7555322
Descripción
Fichas por Kristi Breese, actualizado hace más de 1 año
|
|
Creado por Kristi Breese
hace alrededor de 7 años
|
|
| Pregunta | Respuesta |
| Bi-PAP | 1. Done before mechanical ventilation 2. Noninvasive 3. Delivered through a tight fitting face mask, nasal mask or nasal pillows 4. Must breathe spontaneously & cooperate |
| Bi-PAP Indications | 1. Acute respiratory failure with COPD and heart failure 2. Sleep apnea |
| Endotracheal (ET) Intubation Procedure | Rapid sequence intubation (RSI) -Rapid, concurrent administration of a paralytic agent & a sedative agent during emergency airway management -increased risks of aspiration, combativeness, & injury to patient -not indicated for comatose or cardiac arrest patients |
| Following intubation - what to expect | 1. Confirmation - should hear bilateral lung sounds 2. Hemodynamic stability or instability 3. Settings 4. Comfort & control 5. Tube placement → Nosocomial breakdown 6. Monitoring (Labs) |
| The most potent vasodilator we make naturally | CO2 |
| Why is it important to have fluids nearby following intubation? | Before intubation, a patient can be air hungry and the fight or flight response kicks in (↑ BP, ↑HR, ↑RR). After intubation, there is increased vasodilation and BP can decrease rapid causing a shift in hemodynamics. Fluids can help support that stability |
| AACN Recommendations for ET suctioning | 1. Sawtooth pattern on vent tracing 2. Coarse crackles & rhonchi over trachea 3. ↓ Vt (tidal volume) 4. ↓ O2 Sat and/or ABG values 5. Visible secretions 6. Pts inability to generate an effective cough 7. Acute Resp Distress 8. Suspected or actual aspiration |
| Nursing Management - Artificial Airway | 1. Aspiration - tube feedings, HOB 2. Prevent unplanned extubation - The Joint Commission, Restraints (chemical & behavioral) |
| When to feed an intubated patient | -Determined by why the Pt is there, their metabolic state & co-morbidities -Some MDs will start a trickle tube feeding around day 3 just to keep the gut active -May go on TPN -Dietary consult should be obtained around day 3 |
| Mechanical Ventilation | -Process by which fraction inspired oxygen (FIO2) at ≥21% (room air) is moved into and out of lungs by a mechanical ventilator -Supportive NOT Curative -Temporary to Permanent |
| Indications for mechanical ventilation | -Apnea or impending inability to breathe -Acute respiratory failure -Severe hypoxia -Respiratory muscle fatigue |
| Settings of mechanical ventilators | -Regulate rate, depth, and other characteristics of ventilation -Based on patient’s status (e.g., ABGs, body weight, level of consciousness, muscle strength) -Ventilator is tuned to match patient’s ventilatory pattern |
| Positive pressure ventilation (PPV) | -Used primarily in acutely ill patients -Pushes air into lungs under positive pressure during inspiration -Expiration occurs passively |
| Positive end-expiratory pressure (PEEP) | -Mode of PPV -A little bit of positive pressure that stays in the alveoli to keep it open at the end of expiration |
| Cardiovascular complications of PPV | -PPV affects circulation → pressure to thoracic cavity -↑ Intrathoracic pressure compresses thoracic vessels: ↓ Venous return to heart, ↓ left ventricular end- diastolic volume (preload), ↓ cardiac output, Hypotension |
| Pulmonary complications of PPV | Barotrauma: -Air can escape into pleural space from alveoli or interstitium, accumulate, and become trapped →pneumothorax -COPD (rupt. Blebs) -Chest tubes may be placed prophylactically |
| Other complications of PPV | Pneumomediastinum -Begins with rupture of alveoli into lung interstitium -Progressive air movement into mediastinum and subcutaneous neck tissue -Commonly followed by pneumothorax |
| Other complications of PPV (cont) | Ventilator Associated Pneumonia (VAP) -Pneumonia that occurs 48 hours or more after ET intubation -Clinical evidence: Fever and/or elevated WBC count Purulent or odorous sputum Crackles or rhonchi on auscultation Pulmonary infiltrates on chest x-ray |
| Guidelines to prevent VAP | -ORAL CARE!!!!!!! -HOB elevation at least 30 to 45 degrees unless medically contraindicated -No routine changes of ventilator circuit tubing -Drain condensation that collects in ventilator tubing -Use of an ET that allows continuous suctioning of secretions in subglottic area |
| More complications of PPV | -Fluid retention -Neurologic system -Gastrointestinal system -Musculoskeletal system |
| Mechanical ventilation - Psychosocial needs | -Physical and emotional stress due to inability to speak, eat, move, or breathe normally -Pain, fear, and anxiety related to tubes/ machines -Ordinary ADLs are complicated or impossible -Involve patients in decision making -Encourage hope and build trusting relationships with patient and family -Provide sedation and/or analgesia to facilitate optimal ventilation |
| Psychosocial needs (cont) | -If necessary, provide paralysis to achieve more effective synchrony with ventilator and increase oxygenation -Paralyzed patient can hear, see, think, feel -Sedation and analgesia must always be administered concurrently -Assessment: Train-of-four peripheral nerve stimulation Physiologic signs of pain or anxiety Ventilator synchrony |
| Machine disconnection | -Most frequent site for disconnection is between tracheal tube and adapter -Pause alarms during suctioning or removal from ventilator (Reactivate alarms before leaving) -Malfunction may be due to power failure, failure of oxygen supply, etc. |
| What to do if machine malfunctions | -Disconnect patient from ventilator -Manually ventilate with 100% O2 |
| Nutritional therapy (TPN vs. Enteral) | -PPV and hypermetabolism can contribute to inadequate nutrition -If patient is likely to be without food for 3 to 5 days, a nutritional program should be initiated -Poor nutrition and disuse of respiratory muscles contributes to decreased muscle strength |
| Weaning from PPV & extubation | Process of: -Decreasing ventilator support -Resuming spontaneous ventilation -JUST PULL the TUBE -Patient Self-Extubations (85% Fly) |
| When weaning fails | Focus on tracheostomy |
| Definition of tracheostomy | -Surgical incision into the trachea to establish an airway -Stoma that results from tracheotomy |
| Tracheostomy indications | Prolonged intubations with unsuccessful weaning, management of bronchial hygiene, obstruction of the upper airway (head & neck trauma), and airway protection |
| Advantages of a tracheostomy | -Less of long-term damage to airway -Increased comfort -Patient can eat (potential) -Speaking (potential) -Increased mobility because tube is more secure |
| Tracheostomy care | -Suctioning the airway to remove secretions -Cleaning around stoma -Changing ties -Inner cannula care |
| Accidental dislodging of tracheostomy | -Immediately replace tube -Spread opening with retention sutures grasped or hemostat -Obturator inserted in replacement tube: Lubricated with saline poured over tip Inserted at 45 degrees to neck |
| Nursing Diagnoses | -Ineffective airway clearance -Impaired verbal communication -Risk for infection -Impaired swallowing -Ineffective therapeutic regimen management |
| Techniques to promote speech | -Spontaneously breathing patient may deflate cuff, allowing exhaled air to flow over vocal cords -Patient on mechanical ventilation can allow constant air leak around cuff |
| Decannulation | -When patient can adequately exchange air and expectorate -Stoma closed with tape and covered with occlusive dressing -Instruct patient to splint stoma with fingers when coughing, swallowing, or speaking -Tissue forms in 24 to 48 hours -Opening will close in several days without surgical intervention |
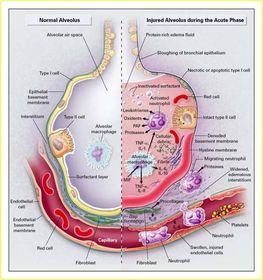
| Acute Respiratory Distress Syndrome (ARDS) | -Sudden failure of the respiratory system -Extensive lung inflammation and small blood vessel injury. -Alveolar capillary membrane becomes damaged and more permeable to intravascular fluid -Alveoli fill with fluid -Stiff, wet or shock lung |
| ARDS is characterized by | -Severe dyspnea/Tachypnea -Hypoxia/Hypoxemia -Decreased lung compliance -Alveolar Collapse -Diffuse pulmonary infiltrates |
| ARDS etiology & pathophysiology | Develops from a variety of direct or indirect lung injuries (some fall under both) |
| Direct mechanisms of ARDS | Direct mechanisms: -Pneumonia -Sepsis -Chest Trauma -Aspiration of gastric contents -Toxic inhalation/Smoking -Pulmonary contusion or PE -O2 toxicity -Near-drowning -Radiation -Reperfusion injury post-lung transplant |
| Indirect mechanisms of ARDS | Triggered from outside the lung through the release of tissue damaging inflammatory cytokines that travel to the lungs. |
| Indirect mechanism of ARDS (cont) | -Most common is SEPSIS -General Trauma -Massive transfusion-Fluid Resuscitation -Pancreatitis -Drug OD -Burns -DIC -Shock |
| Injury or Acute Exudative phase of ARDS | -1 to7 days (usually 24-48 hours) after direct lung injury or host insult. Release of Inflammatory Mediators -Permeability: Damage to the alveolar capillary endothelial cells and alveolar epithelial cells. Begin collapsing. -Proteinaceous fld. Floods alveoli and inactivates surfactant. -Normal gas exchange is compromised triggering diffuse alveolar collapse. V/Q mismatch & Shunting -Worsening hypoxemia that doesn’t respond to supplemental O2. |
| Reparative of proliferative phase of ARDS | -Last up to 1-2 weeks -Influx neuts, monos, & lymphs, & fibroblasts. -Marked by resolution of acute phase & initial repair of the lung OR pt worsens. -Severe Hypoxemia -A patient who reaches this phase may recover fully, or move on to the fibrotic phase. -Of Note: Within 7-10 days, ½ ARDS pts are either deceased or weaned off Rx. |
| Fibrotic or chronic/late phase | -2 to 3 weeks post initial insult -Fibrotic tissue replaces normal lung structure, scarring. -Causes progressive vascular occlusion & pulmonary hypertension -Require long-term support, mechanical ventilation & supplemental O2 |
| Lasting effects of ARDS | -Acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) are potentially lethal complications of critical illness that are unfortunately common in some ICUs. -Impaired physical, mental, & lung fxn @ 1 yr. -The longer the length of stay, the worse physical fxn. |
| Recognizing ARDS | -Who’s @ Risk? Everybody -Assessment findings similar to those with -Respiratory failure. -If on vent—increasing PIP -Difficulty oxygenating & CXR |
| How do you know its ARDS | -ABGs: Initial - Hypoxemia & respiratory alkalosis 2° to hyperventilation, then respiratory acidosis -Pulse Ox ↓ ↓↓ ↓↓↓↓↓ (Despite how much O2 the Pt is receiving -Labs - FULL PANEL OF EVERYTHING!!! |
| ARDS Tx options | -No definitive treatment currently exists, so………Supportive -Mechanical Ventilation /PEEP/?Nitric Oxide -Medications: Sedation, Chemical Paralysis -Nutrition -On Guard Against Complications – MODS -Positioning: Prone |
| Prone positioning in ARDS | -Repositioning of patient from a supine or lateral prone position to prone position -Goal is improved lung recruitment -Used as supportive therapy in critically ill patients with acute lung injury or ARDS |
| Proning | -Must happen early. -Device/Bed -Inclusion: inadequat oxygenation at ≥ 50% FIO2, PEEP > 10cm, presence of bilateral infiltrates on CXR. -Minimize pressure → Nosocomial -Breakdown -Other Risks |
| True or False? I should reactive alarms before leaving the room? | TRUE |
| When should trach care be performed? | 24 hours after the trach has been inserted, then once a shift |
| What might you expect when progressive vascular occlusion & pulmonary hypertension occurs in the fibrotic or chronic/late phase of ARDS? | Patients will have major limitations with their ADL's, so cor pulmonale and DVTs/PE |
| What do you need to monitor to make sure your patient is hemodynamically stable? | BP & urine output |
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.