15184221
Meningitis
- Anatomy of
the scalp,
meninges
and the BBB
- SCALP
- Skin
- Connective tissue
- Epicranial Aponeurosis
- Loose areolar tissue
- Pericranium
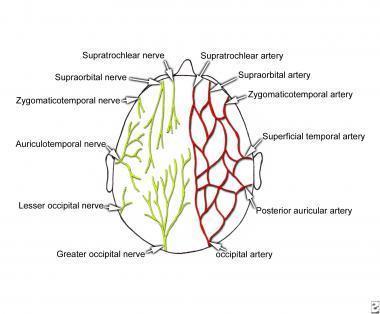
- Nerve and Arterial Supply of the Scalp
- Skin
- meninges
- Dural Folds
- The outer layer
of the dura
forms the
endocranium
- The inner layer
of the dura is
folded to form
- Falx cerebri
- Lies in the mid-sagittal
plane and separates
the two cerebral
hemispheres
- Lies in the mid-sagittal
plane and separates
the two cerebral
hemispheres
- Tentorium cerebelli
- Forms the roof of the posterior
cranial fossa, and separates the
cerebral hemispheres from the
cerebellum
- Forms the roof of the posterior
cranial fossa, and separates the
cerebral hemispheres from the
cerebellum
- Falx cerebri
- The outer layer
of the dura
forms the
endocranium
- Arachnoid Mater
- It consists of layers of connective tissue,
is avascular, and does not receive any
innervation.
- arachnoid granulations allow CSF to re-enter
the circulation via the dural venous sinuses.
- It consists of layers of connective tissue,
is avascular, and does not receive any
innervation.
- Pia Mater
- It is the only covering to follow the contours of the
brain (the gyri and fissures.
- it is highly vascularized, with blood vessels
perforating through the membrane to supply the
underlying neural tissue.
- It is the only covering to follow the contours of the
brain (the gyri and fissures.
- Dural Folds
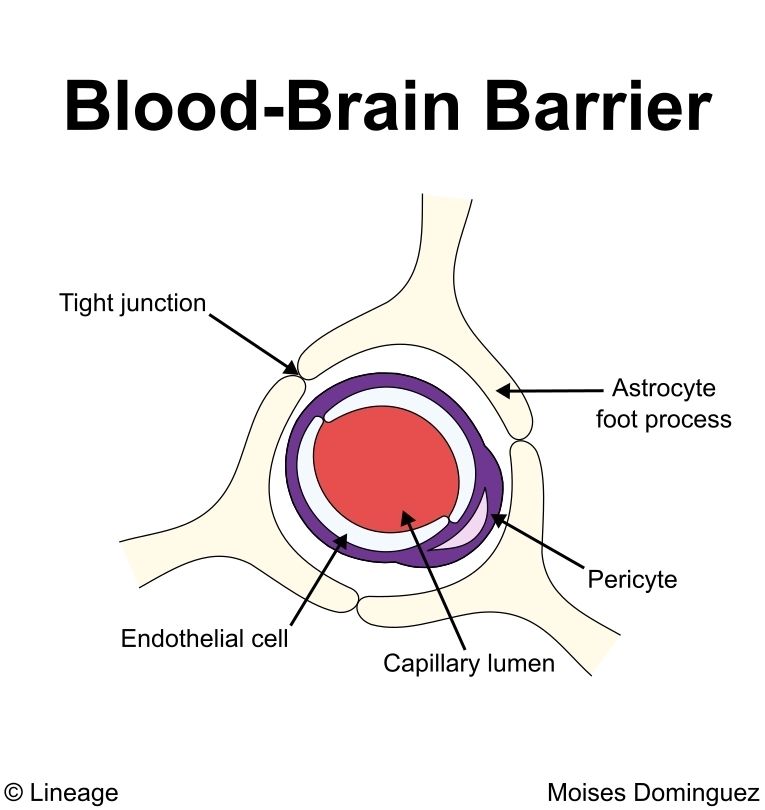
- Blood Brain Barrier
- SCALP
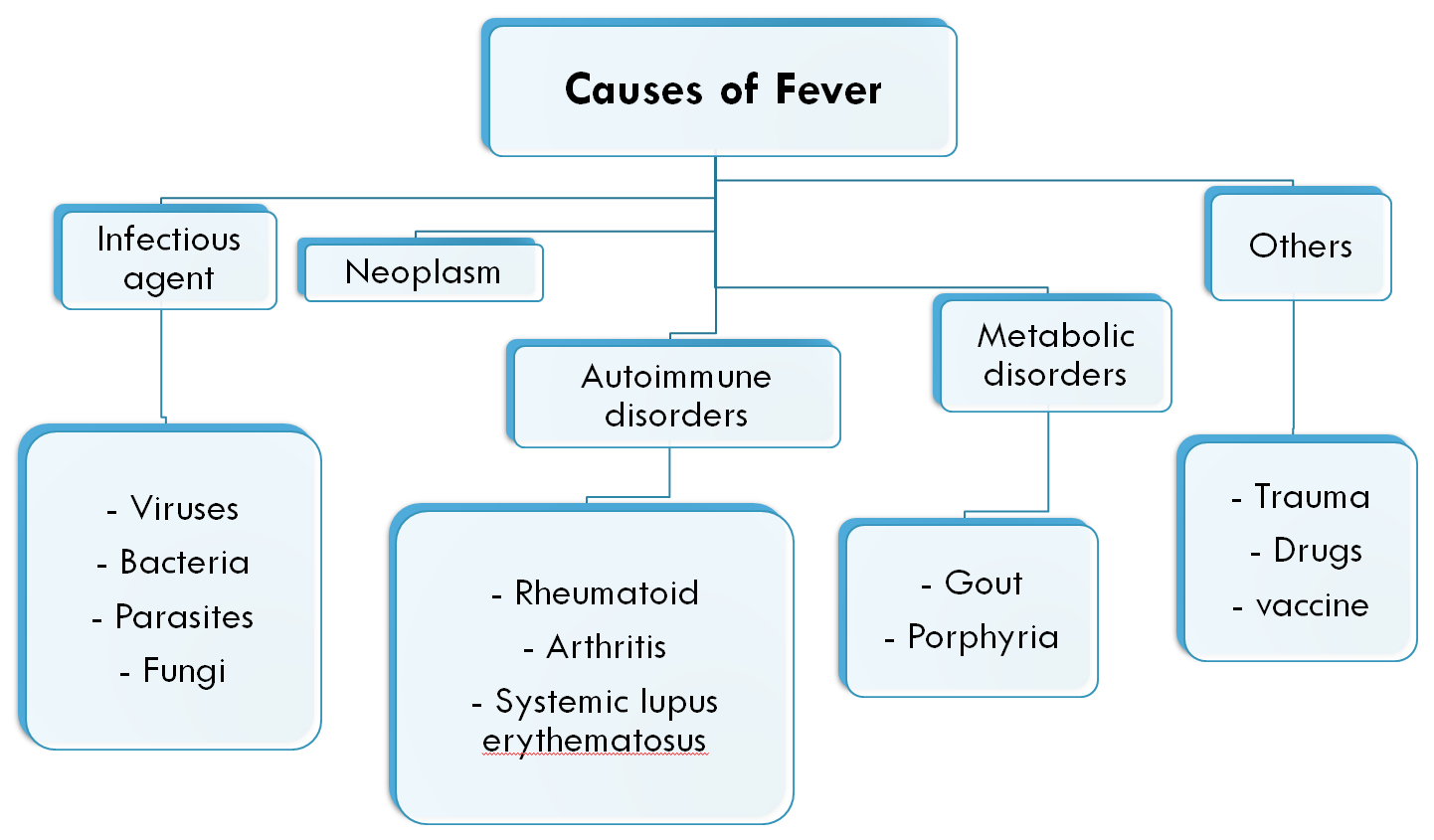
- Fever
- Pathophysiology
- pyrogens
- macrophages and
immune cells are
activated
- cytokines
- Pyretic cytokines: IL-1, IL-6, IL-8 macrophage inflammatory protein 1b, interferon gamma.
- activate phospholipase
- will induce the
production of
PE2
- change the temperature set point
- change the temperature set point
- will induce the
production of
PE2
- Pyretic cytokines: IL-1, IL-6, IL-8 macrophage inflammatory protein 1b, interferon gamma.
- cytokines
- macrophages and
immune cells are
activated
- pyrogens
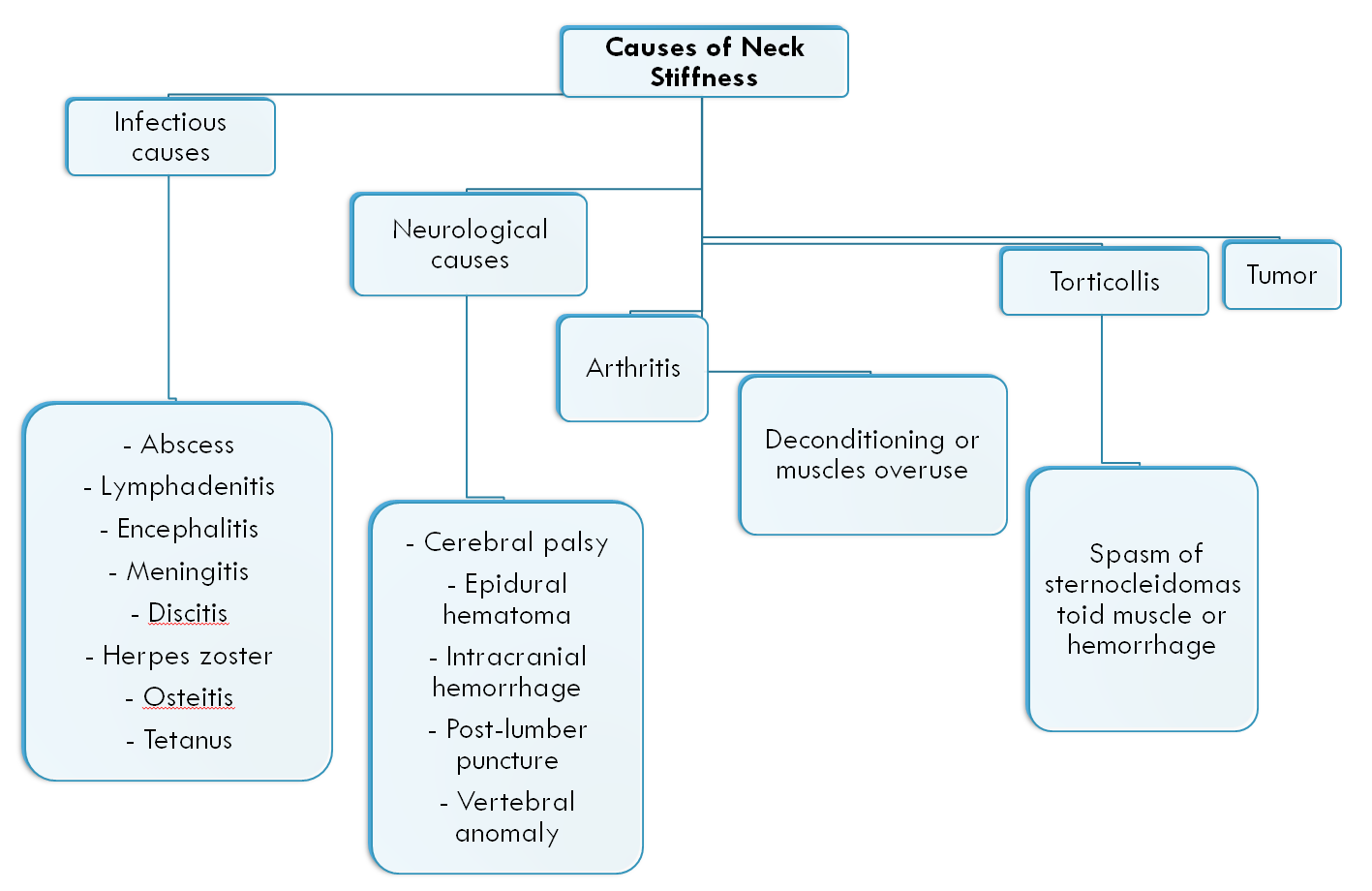
- Differential Diagnosis
- Pathophysiology
- Differential Diagnosis of Stiff Neck
- Epidemiology of
Neisseria
Meningitides
- Meningitis due to
Neisseria Meningitides
has the highest
incidence worldwide in
Africa, exactly in a
region of Sub-Saharan
Africa (Meningitis belt).
- This region is
hyper-endemic and
extends from
Senegal to Ethiopia.
- In the meningitis belt,
350 million people at
least are at risk of
getting meningitis in the
annual epidemics.
- Meningitis due to
Neisseria Meningitides
has the highest
incidence worldwide in
Africa, exactly in a
region of Sub-Saharan
Africa (Meningitis belt).
- Meningitis
Definition
- is an inflammation
(infection) of the
meninges also
involves the fluid
(CSF) surrounding
the brain and
spinal cord
- is an inflammation
(infection) of the
meninges also
involves the fluid
(CSF) surrounding
the brain and
spinal cord
- Meningitis
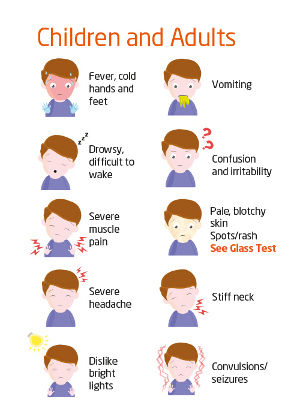
Clinical Picture
- Pathophysiology of meningitis
- Bacteria
- Penetrates BBB; endotoxin
and inflammatory
mediators initiate a CSF
inflammatory response
- Causing leakage of protein and
fluid out of the cerebral
vasculature
- Causing cerebral edema
and cerebral vascular
thrombosis
- Edema and increased
intracranial pressure
- Reduction in cerebral
perfusion and
cerebral infarction
- Brain death
- Brain death
- Reduction in cerebral
perfusion and
cerebral infarction
- Edema and increased
intracranial pressure
- Causing cerebral edema
and cerebral vascular
thrombosis
- Causing leakage of protein and
fluid out of the cerebral
vasculature
- Penetrates BBB; endotoxin
and inflammatory
mediators initiate a CSF
inflammatory response
- Bacteria
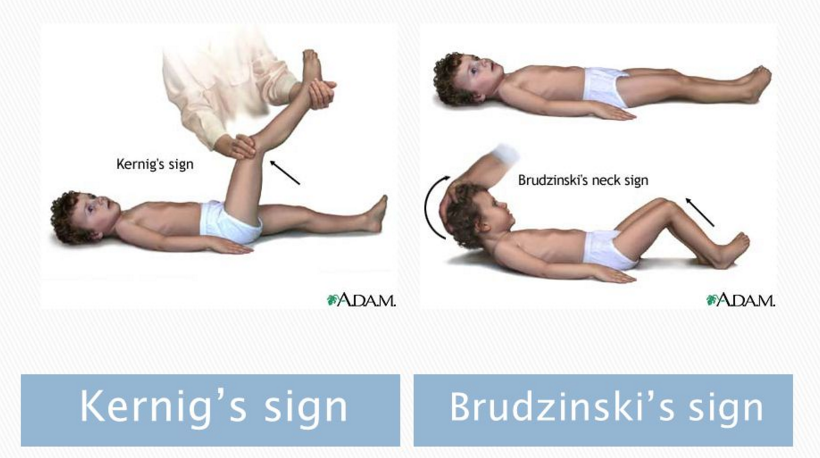
- Kernig’s sign
- • Positive Kernig’s sign
happens when the patient
experiences back pain or
when he can’t extend his
knee.
- • Positive Kernig’s sign
happens when the patient
experiences back pain or
when he can’t extend his
knee.
- Brudzinski’s sign
- • Positive brudzinski’s sign
happens when involuntary
flexion of knee and hip
happens.
- • Positive brudzinski’s sign
happens when involuntary
flexion of knee and hip
happens.
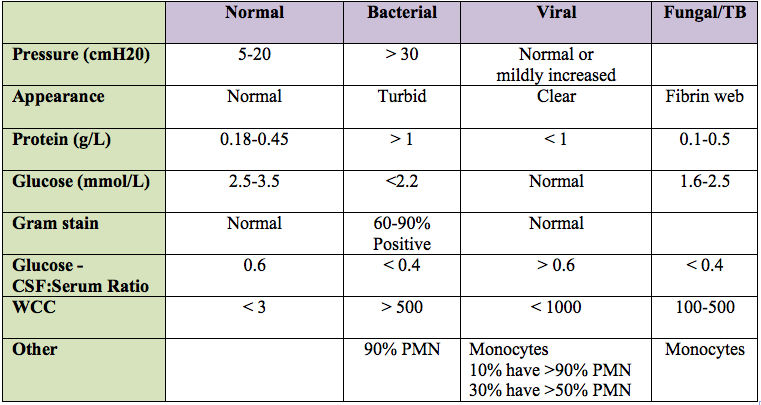
- CSF
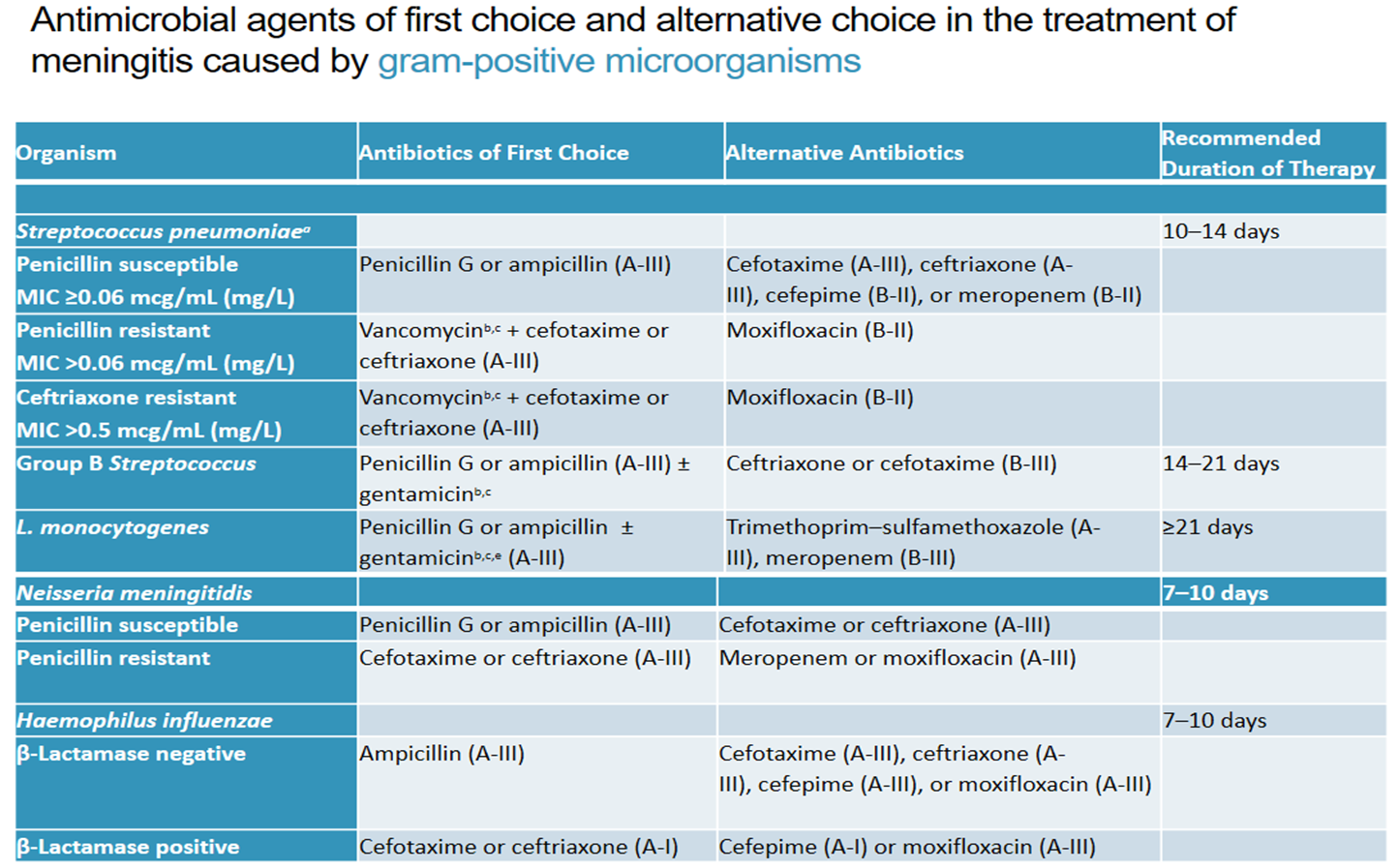
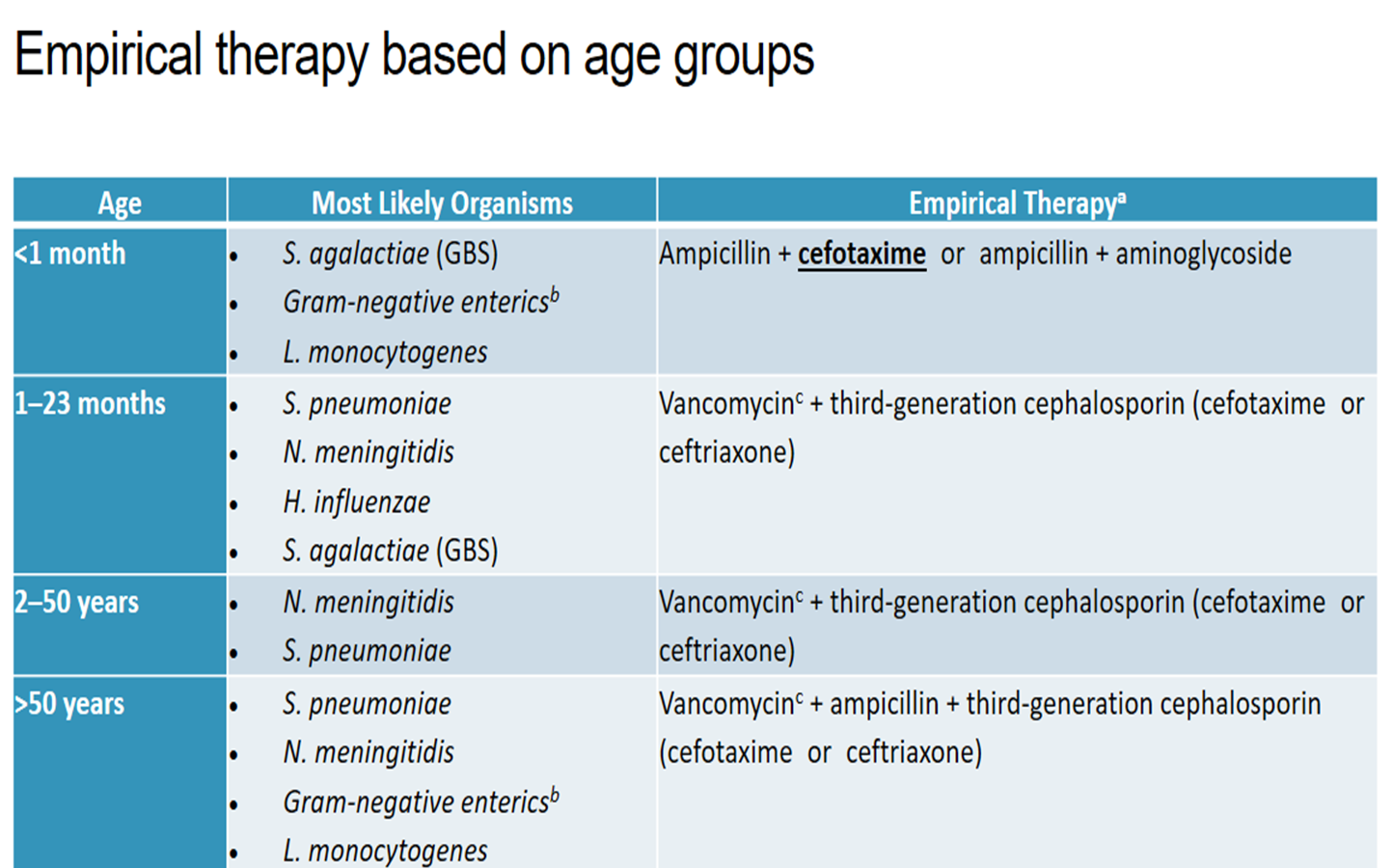
- Management of Meningitis
- Aim of Management
- Eradicate Infection
- Alleviate sings &symptoms
- Prevent complications
- Eradicate Infection
- Aim of Management
- Prevention &
Chemoprophylaxis
- For Anyone who has been in close contact with a
meningitis patient within seven days before the
onset of the disease is at increased risk of
contracting it themselves. With meningococcal
and Hib infections, preventative antibiotics are
usually offered to close contacts. These reduce,
but cannot eliminate, the risk of family members
or other close contacts becoming ill.
- Vaccine – pre-exposure prophylaxis
- Rifampin and ciprofloxacin - ideally within 24
hours after the case is identified
- Vaccine – pre-exposure prophylaxis
- The most effective way to protect against
certain types of bacterial meningitis is to
complete the recommended vaccine
schedule.
- There are vaccines for
three types of bacteria
that can cause
meningitis:
- Streptococcus pneumoniae (pneumococcus)
- Neisseria meningitidis (meningococcus)
- Meningococcal conjugate
vaccines (Menactra)- Covers
Serogroups A, C, Y and W-135
- Serogroup B meningococcal vaccines
(Bexsero) recommended dose of vaccine is a
single 0.5-mL subcutaneous injection
- Meningococcal conjugate
vaccines (Menactra)- Covers
Serogroups A, C, Y and W-135
- Haemophilus influenzae type b (Hib).
- Streptococcus pneumoniae (pneumococcus)
- For Anyone who has been in close contact with a
meningitis patient within seven days before the
onset of the disease is at increased risk of
contracting it themselves. With meningococcal
and Hib infections, preventative antibiotics are
usually offered to close contacts. These reduce,
but cannot eliminate, the risk of family members
or other close contacts becoming ill.
- Complications of meningitis
- Hydrocephalus
- Hearing loss
- Seizures
- Thrombophlebitis
- Septicemia
(Waterhouse-Friderichsen
Syndrome)
- Death
- Hydrocephalus
- Prognosis of meningitis
- Bacterial Meningitis
- 48 – 72 hours following
initial treatment
- More likely to
experience
complications
- 48 – 72 hours following
initial treatment
- Viral Meningitis
- Recovery without
neurologic sequelae
- Recovery without
neurologic sequelae
- Bacterial Meningitis
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.