7060240
Beschreibung
Mindmap von Clodagh Mullins, aktualisiert more than 1 year ago
|
|
Erstellt von Clodagh Mullins
vor etwa 9 Jahre
|
|
Cardiovascular
System
- Anatomy
Cardiovascular
system
- Functions
- Transport
oxygen and
nutrients to cells
- transport carbon
dioxide and other
metabolites away
from cells
- distribute
hormones
- defence
(immune
cells)
- thermoregulation
- Transport
oxygen and
nutrients to cells
- Heart
- ventricles
- atria
- inside lined with
endocardium,
outside epicardium
- valves
- semilunar,
both 3
cusps
- AV, LHS mitral=
BICUSPID RHS
TRICUSPID
- semilunar,
both 3
cusps
- chordae
tendinae +
papillary
muscle
- ventricles
- Cardiac
Skeleton
- non
conducting
connective
tissue
- structural
integrity
- break up
continuity
between A and V
allow separate
contraction
- non
conducting
connective
tissue
- Large Vessels
- VEINS
- bigger
- may have
valves
- less muscle
- most blood is
sitting in the
venous
system
- bigger
- ARTERIES
- Thicker
muscle
- elastic to
allow for
stroke volume
- arterioles- resistance
vessels decrease in
diamater decrease blood
pressure, increase
resistance to blood flow
- Thicker
muscle
- VEINS
- Small Vessels
- arterioles and
venules rally
thin muscle
layer
- microcirculation,
exchange happens
- Arteriole end- high
hydrostatic pressure
forces fluid out into
tissues
- Venous end- osmotic
pull from proteins in
capillary returns fluid
to blood
- starling forces
- lymphatic system
returns the rest to
CVS via lymphatic
duct
- Arteriole end- high
hydrostatic pressure
forces fluid out into
tissues
- arterioles and
venules rally
thin muscle
layer
- Functions
- Regulation
heartbeat/
cardiac cycle
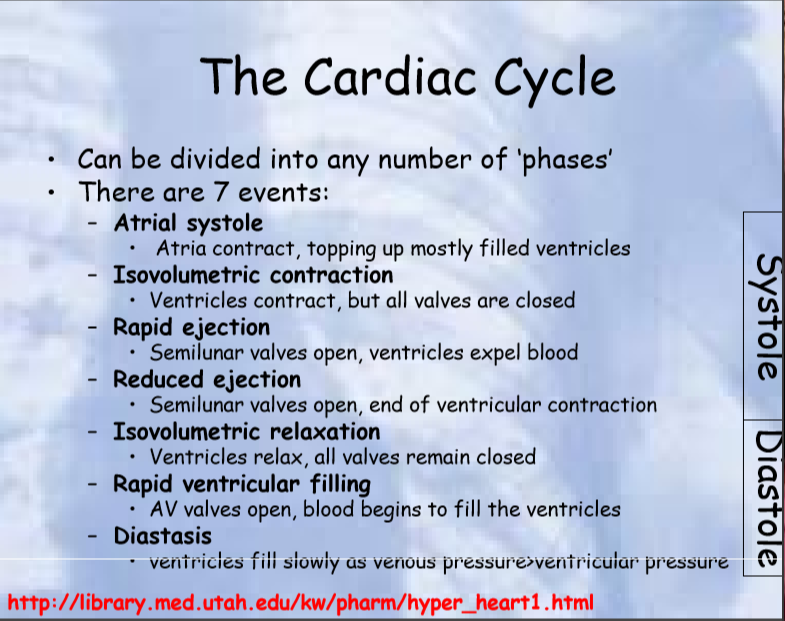
- Atrial Systole>Ventricle
Systole>ejection of
blood, diastole, ventricle
and arteries fill
- electrically- Sinoatrial node
(atria contract),
atrioventricular node,
bundle of His, purkinje
fibres- ventricles contract
- Influence
heart rate?
- parasympathetic,
vagus nerve
innervates SAN and
AVN
Anmerkungen:
- dominant at rest
- Adrenergic nerve
innervate SAN and
AVN
- parasympathetic,
vagus nerve
innervates SAN and
AVN
- cardiac muscle
- cardiac muscle can
beat spontaniously
generating own
action potential
- functional
syncytium- cells
electrically coupled
by intercalated
discs
- v central nuclei
- calcium-induced
calcium
release
excitation
coupling
Anmerkungen:
- calcium ions enter the cell deplarising it, this triggers calcium ions to be released from the sarcoplasmic reticulum so the muscle contracts
- cardiac muscle can
beat spontaniously
generating own
action potential
- CARDIAC ACTION
POTENTIALS IN
SAN
- 1- Slow region of gradual
depolarisation thanks to
sodium ion leak channels
letting sodium ions into
the cell
- 2-depolarisation
reaches a threshold
value and voltage
gated calcium ion
channels open
- 3- calcium ions rush
into the cell causing
rapid depolarisation
- 1- Slow region of gradual
depolarisation thanks to
sodium ion leak channels
letting sodium ions into
the cell
- CARDIAC ACTION
POTENTIALS IN THE
VENTRICLES
- 1- Fast sodium ion
channels open causing
rapid depolarisation
- 2- at a threshold
the fast sodium
ion channels
close
- 3-plateu as calcium
ions enter via
voltage gated
channels
- 4- repolarisation
- 1- Fast sodium ion
channels open causing
rapid depolarisation
- Atrial Systole>Ventricle
Systole>ejection of
blood, diastole, ventricle
and arteries fill
- Regulation
of Cardiac
Output
- Cardiac output=
stroke volume x
heart rate
Anmerkungen:
- so to alter cardiac oputput we must either alter stroke volume or heart rate
- Altering
heart
rate
- SAN-
innervated by
SNS and PNS
- PNS releases acetylcholine
which closes the sodium
ion leak channels so it
takes longer to reach
threshold value
- SNS- releases
noradrenaline binds to
beta-adrenoreceptors
to open more sodium
ion leak channels
- PNS releases acetylcholine
which closes the sodium
ion leak channels so it
takes longer to reach
threshold value
- AVN
innervated
by both
- PNS increases
refractory period,
SNS decreases
refreactory period
- PNS increases
refractory period,
SNS decreases
refreactory period
- SAN-
innervated by
SNS and PNS
- increasing stroke
volume- myocardial
contractility
Anmerkungen:
- increase the force generated by the contractile cells in the heart
- ATRIAL MYOCYTES
respond to both
SNS and PNS
- VENTRICULAR MYOCYTES- does
not directly respond to PNS,
instead PNS affects SNS
decreasing noradrenaline
release
- PRELOAD
- filling
pressure of
the heart
- affected by
central venous
pressure
- INCREASED
PRELOAD=
INCREASED
VENTRICULAR
PRESSURE
- MORE BLOOD ENTERS
THE VENTRICLES SO
VENTRICLE MUSCLE IS
STREACHED
- increased strength
of contraction,
increases stroke
volume= increase
cardiac output
- increased strength
of contraction,
increases stroke
volume= increase
cardiac output
- STARLINGS LAW OF THE HEART- force
of muscle fibre contraction is
proportional to length of fibre, so if
we stretch the fibre we get a
stronger contraction
- filling
pressure of
the heart
- AFTERLOAD
- pressure against
which the heart
ejects
- determined by
arterial pressure
(resistance
vessels?)
- direct oposition to
ejection, increase
in afterload
decrease stroke
volume
- decrease
cardiac
output
- decrease
cardiac
output
- pressure against
which the heart
ejects
- Cardiac output=
stroke volume x
heart rate
- Regulation blood
pressure
- Mean
arterial
pressure (MAP)
- MAP= CARDIAC OUTPUT
X TOTAL PERIPHERAL
RESISTANCE
- to alter we must
either alter heart
rate, stroke volume
or resistance
- MAP= CARDIAC OUTPUT
X TOTAL PERIPHERAL
RESISTANCE
- Short term
regulation
- 1- changes in pressure sensed by
baroreceptors in adventitia of
corotid arteries and aortic arch
e.g. sense BP increase
- 2- impulses send from
baroreceptors to medulla
oblongata
- 3- increase PNS (vagal) output to decrease heart rate
therefore cardiac outptu
- 4- decrease sympathetic, decrease arteriolar tone (decrease
resistance, decrease cardiac contractility and heart rate
- 1- changes in pressure sensed by
baroreceptors in adventitia of
corotid arteries and aortic arch
e.g. sense BP increase
- Long
term
regulation
- if we increase circulating
blood volume, increase
preload, increase cardiac
output so increase MAP
- 1- Renin release stimulates
angiotensin II production
- 2- angiotensin II is a
vasoconstrictor incresaes
TPR and therefore MAP
- 3-stimulate ADH, retain water
increase circulating volume
- 4- aldesterone releaed so kidney
retains more sodium so even
more water is absorbed
- if we increase circulating
blood volume, increase
preload, increase cardiac
output so increase MAP
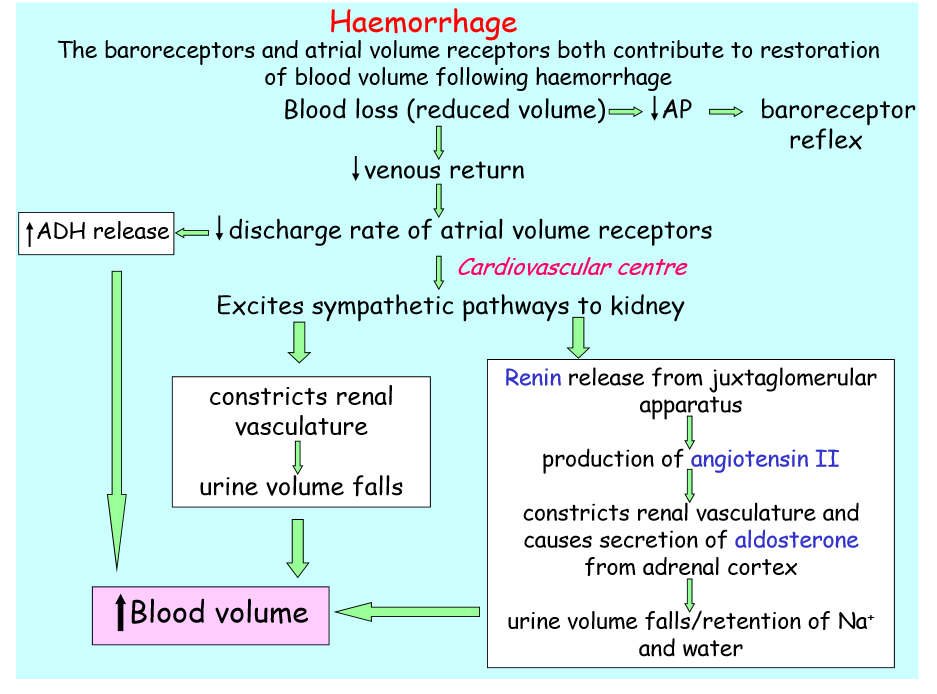
- KEY EXAMPLE- HAEMORRHAGE
- BLOOD LOSS- BIG
DECREASE IN VOLUME
- decrease
arterial
pressure
- barroreceptor
reflex
- barroreceptor
reflex
- decrease in venous return
- decrease discharge of atrial volume receptors
- ADH RELEASE
- EXCITE SYMPATHETIC PATHWAY TO KIDNEY
- renal
vasoconstriction
- incrase MAP
- incrase MAP
- Renin release
- angiotensin II produced
- vasoconstriction and
aldesterone production
- water retention= increase in mean
arterial pressure
- water retention= increase in mean
arterial pressure
- vasoconstriction and
aldesterone production
- angiotensin II produced
- renal
vasoconstriction
- ADH RELEASE
- decrease discharge of atrial volume receptors
- decrease
arterial
pressure
- BLOOD LOSS- BIG
DECREASE IN VOLUME
- Mean
arterial
pressure (MAP)
Medienanhänge
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.