38372995
Description
Quiz by Uchechukwu Nwanja, updated more than 1 year ago
|
|
Created by Uchechukwu Nwanja
over 1 year ago
|
|
Question 1
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
43 y.o. lady is complaining of joint pain.
Rheumatoid arthritis was diagnosed few years ago. She is taking Diclophenac, sometimes - Prednisolone. Obj.: Tender wrists, metacarpophalangeal, Proximal interphalangeal, Metatarsophalangeal joints.
X-ray of hands was performed.
What pathological changes are visible on X-ray, and for which stage of RA are they typical?
{kind=link}
Answer
-
Epiphyseal cysts, local subchondral osteoporosis; initial stage of rheumatoid arthritis
-
Bone erosions in metacarpophalangeal and proximal interphalangeal joints; evident RA (third stage)
-
Epiphyseal erosions in phalanx and palmar bones, narrowing of wrist's joint spaces; RA third stage (evident disease)
-
Cysts of phalanx, wrists ankylosis; advanced RA (fourth stage).
-
Epiphyseal cysts of finger bones, narrowing of metacarpophalangeal joints, osteoporosis, single erosions; RA third stage (evident disease)
Question 2
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
25 y.o. female is sick with rheumatoid arthritis, disease was diagnosed several years ago. Patient is taking Diclophenac and methotrexate. She is doing not bad, and is able to do all her usual works at home and in her office. Joint pain is mild, not everyday, morning stiffness lasts only a few minutes.
Obj.: slightly swollen wrists and II-III metacarophalangeal joints, not tender on palpation. Lab. tests- WBC normal. CRP 5 mg/l. Rheumatoid factor' 164 U/ml. X-ray: narrowed joint spaces, small marginal erosions of mentioned joints.
Which diagnosis is describing situation in the most correct way?
Answer
-
Arthritis rheumatoides, cursus rapide progrediens, act.II°, seropositiva. IF IIº.
-
Arthritis rheumatoides, cursus lentus, act.II°, seropositiva. IF II°.
-
Arthritis rheumatoides, cursus lentus, seropositiva, act.Iº, stadium II. IF II°
-
Arthritis rheumatoides, cursus lentus, seropositiva, act.1º, stadium II. IF 1º.
-
Arthritis rheumatoides, cursus lentus, act.II°, stadium II. IF Iº.
Question 3
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
45 y.o. female admitted due to the joint pain.
Rheumatoid arthritis was diagnosed 3 years ago. Patient is taking Diclophenac, but it does not helps, pain is not decreasing, joints are swollen.
Lung tuberculosis was diagnosed for this patient 3 months ago, she was treated with anti-tuberculous antibiotics. This treatment was effective- patient has no fewer, no cough, on lung X-ray - no signs of lung infiltration.
Lab.tests - slight anemia, ESR 40 mm/H., rheumatoid factor 240 U/ml. Hands X-ray: erosions of MCP joints, ankylosis or wrists.
Which treatment is the best option for the quick reduction of disease activity in this case?
Answer
-
Azahyoprin
-
Hydroxichloroquine
-
Methylprednisolone
-
Methotrexate
-
Sulphasalazin
Question 4
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
45 y.o. female has rheumatoid arthritis.
She is taking methotrexate, and Diclofenac. Two months ago dose of the methotrexate was increased up to 20 mg per week. After this, patient is feeling worse, especially last week: bad appetite, weakness, next day after the injection of methotrexate - nausea and abdominal pain.
Obj.: joint are tender on palpation and movements, but not swollen. Palpation of abdomen - tenderness, liver not increased.
Which tests are the most suitable the evaluation of reasons of worsening in this case?
Answer
-
Whole blood count, CRP, RF, anti-CCP.
-
Whole blood count, liver enzymes
-
Whole blood count, abdominal ultrasound
-
Whole blood count, urinalysis
-
Liver enzymes, test for occult gastrointestinal bleeding
Question 5
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
45 y.o. female admitted due to the joint pain.
Rheumatoid arthritis was diagnosed 3 years ago. Patient is taking Diclophenac, but it does not helps, pain is not decreasing, joints are swollen.
Lung tuberculosis was diagnosed for this patient 3 months ago, she was treated with anti-tuberculous antibiotics. This treatment was effective- patient has no fewer, no cough, on lung X-ray - no signs of lung infiltration. Lab.tests - slight anemia, ESR 40 mm/H., rheumatoid factor 240 U/ml. Hands X-ray:
erosions of MCP joints, ankylosis or wrists.
Which treatment is the most suitable in this case for the control of disease progression?
Answer
-
Azathyoprin
-
Hydroxichloroquine
-
Methylprednizolone
-
Methotrexate
-
Sulphasalazine
Question 6
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
45 y.o. female with rheumatoid arthritis, which was diagnosed 10 years ago. Patient is taking Diclophenac, occasionally - Prednisolone. Treatment does not help much, joint pain does not decrease, joint deformations progresses little bit. Patient is working as office administrator, and is complaining that it's hard to work with computer, to tape, to do her favorite leisure activity - knitting. Obj.: arthritis of the wrists and II-V metacarpophalangeal and proximal interphalangeal joints of both hands, metatarsophalangeal joint of both feet, all of these joints are swollen, painful. Slight knee deformation, typical for the osteoarthritis.
The patient should be sent for disability assessment.
Which test would be most useful to find out the degree of arthritis activity?
Answer
-
Echoscopy of hand joints
-
Knee X-ray
-
X-ray of hands and feet
-
RF, anti-CCP
-
ESR or CRP
Question 7
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
A 25-year old man had an appointment with the family doctor due to eight months ongoing back, sacral pain. Pain mainly increases in the morning, diminishes after exercising. 2 months ago he had left eye uveitis, and he was treated in hospital. He hasn't suffered from any other diseases. He doesn't take any medication. During the physical examination limited, painful movement of the lumbar spine (lateral, anterior flexion) was noticed. There were no other abnormalities in the in the other organ systems.
What medication would you prescribe today?
Answer
-
Diclofenac intramuscular injection
-
Diclofenac tablets
-
Paracetamol
-
Prednisolone
-
Tolperisone
Question 8
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
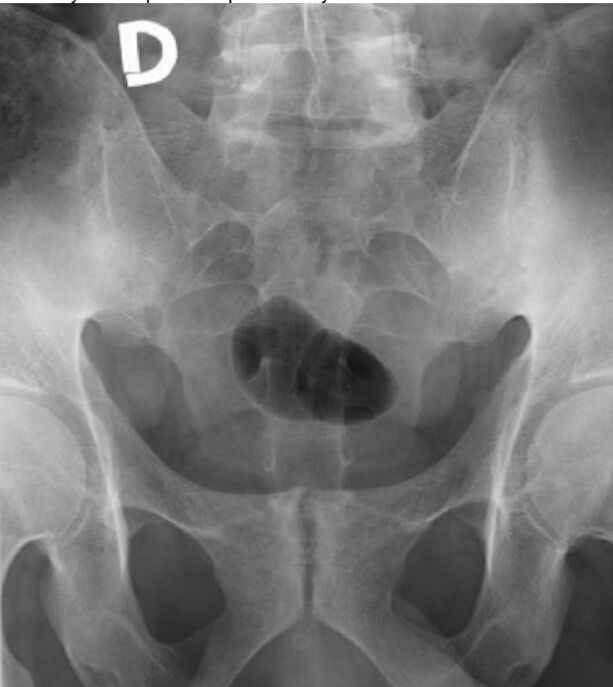
A 27-year-old man visited a family doctor. He has been suffering from back, hip, sacrum, thoracic pain for several years. In the past, he felt pain inconstantly. Osteochondrosis was diagnosed, he was assigned to exercise, occasionally he took NSAIDs. In recent years, the pain has been intensified, and it mainly increases in the morning, diminishes after exercising and taking Diclofenac. Two months ago, he had left foot Achillitis. There is no history of other diseases. During the physical examination, limited, painful movements of the lumbar spine (lateral flexion, forward flexion) were determined. The general physical examination was unremarkable.
The family doctor performs pelvic X-ray:
Describe the changes in the X-ray:
{kind=link}
Answer
-
Grade 3 sacroiliitis bilaterally
-
Grade 3 bilateral coxarthrosis
-
X-ray without of pathological changes
-
Ankylosis of sacroiliac joints
-
Grade 2 sacroiliitis bilaterally
Question 9
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
A 27-year-old man was referred to a rheumatologist. He has been suffering from back, hip, sacrum, thoracic pain for several years. In the past, he felt pain inconstantly. Osteochondrosis was diagnosed, he was assigned to exercise, occasionally he took NSAIDs. In recent years, the pain has been intensified, and it mainly increases in the morning, diminishes after exercising and taking Diclofenac. Two months ago, he had left eye uveitis, and he was treated in hospital. There is no history of other diseases. During the physical examination, limited, painful movements of the lumbar spine (lateral flexion, forward flexion) were determined. There are no swollen joints, "old" sacroiliitis is observed in the pelvic radiograph. Ankylosing spondylitis was diagnosed.
What are the most appropriate blood tests to determine the inflammatory activity?
Answer
-
Complete blood count, HLAB27
-
CRP and ESR
-
ESR
-
HLAB27
-
RF and complete blood count
Question 10
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
A 21-year-old student was referred to a rheumatologist. He has been suffering from lumbar, sacral pain for six months. He thought it hurts because of a long sitting at a computer. Recently, the pain is severe; it awakens him in the morning, he feels morning stiffness and limps. Two months ago, he had a left eye uveitis and was treated in a hospital. He hasn't suffered from any other diseases. He doesn't take any medication. During the examination, limited, painful movements of the lumbar spine (flexion to the side, forward) were determined. The movements of the hip joints are free. There were no other abnormalities in the in the other organ systems. The patient's cousin suffers from Crohn's disease. CRP 36 mg/l. Rheumatologist performed pelvic X-ray:
Please comment on the X-ray. What will you do?
{kind=link}
Answer
-
There is bilateral hip osteoarthritis, no further studies are required, I will give ibuprofen.
-
X-ray without pathological changes, MRI of sacroiliac joints should be performed to clarify the diagnosis, I will give Prednisolone.
-
X-ray without pathological changes, MRI of sacroiliac joints should be performed to clarify the diagnosis, I will give Diclofenac.
-
There is bilateral sacroiliitis on X-ray, no further studies are required, I will give Diclofenac.
-
X-ray without pathological changes, CT of sacroiliac joints should be performed to clarify the diagnosis, I will give Prednisolone.
Question 11
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
A 43-year-old woman was referred to rheumatologist due to worsening condition, treatment. A 15-years ago she was diagnosed with ankylosing spondylitis (she suffered from inflammatory back pain, there was bilateral sacroiliitis on X-ray). She was treated with NSAIDS, physiotherapy and the condition was stable. For about four months her condition has worsened - both knees, ankles, II-IV MTF joints of right foot became swollen. She has tried three different NSAIDs in maximal dosages, but the condition hasn't improved yet. The physical examination: signs of arthritis in both knees, ankles, II- IV MTF. Laboratory tests: CRB: 65 mg/l, CBC, ALT, AST, creatinine within normal ranges.
Which medication would be most appropriate in this case?
Answer
-
Methotrexate and sulfasalazine
-
Prednisolone tablets and intraarticular injections
-
Sulfasalazine and low dose of prednisolone (tablets)
-
Tiramcinolone injections in both knees
-
TNF blockers and Triamcinolone injections into the ankle joints
Question 12
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
A 24-year-old man arrived due to swollen both knees and right ankle joints. Two days ago, he got fever up to 38.0 °C; later his knees and right ankle became painful and swollen. He denies trauma. Previously he was healthy, had only cold and a week ago there was an episode of painful urination, but then he did not make an appointment. Patients uncle suffers from skin psoriasis
During the physical examination, both knee and right ankle joints are very painful, slightly red. Temperature 37.4 °C. A total blood count: leucocytes 12x109/I, neutrophils 78%, Hb 140 g/l, red blood cells 5.1x1012/I, CRP 80 mg/l. An arthrocentesis of the right knee joint was done, 60 ml of yellowish turbid fluid were obtained. Joint fluid tests: leukocytes 46000x106/1, neutrophils 66%; The microscopic examination didn't show any crystals or bacteria
Which diagnosis is most likely in this case?
Answer
-
Gout
-
Psoriatic arthritis
-
Reactive arthritis
-
Rheumatoid arthritis
-
Septic arthritis
Question 13
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
Seven weeks ago a 38-year-old man was diagnosed with reactive arthritis (both knees and right elbow were swollen, arthritis developed after diarrhea, and campylobacteriosis was diagnosed). He was treated with NSAIDs, injections of triamcinolone into both knee joints and methylprednisolone up to 30 mg per day was prescribed. Arthritis of both knees and right elbow is still present. Blood tests: CRP 55 mg/l, HLAB27 detected.
What could be considered as the best treatment for this patient?
Answer
-
Azathioprine
-
Doxycycline
-
Methotrexate
-
Sulfasalazine
-
TNF α blocker
Question 14
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
24 year old male patient suffers from II and IV toes of left foot, right knee and left ankle swelling, bilateral heel and foot pain, pain and stiffness of low back and cervical spine. On examination psoriasis of interphalangeal region was found of both feet, dactylitis of left feet, arthritis of right knee and left ankle. The patient uncle and great-grandmother had psoriasis. Laboratory tests revealed: Hb 142 g/l, ESR 52 mm/h, serum uric acid 524 mmol/l, RF negative, HLAB 27 positive.
On X-ray new bone proliferation of distal interphalangeal joints of feet, erosions of metatarsophalangeal joints, calcaneus and cervical spine enthesitis and left side sacroiliitis was found.
What symptoms and signs are needed to establish diagnosis of psoriatic arthritis according to CASPAR classification criteria?
Answer
-
Uncle of the patient had psoriasis, the patient has negative RF, dactylitis and new bone proliferation in distal interphalangeal joints on X-ray of feet.
-
The patient has psoriasis, negative RF, left side sacroiliitis and cervical spine and calcaneus enthesitis on X-ray.
-
The patient has psoriasis, positive HLAB27, left side sacroiliitis and cervical spine and calcaneus enthesitis on X-ray.
-
Uncle of the patient had psoriasis, the patient has right knee and left ankle arthritis, negative RF, ESR 52 mm/h and left side sacroiliitis and cervical spine and calcaneus enthesitis on X-ray
-
Great grandmother of the patient had psoriasis, the patient has elevated serum uric acid and left side sacroilitis and erosions of metatarsophalangeal joints on X-ray
Question 15
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
24 year old male patient suffers from stiffness and pain of cervical spine and low back, pain of right heel and both foot, pain and swelling of left wrist, right knee, left
metacarpophalangeal and distal interphalangeal joints of right hand and left II toe. The patient has psoriasis since childhood, his sister and great-grandmother suffers from
this disease as well.
On examination arthritis of left wrist, right knee, left metacarpophalangeal joints and distal interphalangeal joints of right hand was found, painful metatarsophalangeal joints on both sides and left II toe dactylitis was observed.
Laboratory tests showed: HLAB27 positive, RF negative. On X-ray: left side sacroiliitis, erosions of metatarsophalangeal joints, enthesitis of right calcaneus was found.
Which set of symptoms and signs are specific only for psoriatic arthritis and cannot be found in rheumatoid arthritis?
Answer
-
Great-grandmother of the patient had psoriasis, the patient has arthritis of right knee and arthritis metacarpophalangeal joints of left hand, HLAB27 positive.
-
Great-grandmother of the patient had psoriasis, the patient suffers from stiffness and pain of cervical spine, HLAB27 positive, RF negative.
-
The patient suffers from psoriasis, he has arthritis of left wrist, RF negative, on X- ray: erosions of metatarsophalangeal joints were observed.
-
The patient suffers from psoriasis, he has RF negative, on X-ray: erosions of metatarsophalangeal joints were observed.
-
A sister of the patient has psoriasis, the patient has left foot dactylitis and arthritis of distal interphalangeal joints of right hand, on X-ray: left side sacroiliitis and enthesitis of right calcaneus was observed.
Question 16
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
24 year old male patient suffers from stiffness and pain of cervical spine and low back,
pain of right heel, swelling of left II and IV toe. Duration of symptoms more than 5 years. The patient has psoriasis since childhood, his sister and great-grandmother suffers from this disease as well. On examination dactylitis of left II and IV toe and extremely restricted motion of neck and low back was observed.
On laboratory tests: CRP 105 mg/l, ESR 56 mm/h.
On X-ray: sacroiliitis on left side and enthesitis of cervical and lumbar spine as well as right calcaneus was revealed. The patient is on diclophenac 150mg/d and Methotrexate 20 mg/w for the last 1,5 years.
What treatment would be the best option for this patient?
Answer
-
Methotrexate 25 mg/w
-
Prednisolon 15 mg/d
-
Prednisolon 15 mg/d, Methotrexate 25 mg/w
-
Prednisolon 15 mg/d, Methotrexate 25 mg/w, TNFα inhibitors
-
TNFα inhibitors
Question 17
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
24 year old male patient suffers from stiffness and pain of cervical spine and low back and pain of right heel. Duration of symptoms is more than 5 years. The patient has psoriasis since childhood, his sister and great-grandmother suffers from this disease as well.
On examination extremely restricted motion of neck and low back was observed. On X-ray sacroiliitis on left side and enthesitis of cervical spine as well as right calcaneus was revealed.
What tests have to be performed in order to establish activity of the disease for this patient?
Answer
-
BASDAI, DAS 28, ESR, CRP, HLAB 27
-
BASDAI, ESR, CRP
-
DAS 28, ESR, CRP, HLAB 27
-
DAS 28, Hb, platelets, ESR
-
Ultrasound examination, Hb, platelets, ESR, CRP, HLAB 27
Question 18
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
64 years old woman suffers from pain and stiffness of neck and low back, pain of both knees, metatarsophalangeal joints and right heel. Duration of symptoms more than 5 years.
The patient has nail psoriasis since childhood.
On examination extremely restricted motion of cervical and lumbar spine was found and enlargement of distal interphalangeal joints of hands and feet was observed. Laboratory tests showed positive HLAB 27, ESR 30 mm/h.
On X-ray: sacroiliitis of left side, joint space narrowing and osteophytes of knees, osteolysis of metatarsophalangeal joints and right calcaleal spur was revealed.
What set of signs are specific only for psoriatic arthritis and not found in osteoarthritis?
Answer
-
Psoriasis, enlargement of distal interphalangeal joints, ESR 30 mm/h, calcaneal spur
-
Sacroiliitis of left side, osteolysis of metatarsophalangeal joints
-
Psoriasis, cervical spine, lumbar spine and sacral pain and stiffness, positive HLA B27
-
Psoriasis, enlargement of distal interphalangeal joints, positive HLA B27
-
Psoriasis, positive HLA B27, joint space narrowing and osteophytes of knees
Question 19
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
60-Year-Old man is complaining with a soft palpable mass on the left elbow area which periodically gets painful, red and swollen, also with sudden attacks of pain and swelling in the left metatarsophalangeal or right knee joint area. Pain and swelling disappear after Diclofenac few days' course. Symptoms last for 5-6 years. Patient is obese, has diabetes (type II) and hypertension.
What is the most probable joint disease in this case?
Answer
-
Osteoarthritis and elbow bursitis
-
Rheumatoid arthritis
-
Acute gout
-
Intermittent gout
-
Reactive arthritis
Question 20
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
48-Year-Old man with gout diagnosis, not taking any medication, comes due to the first metatarsophalangeal (MTP) joint arthritis. Objectively: I MTP joint is deformed, swollen, red and painful. Laboratory tests: CRP 24 mg/l, Erit. 5x1012 g/l, Hb140 mg/l, Leu. 10,9x 10° g/l, Plt. 400 x 10 g/l; serum uric acid 400 μmol/l, creatinine 80 μmol/l.
What treatment is the most suitable in this case now?
Answer
-
Diclofenac 50 mg 3 times per/day per os
-
Allopurinol 300 mg daily per os
-
Allopurinol 100 mg daily per os
-
Methylprednisolon 500 mg intravenously
-
Sol. Penicillin 2 mln. IU 4 times per/day intravenously
Question 21
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
48-Year-old man, ill with gout, under the Allopurinol treatment (100 mg/per day)
comes to rheumatologist. Objectively: I MTP joint is deformed, swollen, red and painful. Feet area examination revealed two subcutaneous nodules. Lab. test results: CRP 24 mg/l; general blood test: Erit. 5x10¹2 g/l, Hb 140 mg/l, Leu.
10,9x 10 g/l, PLT 400 x 10 g/l. Serum uric acid 460 μmol/l.
What treatment would be the most reasonable in this case?
Answer
-
Continue with the same Allopurinol dose, with addition of Diclofenac 50mg TID till disappearance of arthritis symptoms
-
Allopurinol 300 mg daily
-
Temporary stop Allopurinol treatment and give Diclofenac 50mg TID till disappearance of arthritis symptoms.
-
Continue with the same Allopurinol dose, with addition of Diclofenac 50mg TID till disappearance of arthritis symptoms and increase Allopurinol dose up to 300 mg per day afterwards.
-
Treatment with Allopurinol should be switched to the treatment with Colchicine
Question 22
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
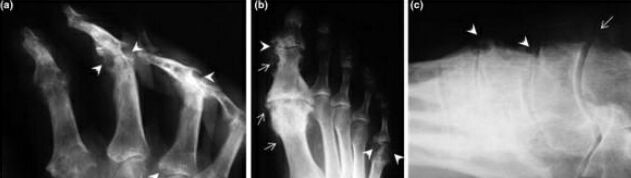
A man, suffering with periodical arthritis symptoms for many years, comes to rheumatologist. The exact diagnosis of his symptoms was never made. Patient was taking Diclofenac or Ibuprofen pills to treat the pain and joint swelling. He also brought his recent hand and foot x-rays.
What changes can be seen on x-rays and what is the most probable diagnosis?
{kind=link}
Answer
-
Periarticular osteosclerosis, narrowing of joint space, cystic bone changes due to rheumatoid arthritis
-
Periarticular osteoporosis, multiple cystic bone changes due to osteoarthritis
-
Periarticular osteosclerosis, narrowing of joint space in the first metatarsophalangeal joint, proximal interphalangeal joints; multiple punched-out or "mouse bitten" appearance bone erosions in hand, foot and tarsal bone area, due to chronic tophaceous gout.
-
Periarticular osteosclerosis, narrowing of joint space in the first metatarsophalangeal joint, proximal interphalangeal joints; multiple punched-out or "mouse bitten" appearance bone erosions in hand, foot and tarsal bone area, due to rheumatoid arthritis.
-
Periarticular osteosclerosis, narrowing of joint space in the first metatarsophalangeal joint, proximal interphalangeal joints; multiple punched-out or "mouse bitten" appearance bone erosions in hand, foot and tarsal bone area, due to acute gout.
Question 23
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
45 y.o. female arrived to her family doctor because of general weakness.
She is working as seller in supermarket, and feels very tired, temperature raises every evening up to 37.2-37.3° C. She lost 3 kg of weight per month. Obj. hard to get form the chair, to raise hands, atrophy of the thigs muscles. Swelling and erythemic rash around the eyes. Dermatomyositis was suspected.
The most appropriate tests to evaluate tissue damage in this case are:
Answer
-
Skin biopsy, WBC, ESR, capillaroscopy.
-
Serum creatinphosphokinase, transaminases, muscle biopsy
-
Serum transaminases, antinuclear antibodies, muscle biopsy
-
WBC, CRP, electroneuromyography, capillaroscopy
-
Antinuclear antibodies, rheumatoid factor, serum creatinphosphokinase
Question 24
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
30 y.o. woman arrived because of general weakness, headaches, fevers up to 37.6°C,
facial rashes, wrist and ankle arthritis. Worsening started approximately 1 month ago. Several years ago, systemic lupus erythematosus was diagnosed, and patient is on plaquenil and low doses of prednisolone. Lab.tests: 100 g/l, leukocytes 3.8 x10 1, PLT 105 x10, Urinanalysis - normal, anti-
DNA 284 U/I (normal < 32 U/I). Ophthalmologists consultation - vasculitis of retinal vessels.
Brain MRI-vasculitis of small blood vessels.
Which treatment would be most appropriate in this case:
Answer
-
Prednisolone per os and azathyoprine
-
Azathyoprine and plaquenil
-
Prednisolone pulstherapy and ibuprophen
-
Prednisolone per os and methotrexate
-
Prednisolone puls therapy and cyclophosphamide
Question 25
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
55 y.o. woman was diagnosed with dermatomyositis 3 months ago. The diagnosis was confirmed by the muscle biopsy, and elevated creatinphosphokinase (2500 U/I, normal < 171 U/l). She was treated with prednisolone 30 mg per day, after 4 weeks dose was increased up to 60 mg per day. But patient feeling bad, very weak, difficult to move. She has no appetite, often spins when eating. She lost 5 kg of body weight.
Obj.: The weakness of proximal muscles of hands and legs, muscles looks atrophied. The voice is tight. Weight - 65 kg.
Lab.tests: WBT is normal, ESR-80 mm/H, serum creatinphosphokinase 4300 U/I.
Which treatment is most useful in this case:
Answer
-
Methylprednisolone and cyclophosphamide puls therapy
-
Prednisolone 1 mg/kg, until CPC normalisation
-
Prednisolone 1,5 mg/kg and methotrexate
-
Mehylprednisolone and azathyoprine
-
Prednisolone and anabolic hormones
Question 26
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
35 y.o. woman is complaining about facial rashes, general weakness, polyarthralgia. Bad feeling - approximately half of year, subfebrille fever.
Obj. facial erythemic rashes, Raynaud syndrome in her hand fingers, paiful metacarpophalangeal joints and wrists, diffuse alopecia. T-37.3°C. Edema of distal parts of legs.
Lab.tests: Hb 100 g/l, leukocytes 2.8x109/I, PLT 105 x10 /, Urinanalysis - normal, anti-DNA 284 U/I (normal < 32 U/I).
Which tests are most appropriate for the evaluation of SLE activity:
Answer
-
Antinuclear antibodies
-
Proteinuria/24 hours, and urine culture
-
CRP, and proteinuria/24 hours
-
Anti-DNA, complement components
-
Complement components and ANA
Question 27
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
35 y.o. woman admitted due to rashes on the face and palms, fatigue, joint pain. Worsening - about 6 months, fevers up to 37.3.
Several years ago she had severe sunlight dermatitis. Obj. facial erythemic rashes, vasculitic rashes on the skin of palms, Raynaud
syndrome, painful metacarpophalangeal joints and wrists, diffuse alopecia. T-37.3°C. Edema of the distal parts of legs. ABP 146/82 mm Hg. Pulse 90 /min.
Systemic lupus erythematosus was suspected.
Which tests are most appropriate for evaluating of organ damage:
Answer
-
Whole blood count, anti-DNA, complement
-
Whole blood count, urinanalysis, CRP
-
Whole blood count, abdominal echoscopy
-
Whole blood count, urinanalysis, creatinine, glomerular filtration rate
-
Whole blood count, urine analysis, proteinuria/24 hours, creatinin, serum albumin
Question 28
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
35 y.o. woman admitted due to rashes on the face and palms, fatigue, joint pain. Worsening - about 6 months, fevers up to 37.3.
Several years ago she had severe sunlight dermatitis.
Obj. facial erythemic rashes, vasculitic rashes on the skin of palms, Raynaud syndrome, painful metacarpophalangeal joints and wrists, diffuse alopecia. T-37.3°C. Edema of the distal parts of legs.
Which diagnosis is most probable:
Answer
-
Systemic lupus erythematosus
-
Systemic scleroderma
-
Skin lupus erythematosus
-
Reactive arthritis
-
Leukocytoclastic vasculitis
Question 29
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
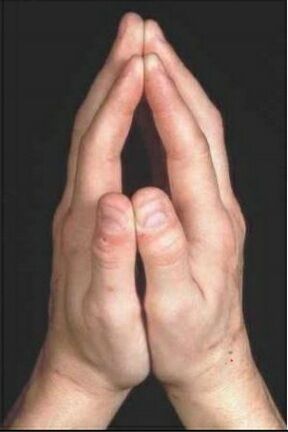
46 year old lady complains about inability to work, she feels very sick. She should work outside the building. The main complain - painful whitening of fingers, especially at work, even very warm gloves does not help. Fingers of arms painful, hard to flex.
Examination findings:
Painful MCP joints, telangiectasia on the face. Patient was asked to put both arms
together, see picture.
Which symptom is presented on picture?
{kind=link}
Answer
-
Arthritis
-
Sclerodactily
-
Raynaud syndrome
-
Tendonitis
-
Acrocianosis
Question 30
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
46 year old lady complains about inability to work, she feels very sick. She should work outside the building. The main complain - painful whitening of fingers, especially at work, even very warm gloves does not help. Fingers of arms painful, hard to flex.
Examination findings:
Painful MCP joints, telangiectasia on the face. Patient was asked to put both arms
together, see picture.
Which medicine and other treatment would be the best?
Answer
-
Skin care oils, keep arms elevated, wear think and natural wool gloves in winter time
-
Pentoxyphyline or nifedipine maximum dosage, NSAIDS
-
Change work conditions, nifedipine maximum dosage
-
Change work conditions, NSAIDS, rehabilitation procedures
-
Change work conditions, glucorticoids injections to the painful joints
Question 31
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
68 year old man visited family doctor complaining of painful joints, swelling of hand fingers, weight loss, and shortness of breath, night cough, food swelling problems and painful fingers ulcers. Spontaneous collection of white, chalk like masses in fingers, these erupts later on.
Clinical findings: thick skin on fingers and forearms, no signs of arthritis, hand to flex fingers, distal part of fingers with ulcers and subcutaneous white masses collections. Bilateral crackles in the lungs, hard leg oedema.
Tests results: ESR - 55 mm/h., peripheral blood test - normal. Uric acid in the blood- 600 micromole/l (normal value less than 450 micromol/l).Chest X-ray - bilateral lung tissue fibrosis.
What laboratory test should be done to prove that it is autoimmune disease?
A.
B.
C.
D.
E.
Answer
-
Antinuclear antibodies (ANA) and extracted antinuclear antibodies (ENA)
-
Antinuclear antibodies (ANA) and extracted antinuclear antibodies (ENA), immunoglobulins (Ig A, G, M)
-
Antinuclear antibodies (ANA) and extracted antinuclear antibodies (ENA), rheumatoid factor (RF)
-
Rheumatoid factor (RF), immunoglobulins (Ig A, G, M), HLA-B27
-
Antinuclear antibodies (ANA), CRP, rheumatoid factor (RF), subcutaneous masses microscopy after aspiration for urate crystals deposition
Question 32
Question
Scenario: (If a clinical vignette, then keep scenarios realistic and language naturalistic rather than technical)
68 year old man visited family doctor complaining of painful joints, swelling of hand fingers, weight loss, and shortness of breath, night cough, food swelling problems and painful fingers ulcers. Patient was sick around a year, not visited doctor before. Clinical findings: thick skin on fingers and forearms, no signs of arthritis, hand fingers contractures, distal part of fingers with ulcers and subcutaneous small calcifications. Bilateral crackles in the lungs, hard leg oedema.
Tests results: ESR - 55 mm/h. peripheral blood test - normal. Chest X-ray - bilateral lung tissue fibrosis, marked dilatation of right atrium.
Right heart catheterisation was done - high pressure was found in right heart.
What is most appropriate treatment for this patient shortness of breath?
Answer
-
Reduce physical activity, breathing exercises, inhalator bronchodilator's
-
Vasodilatation medicine - nifedipine and etc.
-
Diuretics and glucocorticoids
-
Oxygen therapy, prednisolone,
-
Transplantation of lungs and heart
Want to create your own Quizzes for free with GoConqr? Learn more.