6085779
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
over 7 years ago
|
|
| Question | Answer |
| 1535 Explain the CURB-65 score. | C = new onset confusion U = urea =/> 7mmol/L R = RR >30 B = BP <90 systolic or <60 diastolic Aged =/>65 One point for each. |
| 1535 List appropriate empiric ABx Rx for CAP. | Low severity (CURB-65 0-1) = Doxycycline PO 200mg STAT then 100mg OD. Duration 5-7/7. Moderate - severe (CURB-65 2-5) = Benzyl Penicillin IV 1.2g, 4-hrly + Doxycycline PO 200mg STAT then 100-200mg OD (use Clarithromycin IV 500mg, 12-hrly if unable to take oral). Oral switch: Amoxycillin 500mg –1g, 8-hrly +/- Doxycycline PO 200mg STAT then 100mg OD. Duration: 7-10/7 in total. From GB. |
| 1535 List appropriate empiric ABx Rx of infective exacerbation of COPD. | Doxycycline PO 200mg STAT then 100mg OD (or Amoxicillin IV 1g 8-hrly if severe/unable to take orally). Oral switch: Doxycycline PO 200mg STAT then 100mg OD. Duration: 5-7/7. From GB. |
| 1535 List appropriate empiric ABx Rx of uncomplicated UTI. | Trimethoprim PO 200mg, 12-hrly. Duration: women 3/7. Men 7/7. From GB. |
| 1535 List appropriate empiric ABx Rx for soft tissue infxn/cellulitis. | Non-severe: Flucloxacillin PO 500mg, 6-hrly. Duration: 7/7. Severe: Flucloxacillin IV 2g, 6-hrly. Oral switch: Flucloxacillin 500mg –1g, 6-hrly OR Clindamycin 450-600mg 6-hrly. Review IV after 5-7/7 depending on response. From GB. |
| 1537 Take a history of antibiotic allergy. | Taking a history of Penicillin allergy. What to Ask? 1. What antibiotics has the patient reacted to in the past? 2. What antibiotics has the patient taken and tolerated since the allergy diagnosis? 3. What was the nature of the reaction? 4. If rash then: a. Describe nature of rash (e.g. pustular, urticarial etc) b. Could rash be related to underlying condition(e.g. viral) c. How long after commencing antibiotic did rash appear? 5. Why was the patient taking the antibiotic? 6. Did this reaction result in hospitalisation? 7. Did the reaction resolve on stopping the antibiotic? From: http://www.nhstaysideadtc.scot.nhs.uk/Antibiotic%20site/pdf%20docs/Penicillin%20Allergy%20Guidance%20Update%202013%20v4.pdf |
| 1538 Define: adverse drug reaction, drug allergy, anaphylaxis, immediate, accelerated, & late onset reactions, early onset reactions. | Adverse Drug Reaction is a response to a drug which is noxious and unintended and which occurs at doses normally used in man for prophylaxis, diagnosis or therapy of disease or for the modification of physiologic function. Drug allergy is an immunolgically mediated reaction that exhibits specifically and recurrence on re-exposure to the offending drug. A Drug Allergy is a form of Adverse Drug Reaction. Anaphylaxis is a severe, potentially fatal, systemic allergic reaction that occurs suddenly after contact with an allergy-causing substance. Immediate Onset Reactions (Type 1) occur within 1 hour of administration of the drug. These are IgE mediated reactions and may progress to anaphylaxis. Accelerated Onset Reactions occur between 1 and 72 hours of administration of drug. These are almost always IgE mediated reactions. Early Onset Reactions is a collective term used to describe Immediate and Accelerated Onset Reactions. Late Onset Reactions occur beyond 72 hours of administration of the drug. From: as previous slide. |
| 1540 Explain synergy in the context of antibiotics. | Drug synergy occurs when drugs can interact in ways that enhance or magnify one or more effects, or side-effects, of those drugs (e.g. two different antibiotics like a penicillin and an aminoglycoside; penicillins damage the cell wall of gram-positive bacteria and improve the penetration of aminoglycosides). From Wikip. |
| 1542 Describe how clostridium difficile diarrhoea occurs and how it is diagnosed and Rx. | C. diff produces two toxins - A (enterotoxin adheres to the intestinal epithelium without damaging it and induces excessive fluid secretion leading to watery diarrhoea) & B (cytotoxic - damages the intestinal epithelium leading to dysentery). Dx - stool samples to detect toxins using ELISA or PCR. Rx - metronidazole (mild - moderate), oral vancomycin (severe or relapsing). Often causes illness following ABx Rx that has removed bowel commensals or in debillitated pt's. Stop ABx's if possible. K & C p122. |
| 1544 Describe the MOA of penicillin. | Penicillins inhibit the enzymes responsible for cross-linking peptidoglycans in bacterial cell walls. This weakens cell walls, preventing them from maintaining an osmotic gradient. Uncontrolled entry of water into bacteria causes cell swelling, lysis and death. Penicillins contain a β-lactam ring, which is responsible for their antimicrobial activity. Side chains attached to the β-lactam ring can be modified to make semi-synthetic penicillins. The nature of the side chain determines the antimicrobial spectrum and other properties of the drug. T 100 D p174. |
| 1544 Describe the MOA of metronidazole. | Metronidazole enters bacterial cells by passive diffusion. In anaerobic bacteria, reduction of metronidazole generates a nitroso free radical. This binds to DNA, reducing synthesis and causing widespread damage, DNA degradation and cell death. As aerobic bacteria are not able to reduce metronidazole in this manner, the spectrum of action of metronidazole is restricted to anaerobic bacteria (and protozoa). T 100 D p146. |
| 1549 Explain why Gram negative bacteria may be penicillin resistant. | Bacteria resist the actions of penicillins by making β-lactamase, an enzyme which breaks the β-lactam ring and prevents antimicrobial activity. Other mechanisms of resistance include limiting the intracellular concentration of penicillin (reduced bacterial permeability or increased extrusion) or changes in the target enzyme to prevent penicillin binding. T 100 D p174. |
| 1550 Explain the MOA of cephlosporins. | Their antimicrobial effect is due to their β-lactam ring. During bacterial cell growth, cephalosporins and carbapenems inhibit enzymes responsible for cross-linking peptidoglycans in bacterial cell walls. This weakens cell walls, preventing them from maintaining an osmotic gradient, resulting in bacterial cell swelling, lysis and death. Both types of antibiotic have a broad spectrum of action. Cephalosporins and carbapenems are naturally more resistant to β-lactamases than penicillins due to fusion of the β-lactam ring with a dihydrothiazine ring (cephalosporins) or a unique hydroxyethyl side chain (carbapenems). T 100 D p94. |
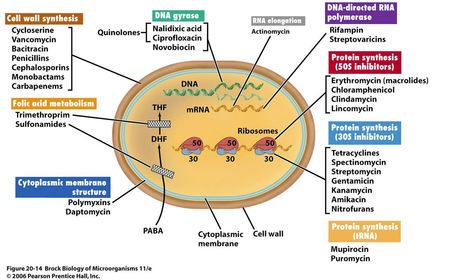
| 1551 Outline how antibiotics work at the cellular level. |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.