7374928
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
over 7 years ago
|
|
| Question | Answer |
| Inflammatory process with cascade of release of inflammatory cytokines (TNFA, IL2, IL6, platelet-activating factor (PAF)) & pancreatic enzymes (trypsin, lipases, co-lipases) initiated by pancreatic injury, but which may develop into full blown MODS or SIRS. OHOCS | Inflammatory process with cascade of release of inflammatory cytokines (TNFA, IL2, IL6, platelet-activating factor (PAF)) and pancreatic enzymes (trypsin, lipases, co-lipases) initiated by pancreatic injury, but which may develop into full blown MODS or SIRS OHOCS |
| Causes of acute pancreatitis. | * Gallstones (60%) * Alcohol (30%) * Hyperlipidaemia * Hypercalcaemia (hyperparathyroidism, multiple myeloma) * Direct damage (trauma, ERCP, post-SX, cardiopulmonary bypass) * Toxins: > Drugs eg azathioprine, oestrogens, thiazides, isoniazid, steroids, NSAID's * Infxn eg viral (mumps, CMV, HBV), mycoplasma * Venom (scorpion, snake bites) * Idiopathic |
| Clinical features of acute pancreatitis. | * Severe epigastric P radiating to the back * Severe N & V * Fever, dehydration, hypotension, tachycardia (may be frankly shocked) * Epigastric tenderness associated with guarding & in severe cases, rigidity which may be generalized * L flank ecchymosis (Grey–Turner's sign) & periumbilical ecchymosis (Cullen's sign), 1–3% of cases haemorrhagic pancreatitis OHOCS |
| Classification/complications of acute pancreatitis. | * Oedematous (70%). May be simple or associated with phlegmon ('noninfected solid mass of inflamed pancreatic & retroperitoneal tissues') formation; transient fluid collections common. * Severe/necrotizing (25%). Necrosis may be sterile or infected. Persistent large peripancreatic fluid collections may form (‘pseudocyst’), which may become infected. * Haemorrhagic (5%) OHOCS |
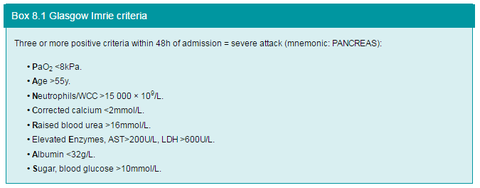
| Emergency Mx/resuscitation of suspected acute pancreatitis. | * Large calibre IV access. Give crystalloid fluid up to 1000mL if tachycardic or hypotensive; may require ongoing fluids IV. * Catheterize & place on a fluid balance chart * BD's - FBC (Hb, WCC), U&E (Na, K), LFT's (bilirubin, albumin), amylase, group & save, clotting * Monitor HR, BP, & urine output (urinary catheter) • Consider central line & Mx pt in HDU if haemodynamically unstable or fails to respond to early resuscitation * Assess the severity of the attack by Glasgow Imrie criteria Box 8.1 Glasgow Imrie criteria |
| Glasgow Imrie criteria. Box from OHOCS. | |
| Ix/Dx of acute pancreatitis. | * Serum amylase >1000U. Diagnostic, but may be normal even in severe cases; ^amylase may occur in a wide range of other acute abdo events (intestinal ischaemia, leaking aneurysm, perforated ulcer, cholecystitis). * Serum lipase. Remains ^longer than serum amylase; more specific, but less sensitive. * AXR (non-specific findings). Absent psoas shadows, ‘sentinel loop sign’ (dilated proximal jejunal loop adjacent to pancreas because of local ileus’), ‘colon cut-off sign’ (distended colon to mid-transverse colon with no air distally); may show gallstone, pancreatic calcification. * CT may be required. Shows pancreatic oedema, swelling, loss of fat planes; may show haemorrhagic or necrotic complications. * US scan. Must be done within 48h of ADx to identify gallstones in bile duct. OHOCS |
| Rx of acute pancreatitis. | * Urgent ERCP & stone extraction for bile duct stones causing obstruction pancreatitis Identify/prevent complications: * IV ABx (eg IV imipenem TDS), sometimes started in moderate-severe cases without evidence of infected necrosis * CT scan identifies development of pancreatic phlegmon, early fluid collections, necrosis, or haemorrhage * CT-guided pancreatic aspiration to identify infected necrosis * Early low volume enteral feeding increasingly used to reduce risk of stress ulceration & bacterial translocation causing sepsis Rx of early complications: * Consider Rx'ing severe cases on HDU/ITU for optimized fluid balance, respiratory, cardiovascular, & renal support * Proven infected necrosis. SX debridement may be required, but is associated with a poor prognosis. * Acute pseudocysts rarely need drainage unless very large OHOCS |
| Chronic pancreatitis - key facts: * Characterized by recurrent or persistent abdo P arising from the pancreas * Often associated with exocrine or endocrine pancreatic insufficiency * Characterized by irreversible destruction & fibrosis of pancreatic parenchyma * May arise following one or more episodes of acute pancreatitis or may be a chronic progressive process de novo OHOCS | Chronic pancreatitis - key facts: * Characterized by recurrent or persistent abdo P arising from the pancreas. * Often associated with exocrine or endocrine pancreatic insufficiency * Characterized by irreversible destruction & fibrosis of pancreatic parenchyma * May arise following one or more episodes of acute pancreatitis or may be a chronic progressive process de novo OHOCS |
| Pathological features of chronic pancreatitis: * May affect all or part of gland (focal) * Head tends to most severely involved part in chronic alcohol DS * Features of acute pancreatitis may occur—oedema, acute inflammatory infiltrate, focal necrosis, intraparenchymal haemorrhage * Chronic inflammatory changes cause progressive disorganization of the pancreas: > Glandular atrophy & duct ectasia > Microcalcification & intraductal stone formation with cystic changes secondary to duct occlusion OHOCS | Pathological features of chronic pancreatitis: * May affect all or part of gland (focal) * Head tends to most severely involved part in chronic alcohol DS * Features of acute pancreatitis may occur—oedema, acute inflammatory infiltrate, focal necrosis, intraparenchymal haemorrhage * Chronic inflammatory changes cause progressive disorganization of the pancreas: > Glandular atrophy & duct ectasia > Microcalcification & intraductal stone formation with cystic changes secondary to duct occlusion OHOCS |
| Causes of chronic pancreatitis. | * Recurrent acute pancreatitis of any cause, especially alcohol * Secondary to pancreatic ductal obstruction: > Pancreatic head cysts, tumours > Pancreatic duct strictures—post-SX, ERCP, parasitic infestation > Congenital pancreatic abnormalities (pancreas divisum, annular pancreas) > Cystic fibrosis * Associated with AI DS's (primary biliary cirrhosis, primary sclerosing cholangitis) * Congenital idiopathic chronic pancreatitis OHOCS |
| Features of chronic inflammation, exocrine, & endocrine failure in chronic pancreatitis. | Chronic inflammation: * Recurrent or chronic abdo P: > Typically epigastric, radiating to back & requiring opiates > ^With food, alcohol Features of exocrine failure: * Anorexia & weight loss (due to protein malabsorption) * Steatorrhoea (due to fat malabsorption) Features of endocrine failure: * Insulin-dependent DM (due to loss of beta islet cells) OHOCS |
| Rx of chronic pancreatitis. | * Prevention of cause/progressive damage: > Stop alcohol, deal with gallstones, Rx AI DS > Encourage a diet rich in antioxidants (vitamins A, C, E, selenium) * Control Sx/complications: > Dietary modifications. Adequate carbohydrates & protein, reduced fat. > Pancreatic exocrine enzyme supplements (e.g. Creon®) > Analgesia > Control of DM often requires insulin Indications for SX Rx: * Rx of reversible cause (anatomical abnormalities, tumours, cysts, ductal strictures & stones). Ops used include those to remove causes & those to drain obstructed duct: > Pancreaticoduodenectomy (Whipple procedure) > Partial pancreatectomy of the head (Frey procedure) or tail (distal pancreatectomy) > Pancreaticojejunostomy (Peustow or Duval procedure) * Rx of severe intractable P or multiple relapses. Ops are usually to resect affected portion: > Partial pancreatectomy of head (Frey procedure) or tail (distal pancreatectomy) > Total pancreatectomy * Complications (pseudocyst, obstruction, fistula, infxn, portal hypertension) OHOCS |
| What risks are associated with resectional SX? | * ^Risk of exocrine & endocrine pancreatic failure * All surgery is associated with a risk of symptom recurrence due to recurrent or progressive DS OHOCS |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.