] [blank_start]syndrome[blank_end] is a common chronic functional disorder of the bowel causing abdominal cramps, bloating, constipation and/or diarrhea. Most common is [blank_start]women[blank_end] in their 20-30s.
Respuesta
-
women
-
Irritable
-
bowel
-
syndrome
Pregunta 12
Pregunta
What is NOT a potential reason for irritable bowel syndrome?
Respuesta
-
overactive bowel
-
increased visceral hypersensitivity
-
short chain carbohydrates in diet
-
post-parturition incontinecne
Pregunta 13
Pregunta
Irritable bowel syndrome is diagnosed if there is at least a [blank_start]6[blank_end] month history of abdomen pain, [blank_start]altered[blank_end] bowel habit, and [blank_start]bloating[blank_end]. The diagnosis is official if the abdominal pain is relieved by [blank_start]defecation[blank_end] or linked to altered bowel habit and AT LEAST 2 OF:
passage of [blank_start]mucus[blank_end]
altered stool passage (urgency, frequency, [blank_start]tenesmus[blank_end])
abdominal bloating
symptoms worsened by [blank_start]eating[blank_end]
On examination, the abdomen is usually normal with some generalized [blank_start]tenderness[blank_end]
Respuesta
-
tenderness
-
6
-
altered
-
bloating
-
defecation
-
mucus
-
tenesmus
-
eating
Pregunta 14
Pregunta
What are ways to generally investigate for irritable bowel syndrome?
Respuesta
-
Full blood count
-
ESR (erythrocyte sedimentation rate)
-
C reactive protein
-
TTGA
-
fecal calprotetectin
-
CA125
-
CA173
-
imaging
-
Hepatitis C
-
hcg
Pregunta 15
Pregunta
Main managements of IBS is dietary changes, peppermint old, and (if needed) loperamide
Respuesta
- True
- False
Pregunta 16
Pregunta
Buscapan can be given for irritable bowel syndrome.
Respuesta
- True
- False
Pregunta 17
Pregunta
A 45 year old gentleman presents with 7 month history of abdominal pain and unintentional weight loss. He has been feeling more tired lately and has noticed he has become increasingly paler. He has a PMH of asthma and coeliac disease. He explains that his father and his brother also experienced similar symptoms and were subsequently diagnosed with colorectal cancer.
What is your main differential?
Respuesta
-
Irritable bowel syndrome
-
Colorectal cancer
-
Crohn's disease
-
Ulcerative Colitis
Pregunta 18
Pregunta
IBD and HNPCC put you at increased risk for colorectal cancer
Respuesta
- True
- False
Pregunta 19
Pregunta
What are these symptomatic of?
Often colicky pain
Rectal bleeding
Bowel obstruction
Tenesmus
Mass in LIF
Early changes in bowel habit
Respuesta
-
left colon cancers
-
right colon cancers
-
HPNCC
-
small cell colon cancers
-
familial colon cancers
Pregunta 20
Pregunta
What are these symptomatic of:
Weight loss
Anemia
Occult bleeding
Mass in RIF
Respuesta
-
right colon cancers
-
left colon cancers
-
IBS
-
small cell colon cancer
-
familial colon cancers
Pregunta 21
Pregunta
Most common presentation of colorectal cancer:
[blank_start]rectal[blank_end] [blank_start]bleeding[blank_end]
[blank_start]persisting[blank_end] change in bowel habit
[blank_start]anemia[blank_end]
Respuesta
-
anemia
-
persisting
-
rectal
-
bleeding
Pregunta 22
Pregunta
Urgent referral for cancer pathway if the patient is aged 40 and over with unexplained weight loss and abdominal pain.
Respuesta
- True
- False
Pregunta 23
Pregunta
How can you NOT investigate colorectal cancer?
Respuesta
-
Bedside tests
-
Liver function test
-
Urea and Electrolytes test
-
Thyroid function tests
-
CEA blood test
-
Colonoscopy
-
Biopsy
-
Flexible sigmoidoscopy and barium enema
-
MRI
-
Ultrasound
Pregunta 24
Pregunta
The earlier the Duke stage (for ex: stage A vs stage B), the lower 5-year survival likelihood.
Respuesta
- True
- False
Pregunta 25
Pregunta
How can you manage colorectal cancer?
Respuesta
-
chemotherapy
-
palliative therapy
-
radiotherapy
-
surgery
-
multidisciplinary team approach
-
screening
-
drugs
-
bedside monitoring
Pregunta 26
Pregunta
Bowel Cancer Screening Program:
In England, men and women between the ages of [blank_start]60[blank_end]-74 years take part
A bowel cancer testing kit is sent every [blank_start]2[blank_end] years
2 bowel cancer screening tests:
[blank_start]Fecal[blank_end] [blank_start]occult[blank_end] blood testing – home testing kit
Flexi-[blank_start]sigmoidoscopy[blank_end] – looking for polyps – one at age 55 years
Respuesta
-
2
-
60
-
Fecal
-
occult
-
sigmoidoscopy
Pregunta 27
{kind=link}
Respuesta
-
4-6
-
salmonella
-
E. coli
-
Bacillus Cereus
-
Campylobacter
Pregunta 28
Pregunta
Which is pelvic pain associated with?
Respuesta
-
gastrointestinal problems
-
gynecological problems
-
musculoskeletal problems
-
urological problems
-
cardiovascular problems
Pregunta 29
Pregunta
What is true regarding Chlamydia trachomatis?
Respuesta
-
small gram negative
-
infect columnar and transitional epithelium
-
sexually transmitted infection
-
causes infertility
-
more common in younger adults
-
asymptomatic
-
small gram positive
-
febrile
-
affects cognitive functionality
-
lies dormant before manifesting later in life
Pregunta 30
Pregunta
Women with chlamydia present with dysuria and yellowish discharge and irregular bleeding
Respuesta
- True
- False
Pregunta 31
Pregunta
Males with chlamydia present with epididymitis, hematuria, dysuria, discharge, and sudden bursts of weakness
Respuesta
- True
- False
Pregunta 32
Pregunta
Investigations for chlamydia:
Male: [blank_start]first[blank_end]-catch [blank_start]urine[blank_end]
Female: [blank_start]vulvovaginal[blank_end] swab
Both samples are sent for NAATs ([blank_start]nucleic[blank_end] [blank_start]acid[blank_end] [blank_start]amplification[blank_end] test)
Respuesta
-
first
-
urine
-
vulvovaginal
-
nucleic
-
acid
-
amplification
Pregunta 33
Pregunta
Chlamydia complications:
[blank_start]pelvic[blank_end] inflammatory disease, infertility, [blank_start]ectopic[blank_end] pregnancy
Treatments:
100mg [blank_start]Doxycycline[blank_end] (danger: [blank_start]teratogenic[blank_end]) or 1 gram stat [blank_start]Azithromycin[blank_end]
Respuesta
-
teratogenic
-
Azithromycin
-
Doxycycline
-
ectopic
-
pelvic
Pregunta 34
Pregunta
Neisseria Gonnorhea is
Gram-[blank_start]negative[blank_end] diplococcus
Infects mucous membranes of the urethra, [blank_start]endocervix[blank_end], rectum, [blank_start]pharynx[blank_end] and conjunctiva
transmitted sexually or [blank_start]perinatally[blank_end]
Presentation:
Women:
[blank_start]Urinary[blank_end] [blank_start]Tract[blank_end] Infection
Discharge
[blank_start]Dysuria[blank_end]
Men:
Discharge: [blank_start]green[blank_end] and thick
[blank_start]dysuria[blank_end]
Respuesta
-
negative
-
pharynx
-
endocervix
-
perinatally
-
Urinary
-
Tract
-
Dysuria
-
green
-
dysuria
Pregunta 35
Pregunta
Investigation for Gonnorhea:
Women: [blank_start]Pharynx[blank_end], vaginal, rectal swab
Men: Pharynx, [blank_start]urethral[blank_end], rectal swab
Respuesta
-
Pharynx
-
urethral
Pregunta 36
Pregunta
Ceftriaxone 500mg IM and Azithromycin 3G stat is how to treat gonnorhea.
Respuesta
- True
- False
Pregunta 37
Pregunta
Which of these are complications of gonnorhea?
Respuesta
-
urethral scarring
-
penile lymphangitis
-
epididymitis
-
prostatis
-
miscarriage
-
pre mature labor
-
infertility
-
perlvic inflammatory disease
-
meningtis
-
ischemic bladder
Pregunta 38
Pregunta
What is the differential diagnosis for these symptoms?
lower abdominal pain
Deep dyspareunia
Abnormal vaginal bleeding and/or discharge
Right upper quadrant pain
Lower abdominal tenderness
Adnexal tenderness, cervical motion tenderness, or uterine tenderness
Abnormal cervical or vaginal mucopurulent discharge
Fever greater than 38°C
Respuesta
-
gonnorhea
-
chlaymdia
-
syphilis
-
inflammatory pelvic disease
-
dysmennorhea
-
inflammatory bowel disease
Pregunta 39
Pregunta
[blank_start]Peri[blank_end]-[blank_start]hepatitis[blank_end] is the development of adhesions between the liver and the peritoneum, causing right [blank_start]upper[blank_end] quadrant pa
Respuesta
-
hepatitis
-
Peri
-
upper
Pregunta 40
Pregunta
How do you manage pelvic inflammatory disease?
Respuesta
-
screen for STIs
-
paracetamol
-
ibuprofen
-
Oral ofloxacin/levofloxacin + oral metronidazole for 14 days
-
Ceftriaxone as a single IM dose, followed by oral doxycycline + oral metronidazole for 14 days
-
Oral cefixime as a single dose (off-label use), followed by oral doxycycline + oral metronidazole for 14 days.
-
Aspirin
-
Oral ofloxacin/levofloxacin or 14 days
-
Ceftriaxone as a single IV dose, followed by oral doxycycline + oral metronidazole for 14 days
-
Ceftriaxone as a single IM dose, followed by oral doxycycline for 14 days
Pregunta 41
Pregunta
The most common cause of a UTI is E colli
Respuesta
- True
- False
Pregunta 42
Pregunta
Obesity, poor bladder emptying, diabetes, kidney stones, and Vitamin E deficiency all put you at increased risk of a UTI.
Respuesta
- True
- False
Pregunta 43
Pregunta
In a UTI, there will be increased urgency and frequency of urination despite it being painful due to the feeling of incomplete urination.
Respuesta
- True
- False
Pregunta 44
Pregunta
What do you pay special notice for in a urinalysis of a UTI?
Respuesta
-
leukocytes
-
nitrates
-
blood
-
pH
-
concentration
-
glucose
-
ammonia
Pregunta 45
Pregunta
Which of these is not a possible complication of a UTI?
Respuesta
-
Renal abscess
-
Sepsis
-
Acute kidney injury
-
Pyelonephritis
-
Fungal Vaginal infections
Pregunta 46
Pregunta
Management of UTI:
[blank_start]Fluids[blank_end] (supportive)
Analgesia
1. [blank_start]Trimethoprim[blank_end]
2. [blank_start]Nitrofurantoin[blank_end]
for:
Women - [blank_start]3[blank_end] days
Men - [blank_start]7[blank_end] days
Respuesta
-
3
-
7
-
Fluids
-
Trimethoprim
-
Nitrofurantoin
Pregunta 47
Pregunta
While both occur shortly after menarche, there is no underlying pelvic pathology in primary dysmennorea like there is in secondary dysmenorrhea.
Respuesta
- True
- False
Pregunta 48
Pregunta
Which of these may NOT be the reason for secondary dysmenorrhea?
Respuesta
-
Pelvic inflammatory disease
-
Fibroids
-
Adhesions
-
Endometriosis
-
Meniere's disease
Pregunta 49
Pregunta
[blank_start]Primary[blank_end] dysmennorhea is pain which begins just before menstruation and lasts up to [blank_start]72[blank_end] hours, progressively improving
Respuesta
-
Primary
-
72
Pregunta 50
Pregunta
NSAIDS, analgesia and contraceptive pill is how to manage dysmenorrhea.
Respuesta
- True
- False
Pregunta 51
Pregunta
You use ultrasounds and PAP smear tests to investigate for dysmenorrhea.
Respuesta
- True
- False
Pregunta 52
Pregunta
Which of these are emergency findings related to dysmenorrhea?
Respuesta
-
Abnormal cervix
-
persistent bleeding
-
pelvic mass
-
abdominal mass
-
ultrasound suggesting cancer
-
positive pregnancy test
-
distended abdomen
Pregunta 53
Pregunta
Contraception:
Starting the pill on day [blank_start]5[blank_end] or before protects from pregnancy straight away. Otherwise, patients will need additional contraception until taken for [blank_start]7[blank_end] days.
Respuesta
-
5
-
7
Pregunta 54
Pregunta
What is NOT true regarding the pill?
Respuesta
-
not taking it at the same time everyday makes it less effective
-
missing a dose makes it less effective
-
Vomiting makes it less effective
-
Severe diarrhea makes it less effective
-
It is taken every day for 21 days, then stopped for 7 days
-
It is not prescribed for those over the age 40
Pregunta 55
Pregunta
If you forgot to take the pill yesterday, the missed pill should still be taken, even if it means taking two pills in today.
Respuesta
- True
- False
¿Quieres crear tus propios Tests gratis con GoConqr? Más información.