Description

|
|
Created by Niamh McLoughlin
over 6 years ago
|
|
Page 1
Drug discovery
i) What is drug discovery? Creating new compounds from scratch or isolating them from natural sources... ...testing them in vitro - then on animal models... ...determine their efficacy & safety... ...before advancing them on to clinical trials for human testing! Drug discovery combines the fields of synthetic & natural product chemistry
ii) Why do we need new drugs? Unmet medical needs Tackle new diseases - i.e. AIDS, obesity, CJD Improve on low efficacy rates - dementia & cancer drugs Filter out unwanted/harmful side-effects - antidepressants, antipsychotics Overcome drug resistance - antibiotics Treat diseases earlier so downstream costs for treatment/disease management are lower - Alzheimer's, spinal injuries Cost of therapy - interleukins used in HIV therapy Social costs to individuals/countries - Depression Create employment
Page 2
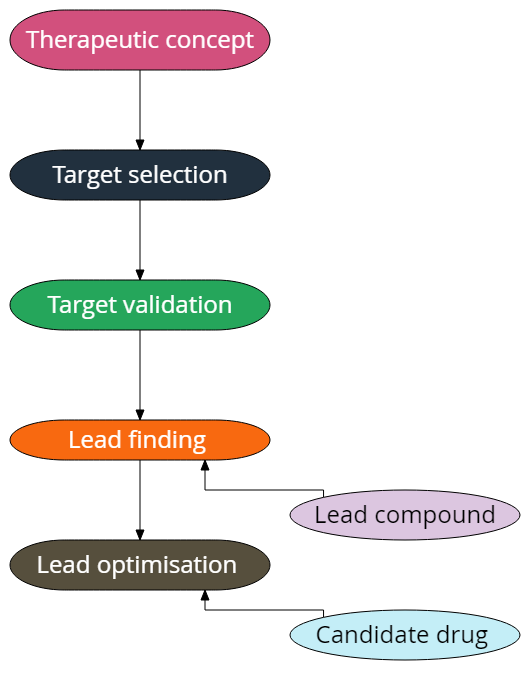
Steps in drug discovery
{kind=link}
{kind=link}
Page 3
Therapeutic concept
Firstly, we define a particular disease with a therapeutic need to be met Examples might include: Alzheimer's disease - improve cognition Schizophrenia - reduce frequency or severity of psychotic episodes HIV - prevent virus from inflitrating cells
Therapeutic concept = Identification of a biochemical, cellular or pathophysiological mechanism in a disease Look at the various levels & stages of our chosen disease to see where the problem/s are occuring Examples: Relationship of a gene mutation with pathology of disease How bacteria/virus/fungus infiltrates cell & destroys it Identifying why the immune system is attacking certain cells/organs
Target selection
Particular molecular target is selected & validated Hone in on specific action we want drug to have Example: Enzyme inhibitors Target DNA Receptor agonists & antagonists
Page 4
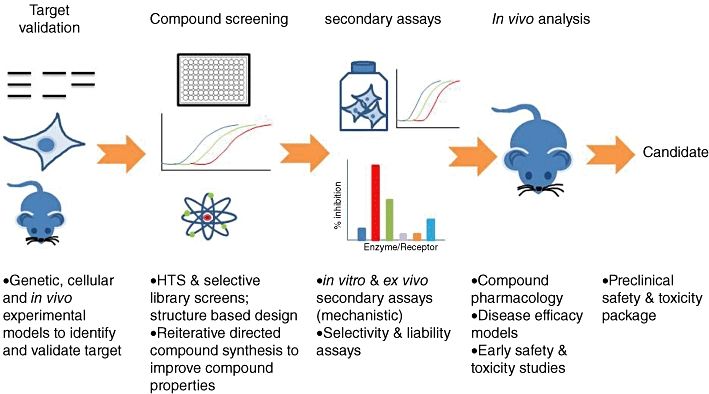
Target validation
i) High throughput screening Used to filter millions of potential compounds into a few hundred 'Hits' are identified through their activity with a particular assay - show specific effects 'Artefacts' are the remaining few hundred drugs - show no specific effects Use 2 different mechanisms: Biochemical assays: Assess protein-protein interactions Provide info on nature of molecular interactions (binding affinity, regions of protein interactions & kinetics) Cannot determine cellular impact - only structure & target (region & site) Cell-based assays: Based on iPS culture Measure features such as: Growth Cell metabolism changes Morphology Changes in 2nd messenger activity CBAs can distinguish agonists & antagonists - biochem cannot
ii) Structure activity relationships (SAR) Relationship between chemical structure of a molecule & its biological activity Useful substructures within the lead series are defined & maintained.... ...whilst other structural features that have no defined purpose are varied/changed Medicinal chemists use chemical synthesis - insert new chemical groups into the compound & test their biological effects
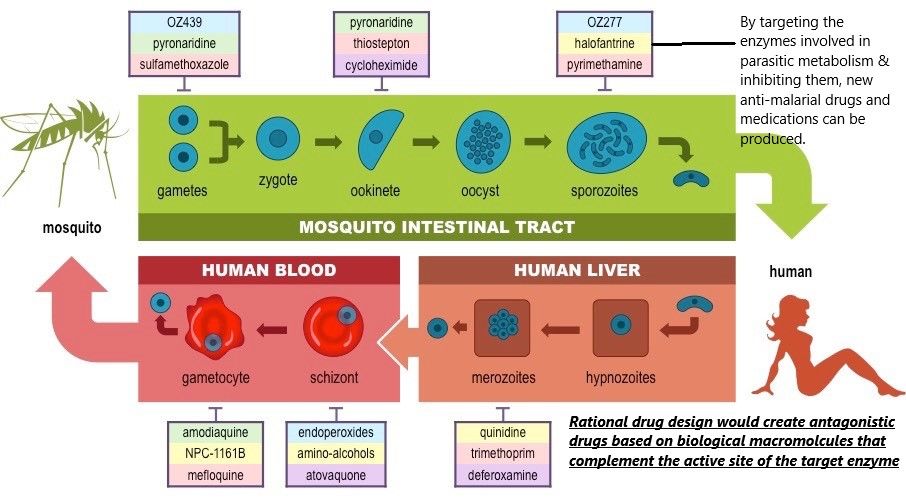
iii) Rational drug design Uses natural endogenous mediator as lead compound & makes modifications (the biological macromolecule implicated in disease pathology acts as a starting point) Based on the idea that modulation of a specific biological target may have therapeutic value Alternative to blindly testing hundreds of molecules to see if one or more will bind to cellular/molecular targets Difficult start point - they're usually too polar & have v high Mr Chemists must: Reduce Mr Reduce number of polar OH groups Eliminate chiral centres 'Me-too' drugs = use pre-existing drugs as a chemical start point Need to make sig. improvements on 'parent' drug (due to patency issues) - needs to have better absorption, pharmacokinetics or receptor affinity
{kind=link}
iv) Structure based design Historically used to make enzyme inhibitors Carried out in 5 steps: X-ray crystal structure of target in its biologically active form is found Ligand is co-crystallised with target protein Ligand analysed to find its binding domain Biological relevance of interactions confirmed by site-directed mutagenesis (changing DNA sequence of gene) Ligand is continually redesigned to optimise interactions
SARS, Rational drug design & Structure-based design eliminate futher artefacts Reduce potential drug list from hundreds down to approx 10 - 'Lead series'
Page 5
Lead finding
Drug metabolism/pharmacokinetic & toxicological properties of remaining potential drugs examined - DMPK & toxcitiy ipS assays ~3 drugs remain in 'lead series' Liver activity assays Liver microsome/hepatocyte survival after drug exposure recorded - drug conc. & effects also noted Lots of SAR info collected Activity CYP450 enzymes assayed to predict drug interactions (allow us predict how drug will interact with P450 enzymes - multiple drug interactions!!) Intestinal absorption assays Drug permeability through Caco-2 cells (Intestinal epithelial cells) Drug applied apical side cell - conc. measured on basolateral side Determines absorption & bioavailability BBB absorption assays in-vitro assays using brain endothelial cells Drug applied blood-facing side of cells - measured on brain side Compound profiling = Drug properties (pharmacoK, toxicity, metab) discovered in target validation & lead finding phase are compiled & catalogued - Other researchers can know properties of specific compounds without needing to re-use assays
Page 6
Lead optimisation
Drug optimisation = key! Want to improve affinity, selectivity & DMPK parameters (plasma 1/2 life, oral bioavailability etc) of leads Want to maintain physiocochemical properties - esp. aqueous solubility Want to make the drug pharmaceutically 'easy-to-make' - intrinsic solubility (solubility @ pH where drug is un-ionised), dissolution rate & stability (want to have long shelf-life, no demand for V specific storage environment) Pharmacists may carry out more tests in: Permability Receptor-specificity, CYP450 inhibition/activation Genotoxicity
Page 7
Animal testing
i) Animal models Why do we need to use animal models in pre-clinical drug development? Many human diseases involve interactions between multiple organs & tissues These interactions cannot be fully understood through sole use of cell & molecular biological assays Animal models allow researchers to view the physiological impact of a drug - not just its cellular/biochemical Animal screening = expensive Occurs after extensive in-vitro studies Main aim of animal testing = Evaluation therapeutic index Ideal animal model: Produces valid results Displays selectivity Predictable (Oncology & CNS diseases are most unpredictable in animal models - researchers prefer use of iPs (induced pluripotent stem cells) derived from patients with onco/CNS genetic disease) Reproducible results
ii) Pharmacokinetics Rat, dog, pig or primate models Establishing ADME characteristics (See Pharmacokinetics lectures :) Bioavailabilty Tissue distribution Active metabolite formation Elimination test compound Tests typically last less than 48hrs Also used to establish appropriate administration methods (oral, bolus, intraperitoneal)
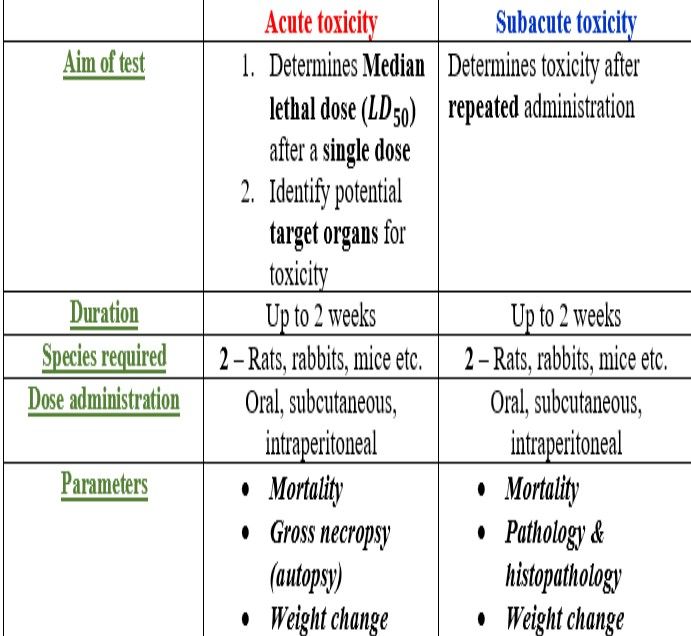
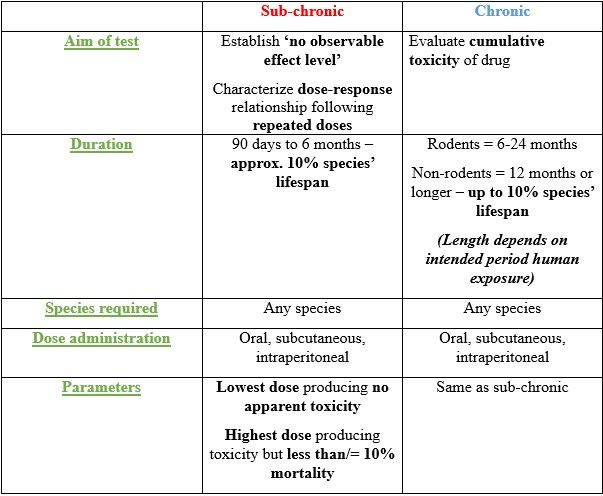
iii) Toxicity Acute vs subacute toxicity Chronic vs subchronic toxicity Reproductive toxicity
{kind=link}
{kind=link}
Reproductive toxicity Determine potential adverse effects of drugs on: Gametogenesis Foetal organogenesis Parturition Lactation Neonatal survival Vitality of newborn Carried out in rodents & rabbits Divided into 3 segments: Segment I (pre-conception): Treatment during gametogenesis Females = 60 days Males = 15 days Segment II (pre-implantation): Treatment during gestation Rodents = day 6-15 Rabbits = day 6-18 Segment III (perinatal to postnatal): Treatment through at least 15 days of gestation Plus 21 days lactation
Want to create your own Notes for free with GoConqr? Learn more.