18393297
| Question | Answer |
| Name of the central depression of the head of the femur. | Fovea capitis femoris |
| Coxa valga is angle of inclination ______- | Larger than 125 deg |
| Coxa vara is angle of inclination _______. | Less than 115 deg |
| Femoral anteversion is excessive when anterior antetorsion is ________ | More than 25 - 30 deg |
| Femoral retroversion is excessive if anterior antetorsion angle is ______. | Less than 10 deg. |
| What is the name of the Y ligament? | Iliofemoral ligament |
| Attachment sites of the iliofemoral ligament | 1. AIIS 2. distal and proximal aspect of intertrochanteric line. |
| What does the iliofemoral ligament prevent? | 1. Both bands: extension and ER. 2. superior band: adduction 3. inferior band: abduction |
| What does the pubofemoral ligament restrict? | Extension, ER, abduction. |
| Which ligament forms the posterior aspect of the hip ligament complex? | Ischiofemoral ligament |
| Which movements does the ischiofemoral ligament restrict? | 1. IR 2. abduction 3. extension |
| Blood supply for: 1) proximal femur 2) femoral head 3) acetabulum | 1) proximal femur: medial and lateral femoral circumflex 2) femoral head: small branch off obturator artery 3) acetabulum: branches from superior and inferior gluteal arteries |
| Normal gait requirement for hip ROM: | 1. 30 deg flex 2. 10 deg ext 3. 5 deg abd/add/IR/ER |
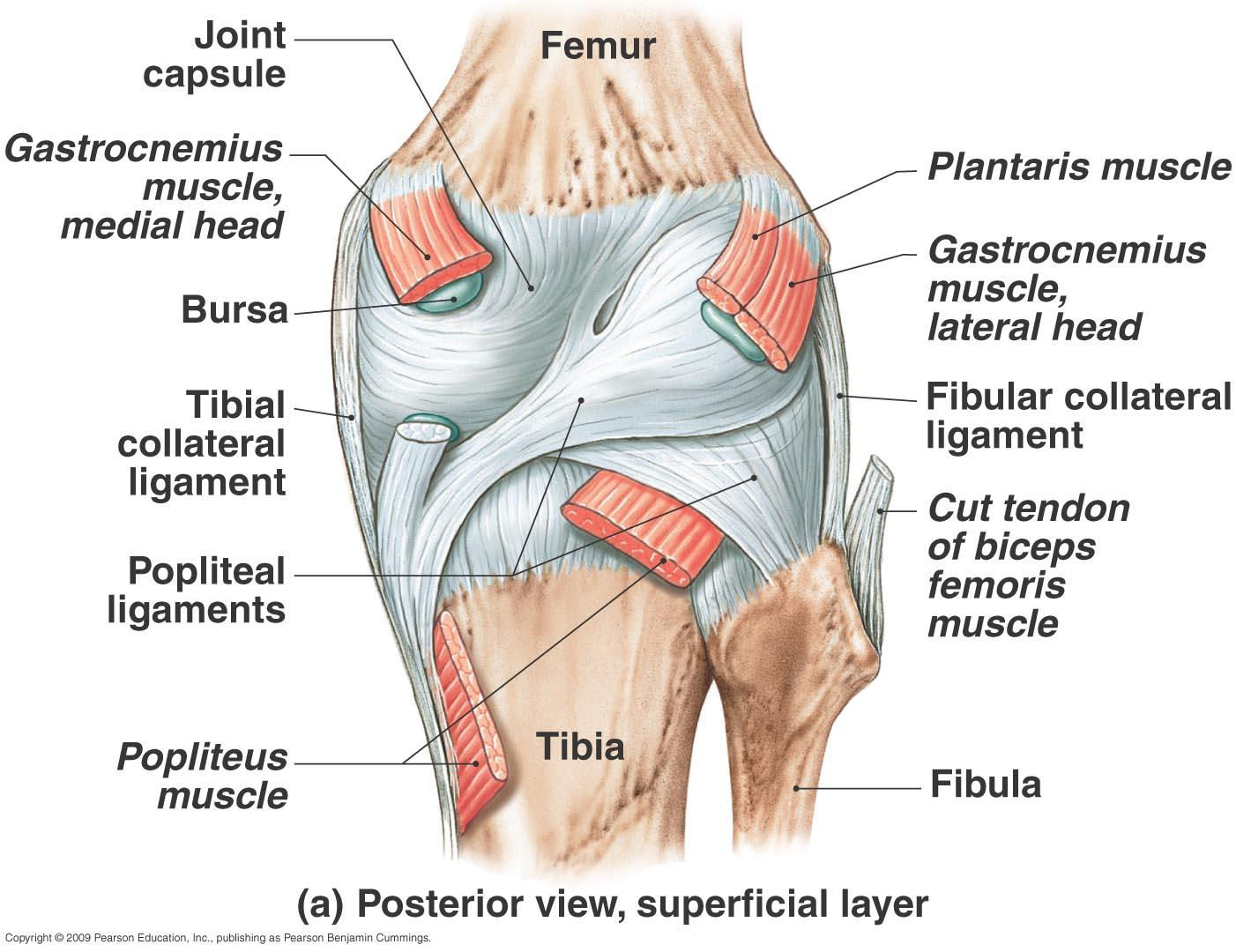
| Locate the oblique and arcuate popliteal ligaments. | |
| T/F:Both the medial meniscus and lateral meniscus are attached to their respective collateral ligaments. | F. The medial meniscus is attached to MCL. However, lateral meniscus and LCL are separated by popliteus muscle tendon. |
| T/F: Meniscus move opposite to the tibia during rotation. | T. (follows femoral condyle) |
| During knee flexion, the medial meniscus is pulled (anteriorly/posteriorly) by the _______. During extension, it is pulled (anteriorly/posteriorly) by the _______. | Flexion: posteriorly, by semimembranosus. Extension: anteriorly, by the medial meniscopatellar ligament |
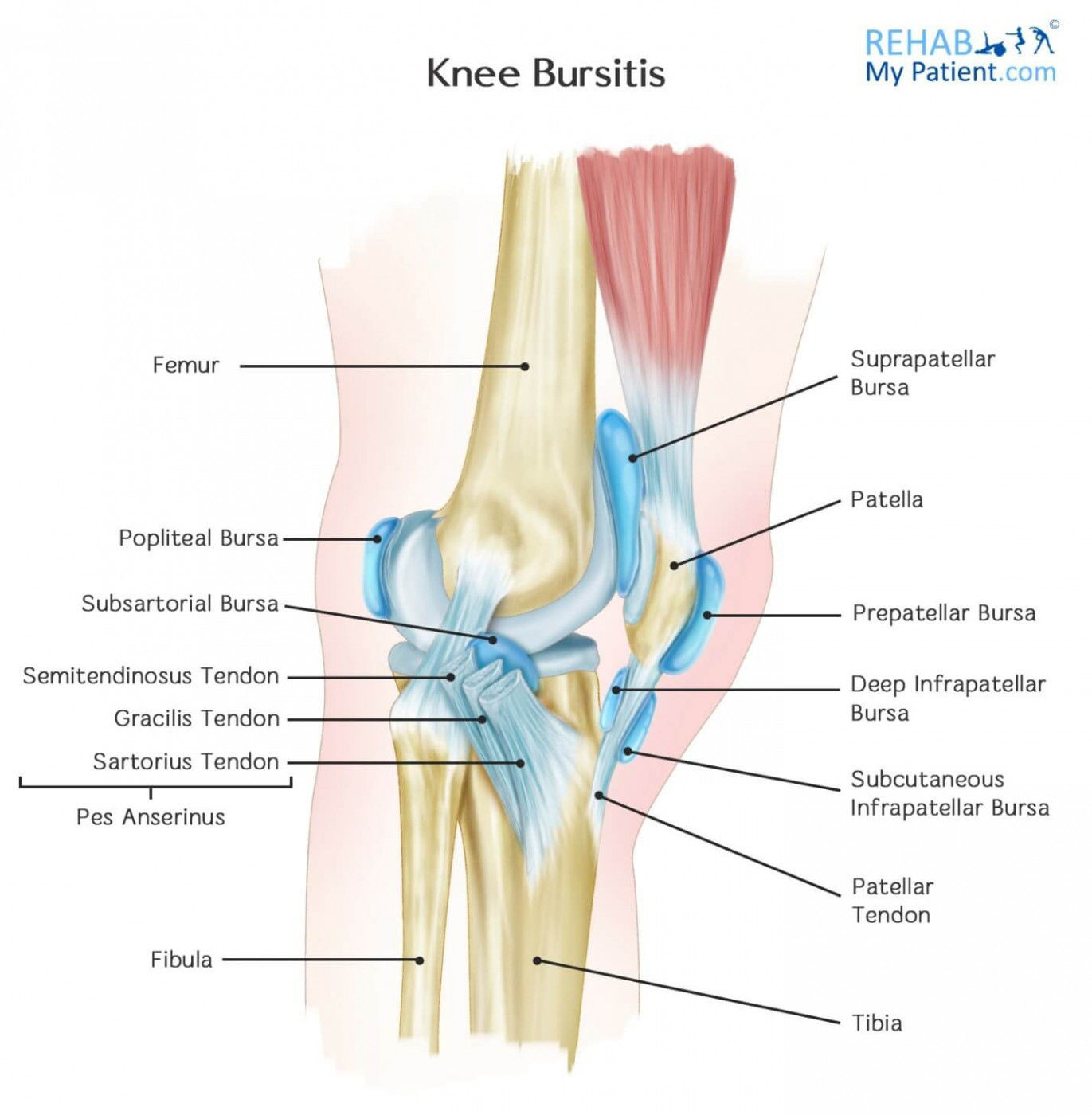
| Name the knee bursae. | |
| The blood supply for the knee bursae | 1. descending branch of the deep femoral artery 2. genicular branches off of the popliteal artery 3. recurrent branch of the deep femoral artery |
| Screw home mechanism is described as _________ in open chain and ______ in close chain during the last ____ of knee extension. | Open chain: tibial ER Close chain: femoral IR Last 5 deg of knee extension |
| Which muscle helps to unlock the knee after terminal extension? | Popliteal muscle |
| Proximal tibiofibular joint: What happens during ankle DF? | 1. fibular shaft rotates externally 2. fibular head glides superiorly and posteriorly |
| Proximal tibiofibular joint: What happens during ankle PF? | 1. fibular shaft rotates internally 2. fibular head glides inferiorly and anteriorly |
| Hip ROM: 1. flexion 2. extension 3. abduction 4. adduction 5. ER 6. IR | 1. flexion: 110 - 120 2. extension: 10 - 15 3. abduction: 30 -50 4. adduction: 30 5. ER: 40 - 60 6. IR: 20 - 30 |
| Knee ROM: 1. flex 2. extension 3. ER 4. IR | 1. flex: 135 2. extension: 0 - 15 3. ER: 30 - 40 4. IR: 20 - 30 |
| Special tests for hip intra-joint pathology. | 1. scour 2. FABER 3. FADIR |
| Special tests for hip muscle length 1. hip flexor 2. TFL and ITB 3. Rectus Femoris 4. Hamstring 5. Piriformis | 1. Thomas test 2. Ober test 3. Prone knee bend (Ely's test) 4. 90-90 hamstring 5. Piriformis test |
| Tests for anterolateral instability of the knee? | Pivot shift test. |
| Which test will be positive if the patient has IT band compression? | The noble compression test |
| List the criteria for Ottawa Knee Rules | 1. knee injury age 55+ 2. isolated patellar tenderness 3. fibular head tenderness 4. unable to flex knee >90 deg 5. unable to weight bear immediately after the injury or in the ER. |
| What is the ROM limitation pattern for patients with hip avascular necrosis? | flexion, IR, abduction |
| Diagnosis of femoroacetabular impingement syndrome (FAI) include the following: 1. (anterior/posterior) groin pain reproduced by FADIR or FABER 2. Hip (IR/ER) less than 20 deg at 90 hip flexion. 3. popping/snapping 4. Imaging findings for _______. | 1. anterior groin pain 2. IR less than 20 deg at 90 hip flexion 4. CAM or pincer |
| Action of piriformis: IR at _____ hip flexion. ER at _____ hip flexion. | ER at <60 hip flexion IR at >90 hip flexion |
| Which one is CAM and which one is pincer? 1. Femoral head too big 2. Acetabular too small | 1. CAM 2. pincer |
| How do we classify degrees of ligamentous tear in the knee? | 1. first degree: little or no instability 2. second degree: minimal to moderate instability 3. third degree: extreme instability |
| Another test for meniscal tear, other than McMurray? | Apley's test. (patient prone with 90 deg knee flexed. traction with IR, ER, then compression with IR, ER) |
| Following ACL reconstruction, when should ressitance training begin, which muscle is the main target, and what type of exercises? | 1. NMES up to 6-8 weeks, voluntary quad exercises starting within 4-5 weeks and up to 10 months 2. quad muscle is main target 3. can be concentric or eccentric, weight-bearing or non-weight-bearing. |
| Other than ther-ex and NMES, which other treatment is strongly recommended by the CPG? | Neuromuscular re-education. (level 1) |
| According to the CPG, how long should immobilization be after ACL reconstruction, and what is the goal? | within 1 week of reconstruction. goals are 1) pain prevention, 2) increase ROM, 3) avoid adverse soft tissue response |
| Is ice recommended immediately after ACL reconstruction? | Yes. |
| When should weight-bearing start after ACL reconstruction? | within 1 week. (with knee bracing) |
| What are the following outcome measures for? 1. SF-36 2. knee QoL questionnaire 3. KOOS | 1. quality of life 2. QoL specific to knee injuries 3. Knee Injuries and Osteoarthritis Outcome Score |
| Following meniscal repair, stepwise progression of weight-bearing should reach full WB at what time? | 6-8 weeks post surgery. |
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.