6414282
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
over 7 years ago
|
|
| Question | Answer |
| 4098 Define delirium. How does it differ from conditions such as dementia? | Delirium - a functional brain disorder characterised by clouding of consciousness & impaired cognitive function, which develops over hours or days, & typically fluctuates over the course of the day. MAAG p167. Dementia is a clinical syndrome with multiple causes which is usually progressive. Defined by: * An acquired loss of higher mental function, affecting two or more cognitive domains including: – Episodic memory – usually involved – Language function – Frontal executive function – Visuospatial function – Apraxia or agnosia * Of sufficient severity to significantly cause social or occupational impairment * Occurring in clear consciousness (to distinguish it from delirium). K & C p1137. |
| 4099 DDx for pt's presenting with delirium (acute confusion). | * Systemic infxn: > Any infxn, esp with ^fever (eg malaria, sepsis) * Metabolic disturbance: > Hepatic failure > CKD > Electrolyte imbalance/dehydration > Hypoxia * Vitamin deficiency: > Thiamine (Wernicke-Korsakoff syndrome, beriberi) > Nicotinic acid (pellagra) > Vit B12 * Endocrine DS: > Hypothyroidism > Cushing's syndrome * Intracranial causes: > Trauma > Tumour > Abscesses > Subarachnoid haemorrhage > Epilepsy * Drug intoxication: > Anticonvulsants > Antimuscarinics > Anxiolytics/hypnotics > Tricyclic antidepressants > Dopamine agonists > Digoxin * Drug/alcohol withdrawal * Postoperative states. K & C p1188. |
| 4100 Give a DDx for dementia. | * Degenerative > Alzheimer's > Dementia with Lewy bodies > Frontotemporal dementia > Huntington's DS > Parkinson's DS > Prion DS's - eg Creutzfeldt-Jakob * Vascular > Vascular dementia > Cerebral vasculitis (rare) * Metabolic > Uraemia > Liver failure * Toxic > Alcohol > Solvent abuse > Heavy metals * Vitamin deficiency - B12 & thiamine * Traumatic * Intracranial lesions > Subdural haematoma > Tumours > Hydrocephalus * Infxn > HIV > Neurosyphilis > Whipple's DS > TB * Endocrine > Hypothyroidism > Hyperparathyroidism * Psychiatric K & C p1139. |
| Although the cause of alzheimer's DS (AD) is still not known, a great deal is now understood about the molecular pathology of AD. The pathological hallmarks are the deposition of β..... in a..... plaques in the cortex and formation of t..... containing intracellular n..... tangles. These protein aggregates damage synapses and ultimately lead to neuronal death. | Although the cause of AD is still not known, a great deal is now understood about the molecular pathology of AD. The pathological hallmarks are the deposition of β-amyloid in amyloid plaques in the cortex and formation of tau-containing intracellular neurofibrillary tangles. These protein aggregates damage synapses and ultimately lead to neuronal death. K & C p1139. |
| 4106 Multi-infarct dementia - multiple large infarcts, once they reach a certain volume and affect a large enough number of individual brain regions, will exhaust the brain's c..... mechanisms and lead to dementia. However, small infarcts in strategic areas such as the b..... g..... and t..... can also lead to dementia with only a small volume of brain having been infarcted. Most of these small infarcts - that is, <1.5 cm in size (l..... infarction) - are caused by a...... of the small irrigating superficial and deep penetrating arteries and arterioles. The underlying cause is thought to be secondary to ..... The basal ganglia, thalamus, pons, internal capsule, and deep white matter areas are maximally affected. | Multiple large infarcts, once they reach a certain volume and affect a large enough number of individual brain regions, will exhaust the brain's compensatory mechanisms and lead to dementia. [9] However, small infarcts in strategic areas such as the basal ganglia and thalamus can also lead to dementia with only a small volume of brain having been infarcted. [5] Most of these small infarcts - that is, <1.5 cm in size (lacunar infarction) - are caused by arteriosclerosis of the small irrigating superficial and deep penetrating arteries and arterioles. The underlying cause is thought to be secondary to HTN. The basal ganglia, thalamus, pons, internal capsule, and deep white matter areas are maximally affected. |
| 4107 Distinguish cortical & sub-cortical dementias & give examples of each. | Dementia can be split into two groups based on which part of the brain is affected: * Cortical dementias happen because of problems in the cerebral cortex. They play a critical role in memory & language. People with these types of dementia usually have severe memory loss and can't remember words or understand language. Alzheimer's and Creutzfeldt-Jakob disease are two forms of cortical dementia. * Subcortical dementias happen because of problems in the parts of the brain beneath the cortex. People with subcortical dementias tend to show changes in their speed of thinking & ability to start activities. Usually, people with subcortical dementia don't have forgetfulness & language problems. Parkinson's disease, Huntington's disease, & HIV can cause these types of dementia. Some types of dementia affect both parts of the brain. http://www.webmd.com/brain/types-dementia#1 |
| 4108 Describe investigations used to confirm dementia & look for treatable causes. | Diagnosis is primarily clinical. * Sx: personality change / nocturnal wanderings / reversed day-night sleep cycle / intellectual decline / mood change -> Suspected dementia -> * Hx & examination -> * Important tests @ BD tests: FBC / ESR / vitB12 / U & E's / glucose / liver biochem / serum Ca2+ / TSH, T3, T4 / HIV serology @ Imaging: CT / MRI @ Other for selected pt's: CSF inc tau & A-beta42 / genetic studies eg AD genes, Huntington's DS, prion mutations / EEG / brain biopsy -> * Tests for mental cognition eg MMSE, Addenbrooke's Cognitive Examination. K & C p1138 & MAAG p430. |
| 4109 Outline the Mx of pt's with dementia. | * Enlist a care coordinator via Social Services or Community Mental Healthcare Team * Capacity - where possible allow pt to guide decisions. Suggest making an advanced directive or appointing a Lasting Power of Attorney. * Develop routines - ie putting things in the same place * Plan ahead - eg move house sooner rater than later * Use day services to provide stimulus for pt's & give carers respite * Care for the carers - provide contacts for support groups eg UK AD Society * Challenging behaviour - rule out P & infxn then consider trazadone, lorazepam, or haloperidol * Depression is common - try an SSRI or mirtazipine (if severe). CBT may help. * Avoid drugs that impair cognition - eg neuroleptics, sedatives, tricyclics. |
| 4110 Outline the MOA & role in Rx of drugs developed to treat the cognitive defect in AD. | * Cholinesterase inhibitors (donepezil, rivastigmine, galantamine) ^acetylcholine levels by inhibiting CNS acetylcholinesterase. * NMDA receptor antagonist (memantine) - used in moderate-severe AD or where cholinesterase inhibitors aren't tolerated. K & C p1141. |
| 4102 Seizures are divided by clinical pattern into two main groups – partial seizures & generalized seizures. A partial (f.....) seizure is caused by electrical d..... restricted to a limited part of the cortex of ..... cerebral hemisphere. Partial seizures are further sub-divided according to whether or not there is loss of a.....: – simple partial seizures – without loss of a....., e.g. one limb jerking (a Jacksonian seizure). – complex partial seizures – with loss of a....., e.g. a temporal lobe seizure. In generalized seizures, there is simultaneous involvement of both h....., always associated with loss of c..... or a..... | Seizures are divided by clinical pattern into two main groups – partial seizures & generalized seizures. A partial (focal) seizure is caused by electrical discharge restricted to a limited part of the cortex of one cerebral hemisphere. Partial seizures are further sub-divided according to whether or not there is loss of awareness: – simple partial seizures – without loss of awareness, e.g. one limb jerking (a Jacksonian seizure). – complex partial seizures – with loss of awareness, e.g. a temporal lobe seizure. In generalized seizures, there is simultaneous involvement of both hemispheres, always associated with loss of consciousness or awareness. K & C p1111. |
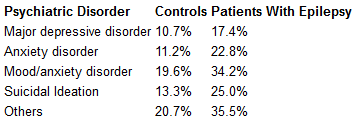
| 4103 Outline the psychiatric manifestations of epilepsy. | It is estimated that 20-30% of patients with epilepsy have psychiatric disturbances. Of patients with intractable complex partial seizures, 70% may have 1 or more diagnoses consistent DSM-III-R; 58% of these patients have a history of depressive episodes, 32% have agoraphobia without panic or other anxiety disorder, and 13% have psychoses. The risk of psychosis in patients with epilepsy may be 6-12 times that of the general population, with a prevalence of about 7-8%; in patients with treatment-refractory temporal lobe epilepsy, the prevalence has been reported to range from 0-16%. The most common psychiatric conditions in epilepsy are depression, anxiety, and psychoses. medscape.com |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.