4990755
Diabetes
Resource summary
Slide 1
Diabetes (T2D)
100 amputations a week on patients with diabetes
3.8m Britons have diabetes
600,000 of people don't know they have the disease
24,000 diabetic die early each year
Chronic metabolic disease caused by insulin deficiency - the pancreas does not produce enough insulin to maintain a normal blood glucose level ORReduced effectiveness- insulin that is produced does not work correctly suggesting a defect of insulin action at the receptor, this is known as insulin resistance. OR BOTH
Slide 2
{kind=link}
Why we love Insulin
Slide 3
Clinical Features & Screening
CLINICAL FEATURES
Characterised by a raised blood glucose concentration
Presents with acute symptoms and severe multisystem chronic complications
Age of diagnosis >40 and onset is low
Increased weight
The endogenous insulin is present but insuffienct/ inefficient
SCREENING IN THE COMMUNITY
NHS health check - aged 40 - 7
If exhibit symptoms of diabetes
If have multiple risk factors - overweight, family history, ethnicity
Slide 4
Aetiolgy (Cause)
RISK FACTORS
Age - being over 40 (over 25 for south Asian). This may be because people tend to gain weight and exercise less as they get older.
Genetics- first degree relative with the T2D. Parent with T2D increases risk to 1 in 3.
Weight- overweight/obese. Abdomen fat increases risk because chemicals are released with can disrupt the body's cardiovascular and metabolic systems. This increases the risk of CVD and stroke.
Ethnicity - South Asian (x6 more common), Chinese, African-Caribbean and Black African (x3 more common).
CAUSE
Impaired insulin secretion from pancreas and insulin resistance.
There is a strong genetic component involved more than Type I, so there is a probability of inheriting Type II. A missense mutation is the glucagon gene has been shown to be associated with the development of type II.
Environmental - lifestyle; excessive calorie intake and inadequate calorie expenditure, high sugar diet.
Slide 5
{kind=link}
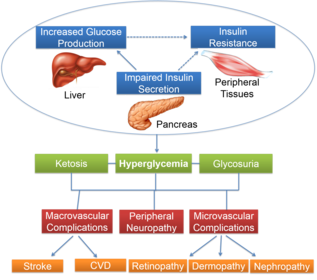
Pathophysiology Overview
As tissues are not taking up the insulin, the liver continues to produce and secrete glucose → hyperglycemia and glycosuria. Glycosuria occurs because the filtered glucose exceeds the renal threshold → glucose appears in the urine and acts as an osmotic diuretic → frequent urinations and excessive thirst which are the most common symptoms → over time the hyperglycemia damages the blood vessels → macro/microvascualr complications. The main cause of morbidity and mortality in diabetes in the poorly controlled hyperglycemia over a period of years. The damage is irreversible.
Slide 6
Pathophysiology
Macrovascular Complications
Macroangiopathy - large vessel disease which leads to accelerated atherosclerosis. Increases the risk of:
IHD ( Angina/MI)
Stroke
CVD - 8/10 people with T2D die from CV events.
Hypertension
Peripheral vascular disease (PVD) - pain in legs and arms due to poor perfusion, skin ulcers and amputations
Atherosclerosis also increases susceptibility to infection
Microvascular ComplicationsMicroangiopthay - disease of fine capillary damage. This occurs due to protein glycation and small osmotic damage in small blood vessels.
Retinopathy - can cause blindness, cataracts, glaucoma.
Nephropathy - result in renal failure
Neuropathy - damage to nerves
Sensory: numbness, tingling and neuropathic pain. Autonomic: impotence, GI disturbance, postural hypotension. Damage to sympathetic/parasympathetic nerves may result in loss of normal cardiovascular reflexes.
Slide 7
Complications
CHRONIC'Diabetic Foot' - caused by PVD, neuropathy, increased susceptibility to infection. The peripheral nervous tissue becomes progressively damaged, → pain → eventual numbness in the feet →Can result in amputation.
ACUTE
Hyperosmolar Hyperglycemic State (HHS) - due to high glucose → dehydration and high osmolarity. Treated with sliding scale insulin and IV saline.
Diabetic ketoacidosis - state of uncontrolled catabolism associated with insulin deficiency(usually Type 1). Breakdown of fatty acids → which ↑ ketone bodies → ↓ plasma pH. Treated with sliding scale insulin, IV saline and potassium. (as there will be electrolyte imbalances.
Hypoglycaemia - symptomatic if glucose <202mmol/L. Treat onsite with 2 teaspoons of sugar/equivalent and hospital IM Glucagon (will ↑ conc. of glucose)
Slide 8
Signs and symptoms
SYMPTOMS
Fatigue
Polydipsia
Frequent urination - especially at night
Genital itching or thrush
Always hungry
Blurred vision
Sudden weight loss
Wounds taking longer to heal
Slide 9
Diagnosis
Symptoms
Urine sample - detection of glucose
HbA1c - gives the average blood glucose levels over the previous 2-3months.
Glucose Tolerance Test (GTT) - 75g glucose in water. Blood glucose before and 2 hours after the glucose has been given. Fasting plasma glucose ≥7.0mmol/L
Random plasma glucose ≥ 11.1mmol/L
Blood pressure
Blood lipids
Family history
Slide 10
National Service Framework (NSF)
The NSF for Diabetes sets quality standards for diabetes care. The standards aim to improve care for people with diabetes. There are 12 standards. Standard 4:
Improve blood glucose control - drug choice/monitoring
Control hypertension - reduce CVD/retinopathy/nephropathy
Reduce raised cholesterol levels - give statin + aspirin (secondary prevention)
Encourage smoking cessation - NRT
Slide 11
Treatment Options
Diet Alone
Diet + oral antidiabetic drugs
Diet + oral antidiabetic drugs + Insulin
AIMS
Avoid hypo and hyper
Maintain normal body weight
Reduce risk of CVD
Overall health through good nutrition
Slide 12
Diet
STRATEGIES
Refer to dietician
Aim for realist BMI
portion and proportion control
Eat smaller, more frequent meals
Vary content
Adjust for any unusual activity
DIET
Carbohydrate - 50-60% calories. Low glycaemic index foods such as fibre (slow absorption of sugar), complex carbohydrates (polysaccharides) - pasta, potatoes, rice. Small amount of sugar allowed.
Fat - low fat diet. <35% energy from fat. More polyunsaturated fats and low cholesterol.
5 Portions of fruit and veg
Reduce salt intake
Alcohol - ok in moderation. BUT blood glucose will ↑ and then ↓↓. Best with food and count the calories.
Slide 13
Insulin
Porcine, Bovine, Human sequence insulin, recombinant human insulin
Route - SC, IM, IV
T2D - when other methods have failed to achieve good control.
Temporarily in the presence of intercurrent illness or peri-operatively
Insulin Pump - The insulin is houses inside the pump in a cartridge called a reservoir. The insulin travels into your body through a flexible tube that ends with a cannula inserted just under the skin.
Dosage - tailor to the individual depending on motivation, comprehension, lifestyle and pattern of eating and activity.
Aim- to keep blood glucose 4-10mmol/L and HbA1c <7.5%
Patients can self-monitor and fine tune dose themselves.
AE's - weigh gain, hypo, resistance, allergy, lipoatrophy/lipohypertrophy at injection site - rotate injection site.
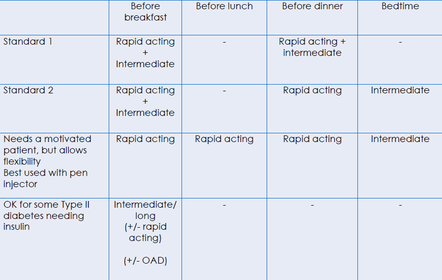
Rapid acting -Lispro (Humalog), Asparte (Novarapid) - works within in 15 mins. peaks 30-90misn and can last 4 hours.
Short- acting - regular insulin. works within 30 mins. peaks 2-4hours and last 4-8 hours
Intermediate -Isophane/NPH, Humulin I. usually taken with short acting. work within 1 hour, peak up to 7 hours, and lasts 18-24 hour.
Long acting- Ultralente, Glargine (Lantus), Determir (Levermir) . works within 6-14 hours, peaks at 10-16hrs and last 20-24hrs.
Slide 14
Insulin Counselling
Insulin absorption - to be aware of the factors influencing insulin absorption which can have an effect on blood glucose control
Injection site - to ensure that the appropriate sites are used for injecting insulin
Injection technique - to ensure that insulin is injected correctly
Injection site rotation - to prevent lipohypertrophy
Timing of injection - to optimize glycemic control
Self-injecting - support parents and young children using self-injecting insulin
Slide 15
{kind=link}
Insulin Regimen
Slide 16
Drug Treatment -
Initial drug treatment- Treatment with a single non‑insulin blood glucose lowering therapy (monotherapy)Metformin OR if contra - DPP-4 Inhibitor or Pioglitazone or SulfonylureaFirst intensification of drug treatment - Treatment with 2 non‑insulin blood glucose lowering therapies in combination (dual therapy)Metformin + DPP-Inhibitor/Pioglitazone/Sulfonylurea OR if contra - DPP-4 + Pioglitazone/Sulfonylurea or Pioglitazone + Sulfonylurea Second intensification of drug treatment - Treatment with either 3 non‑insulin blood glucose lowering therapies in combination (triple therapy) or any treatment combination containing insulinMetformin + DPP-4 Inhibitor + sulfonylurea or Metformin + Pioglitazone + Sulfonylurea + Insulin
Slide 17
Drug Treatment
{kind=link}
Caption: : Drug treatment if diabetes is not controlled by diet alone for 3 months
Insulin sensitizers - bigunaide, glitazonesInsulin secretogogues - sulphonylureas, meglitinides, DPP-4 inhibitors (gliptins)GI glucose absorption inhibitor - acarbose
Slide 18
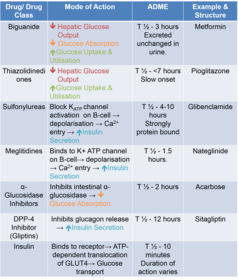
Pharmacology and Pharmacokinetics
BIGUANIDE (METFORMIN)
↓ gluconeogenesis
↑ peripheral utilisation of glucose
First line treatment in obese patients as it does not increase appetite
AE's- anorexia, N&V&D
SULPHONYLUREAS
↑ Insulin secretion
For patients who metformin is contra
Common AE- hype
long acting - glibenclamide - greater risk of hypo
short acting - gliclazide, tolbutamide
ALPHA- GLUCOSIDASE INHIBITORS (ACARBOSE)
Inhibits intestinal glucosidase, impairing carb digestion and glucose absorption
Small but significant effect in lowering blood glucose
AE- GI effects; flatulence, bloating and D.
THIAZOLIDINEDIONES (PIOGLITAZONE)
Enhance insulin receptor sensitivity → ↓ peripheral insulin resistance
Used alone or in combo
Small increase risk of bladder cancer
GLIPTINS (DPP-4 INHIBITORS)Inhibit DPP-4 → ↓ glucagon secretion and ↑ insulin secretionPOST-PRANDIAL REGULATORS
Stimulate insulin release
Rapid onset and short duration
Administered shortly before each meal
Repaglinide - mono or combo with metformin
Nateglinide - ONLY with metformin
↑ ketone bodies → ↓
Slide 19
Pharmaceutics
{kind=link}
Slide 20
Pharmacoeconomics
10% of the NHS budget is spent of the disease
£17b will be cost to NHS by 2025
Slide 21
Clinical Monitoring
{kind=link}
Slide 22
Control of Hypertension
Not all drugs are appropriate
B-Blockers should generally be avoided - mask some symptoms of hypo
Diuretics used with caution - Hypokalemia can impair insulin release and worsen glucose tolerance
ACEI- usually drug of choice. Especially in presence of proteinuria and in presence of HF.
Slide 23
NICE Guidelines (2009 & 2015)
RECOMMENDATIONS
Individualized care - tailored to the individual taking into account their personal preferences, comorbidities, risks from polypharmacy, and their ability to benefit from long‑term interventions because of reduced life expectancy.
Patient education - structured education programme meets all patient needs, eg. linguistics, culture
Dietary advice - Individualize, Integrate and emphasize
Blood pressure management - check annually, lifestyle advice. Repeat blood pressure measurements within:
1 month if blood pressure is higher than 150/90 mmHg
2 months if blood pressure is higher than 140/80 mmHg
2 months if blood pressure is higher than 130/80 mmHg and there is kidney, eye or cerebrovascular damage.
Antiplatelet therapy - Do not offer antiplatelet therapy (aspirin or clopidogrel) for adults with type 2 diabetes without cardiovascular disease
Blood glucose management - HbA1c measurements and targeting measure very 6 months if stable. Managed either by lifestyle and diet, or by lifestyle and diet combined with a single drug not associated with hypoglycaemia, support the person to aim for an HbA1c level of 48 mmol/mol (6.5%). For adults on a drug associated with hypoglycaemia, support the person to aim for an HbA1c level of 53 mmol/mol (7.0%).
Slide 24
7. Managing complications
Gastroparesis - antiemetic not helpful but maybe erythromycin and metocloprimaide alternated.
Neuropathy - treat neuropathic pain
Erectile dysfunction
Diabetic foot problems
Eye Disease: Retinopathy - regular eye tests. Can be managed with laser treatment. Need good glucose and BP control. Refer to optometrist or ophthalmic optician. Free eye tests for diabetics.
Kidney Disease: Nephropathy - minimize by good glucose and BP control. Characterised by microalbuminaemia. Worsens to proteinuria. ACEI slows progression.
NICE Guidelines (2009 & 2015)
Slide 25
PVD & Neuropathy
Diabetic Foot care
Provide advice on good basic foot care, avoid narrow fitting, tight shoes
Keep toenails well trimmed, cut straight across
Seek attention of chiropodist/podiatrist if appropriate
Warn of danger signs - pins and needles
Get cuts, burns on feet treated
Watch for fungal infections
Slide 26
Driving
Need to inform DVLA if on insulin injections not on oral medication
If on oral medication advise patient to avoid delaying or missing meals and snacks
If had 2 or more episodes of hypo in last 12 months inform DVLA
Take breaks on long journeys
Always keep hypo treatments to hand in the car
Consider timing of meals and snacks
Be aware of hypo signs and stop driving
Declare diabetes when applying for motor insurance.
Slide 27
Medicine's Management & Optimisation
{kind=link}
MEDICINES OPTIMISATION
Ensure all appropriate drugs prescribed
Best choice of anti-diabetic agent
Correct dosage regime
Compliance with regime
Complications optimally managed
Education - eg - hypo, seeking help
Insulin - how to use, storage, test strips, monitors, diary
Caption: : If use insulin or medication to manage diabetes - entitled to free prescription with a medical exemption certificate - FP92A
Slide 28
Signposting - Diabetes UK
Integrated Care Approach
Integrated Care Approach
{kind=link}
Want to create your own Slides for free with GoConqr? Learn more.