6841925
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
over 7 years ago
|
|
| Question | Answer |
| Stroke, causing acute loss of vision, is usually an occlusion of which arteries? | Vertebral, basilar, posterior cerebral, occipital cortex. From lecture notes: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
| What patterns of visual loss are typically seen in stroke? | Bilateral, hemianopic, +/- macular sparing. K & C p1099 & https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
| GCA - what is it? S & Sx? | * Inflammatory arteritis of large cerebral arteries (occurs in association with PMR - 50%) * Occular emergency as can affect opthalmic artery leading to sudden loss of vision * Usually affects >50 YO * Sx: > +++ Headache > Scalp/temple tenderness > Jaw claudication * OE there may be RAPD, pale swollen disc, pale ischaemic retina K & C p543 & https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
| Ix & Rx of GCA. | * Start Rx before Ix - remember possibility of vision loss! * Prednisolone PO 60-80 mg or methylprednisolone IV 0.5-1.0 g * BD's - ^CRP & ESR (ESR may be normal in 20%), platelets often^ * Temporal artery biopsy - definitive Ix but time consuming & can get false -ve * Long term - prednisolone needs to be tapered over 12-18/12. Beware SE's - osteoporosis, DM, HT, infxn (co-prescribe bone & gastric protection). K & C p543 & https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
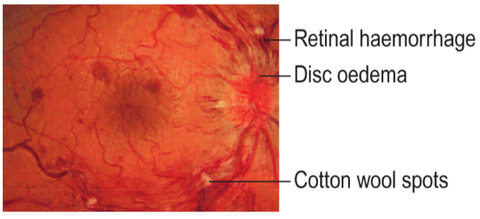
| Central retinal vein occlusion - who gets it, S & Sx, & Rx. | * Thrombus of central retinal vein obstructs outflow of BD -> ^intravascular pressure. * Dilated veins, retinal haemorrhage, cotton wool spots, retinal oedema (see following slide). * Sudden, painless, monocular vision loss ('like a curtain closing' - occuring in seconds). * Risk factors - age (>60 YO), HT, CVD, DM, glaucoma, hypercoagulability. * Rx - anti-VEGF, retinal laser. From lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
| Central retinal vein occlusion. K & C p1063 | |
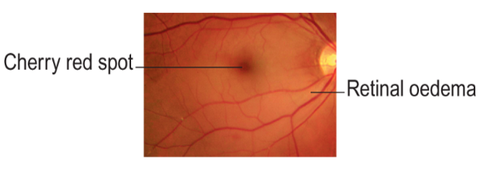
| Central retinal artery occlusion (CRAO) - who gets it, S & Sx, & Rx. | * CRAO -> arteries narrowed, retina becomes opaque & oedematous, cherry red spot seen over fovea, usually RAPD (see following card). * Arteriosclerotic emboli (HT/carotids) most common cause. * Sudden, painless, monocular vision loss ('like a curtain closing' - occuring in seconds). * Temporary CRAO = retinal TIA (aka amaurosis fugax). * Need to rule out GCA - esp in >60 YO. * No proven Rx. * Stroke/TIA work-up. K & C p1063 & https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
| Central retinal artery occlusion. K & C p1063. | |
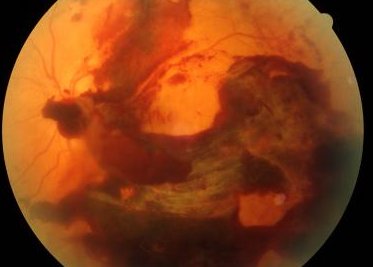
| What are some causes of vitreous haemorrhage? S & Sx? | May be secondary to: * Trauma * Proliferative retinopathy - esp diabetic, also other causes of neovascularisation - eg occlusions. * Retinal tear/detachment - may rupture BD vessels. S & Sx: * Painless monocular loss of vision - 'all blurry/hazy'. * Often starts as floaters/blobs. * Absent red reflex, poor/no fundal view, no RAPD. From lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
| Ix & Rx of vitreous haemorrhage. | * USS of eye to check retina flat/without tears * Usually self-resolving in 6-8/52 * If non-resolving then virectomy * If recurrent in proliferative diabetic retinopathy then retina may need fully lasering From lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
| Vitreous haemorrhage. | |
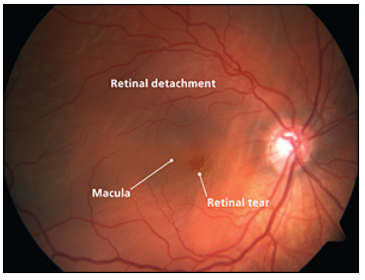
| What is the most common cause of retinal detachment? S & Sx & Rx? | Posterior vitreous detachment (PVD)- with age the vitreous becomes liquified, lacunae appear which reduce shock absorption. Vitreous collapses. * PVD Sx: * Floaters & flashes (retinal stimulation from traction) 10% develop a tear which can then allow fluid behind the retina causing detachment (RD). RD Sx: * Black curtain/loss of vision progressing across visual field over hours to days. Blindness if not Rx. Risk factors: * Myopia * Trauma * Inflammation * Connective tissue disorders OE: * Field loss * RAPD * Visible detachment on fundoscopy Rx: * Retinal surgery - vitrectomy/cryotherapy/gas From lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Ophthalmology+notes.pdf |
| Retinal tear. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.