Page 1
Lower Gastrointestinal Problems Medsurg p 1192-1195 Initially I wasn't able to see where LGP fit into the fluid and electrolyte imbalance chapter and what it had to do with the fluid care scenario, until I got to the clinical manifestations of a bowel obstruction and read that "With a bowel obstruction, there is retention of fluid in the intestine and peritoneal cavity, which can result in a severe reduction in circulating blood volume and lead to hypotension and hypovolemic shock. Ie. if high in pylorus, metabolic alkalosis may result from Hal from the stomach through vomiting or NG intubationObstruction in small intestine * onset: rapid * vomiting is frequent and copious * Pain: colicky, cramplike, intermitent * dehydration and electrolyte imbalance occur rapidly In our care scenario our patient is showing these symptoms, and our clinical group task is going to be focussing on shock. Malabsorption Syndrom Common Causes of Malabsorption biochemical or enzyme deficiencies bacterial proliferation small intestinal mucosal disruption disturbed lymphatic and vascular circulation surface area loss Malabsorption Syndrome • Malabsorption results from impaired absorption of fats, carbohydrates, proteins, minerals, and vitamins• The most common clinical manifestation of malabsorption is steatorrhea (bulky, foul-smelling, yellow-grey, greasy stools with putty-like consistency).Clinical Manifestations of MalabsorptionGastrointestinal weight loss diarrhea flatulence steatorrhea glossitis, cheilosis, stomatitis Hematological Anemia Hemorrhagic tendency Musculoskeletal bone pan tetany weakness, muscle cramps muscle wasting Neurological altered mental status parenthesis peripheral neuropathy night blindness Integumentary bruising dermatitis brittle nails hair thinning and loss Cardiovascular hypotension tachycardia peripheral edema Celiac Disease is an autoimmune disease characterized by damage to the small intestinal mucosa from the ingestion of wheat, barley, and the in genetically susceptible individuals.Lactase deficiency • Lactase deficiency is a condition in which the lactase enzyme is deficient or absent. Lactase is the enzyme that breaks down lactose into two simple sugars—glucose and galactose.• The symptoms of lactose intolerance include bloating, flatulence, crampy abdominal pain, and diarrhea. They may occur within a half hour to several hours after drinking a glass of milk or ingesting a milk product.• Treatment consists of eliminating lactose from the diet by avoiding milk and milk products and/or replacement of lactase with commercially available preparations. Short bowel syndrome • Short bowel syndrome (SBS) results from surgical resection, congenital defect, or disease-related loss of absorption. SBS is characterized by failure to maintain protein-energy, fluid, electrolyte and micronutrient balances on a standard diet. The length and portions of small bowel resected are associated with the number and severity of symptoms. Short bowel syndrome is characterized by failure to maintain protein-energy, fluid, electrolyte, and micronutrient balances on a standard diet. • The predominant manifestations of SBS are diarrhea, steatorrhea, and weight loss. There may be signs of malnutrition and multiple vitamin and mineral deficiencies (e.g., cobalamin and zinc deficiency, hypocalcemia). The length and the portions of small bowel resected are associated with the number and severity of symptoms. Resections of up to 50% of the small intestine cause little disturbance of bowel function. Collaborative CareOverall goal: electrolyte & fluid balance, normal nutritional status, control over diarrhea o Use TPN post bowel resection sx to maintain nutrition o Use PPIs to reduce gastric hyper secretion Diet: high in carbs and low in fat, soluble fibre and pectin will slow transit time o Eat 6 – 8 small meals/ dayOral supplements of calcium, zinc, and multivitaminsAntidiarrheal narcotics are effective at decreasing intestinal motilityMore limited resections, may use cholestryarmine to reduce diarrhea Intestinal obstruction • Intestinal obstruction occurs when a partial or complete obstruction of the intestine prevents intestinal contents from passing through the GI tract. The causes of intestinal obstruction can be classified as mechanical or nonmechanical. Mechanical obstruction may be caused by an occlusion of the lumen of the intestinal tract. A nonmechanical obstruction may result from a neuromuscular or vascular disorder. • Intestinal obstruction can be a life-threatening problem.• Carcinoma is the most common cause of large bowel obstruction, followed by volvulus and diverticular disease. Paralytic (adynamic) ileus (lack of intestinal peristalsis) is the most common form of nonmechanical obstruction.• Emergency surgery is performed if the bowel is strangulated, but many bowel obstructions resolve with conservative treatment.• With a bowel obstruction, there is retention of fluid in the intestine and peritoneal cavity, which can result in a severe reduction in circulating blood volume and lead to hypotension and hypovolemic shock.Clinical Manifestations of Small and Large Intestinal ObstructionsEtiology and patho: * Normally 6 – 8 L of fluid enter small bowel/ day o Most water is absorbed before it reaches the colon o Fluid and gas and intestinal contents build up prior to the obstruction – distension and bowel collapse o Increase in pressure => increased capillary permeability and extravsation of fluids and electrolytes into peritoneal cavity * Leads to edema, congestions and necrosis from impaired blood supply and possible rupture of bowel * With a bowel obstruction, there is retention of fluid in the intestine and peritoneal cavity, which can result in a severe reduction in circulating blood volume and lead to hypotension and hypovolemic shock. * Location of obstruction determines extent of imbalance: o Ie. if high in pylorus, metabolic alkalosis may result from Hal from the stomach through vomiting or NG intubationObstruction in small intestine * onset: rapid * vomiting is frequent and copious * Pain: colicky, cramplike, intermitent * dehydration and electrolyte imbalance occur rapidly * Feces for a short time * Ab distension may occur dependent upon location of obstruction Obstruction below proximal colon most GI fluids have been absorbed and just solid fecal matter accumulate and symptoms of discomfort appear, greater chance of metabolic acidosis * Onset: gradual * Pain: low-grade, cramping ab pain * Absolute constipation * Greatly increased ab distension * At end stages, may vomit fecal matter * Paralytic Ileus: generalized sense of discomfort * Emergency surgery is performed if the bowel is strangulated, but many bowel obstructions resolve with conservative treatment. Nursing Management: Intestinal Obstruction Assessment: * Get detailed hx: type and location of obstruction with characteristic symptoms Ab pain * Ab tenderness or rigidity * Onset, frequency, colour, odour and amount of vomitus * Bowel function: passage of flatus * Auscultate bowel sounds: will be more high pitched before obstruction * Inspect ab for scars, palpable masses and distension and observe muscles for guarding and tenderness Possible Nursing Dx: * Acute pain related to ab distension and increased peristalsis * Deficient fluid volume related to decrease in intestinal fluid absorption and loss of fluids secondary to vomiting * Imbalance nutrition: less than body requirements related to intestinal obstruction and vomiting Planning * Overall goal is to relief the obstruction and return to normal bowel function * Minimal to no discomfort * Normal fluid and electrolyte status * Maintain adequate nutrition Implementation * Monitor for I & O * IV admin if ordered * Serum electrolyte levels should be monitored * pt is often restless to try and relieve pain with position adjustments – try to promote restful enviro RNAO: BPG Assessing Pain Practice Recommendations for Pain Assessment: * Screen for the presence or risk of any type of pain * Perform pain assessment * Use a validated tool if person unable to self report * Explore person’s beliefs, knowledge and level of understanding about pain and pain management * Document Planning: * Collaborate with person to identify goals for pain management and suitable strategies to ensure comprehensive approach * Establish plan to incorporate goals and make sure to address: o Assessment findings o Persons belief and knowledge and level of understanding o Person’s attributes and pain characteristics Implementation * Implement plan while trying to minimize adverse effects of pharm interventions including: o Multimodal analgesic approach o Changing opioids (dose or routes0 o Prevention, assessment and management of adverse effects during the administration of opioid analgesics o Prevention , assessment and management of opioid risk * Evaluate any non pharm interventions for effectiveness * Teach caregiver about pain management strategies in their plan of care Evaluation * Reassess person’s response to pain management interventions consistently using the same re-evaluation tool. Frequency of reassessment is determined by: o Presence of pain o Pain intensity o Stability of person’s medical condition o Type of pain: eg. Acute vs persistant o Practice setting * Communicate and document person’s response to pain management
{kind=link}
{kind=link}
{kind=link}
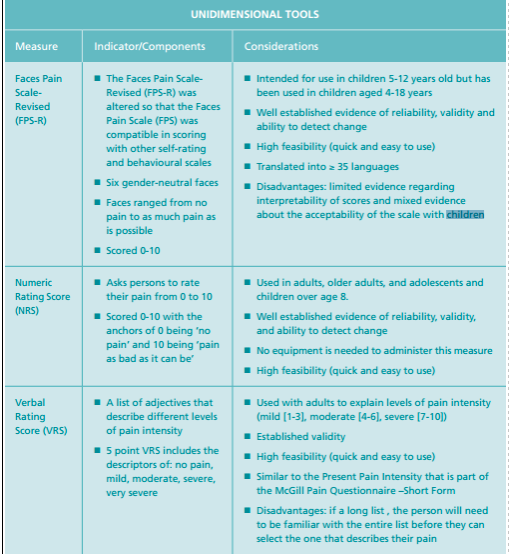
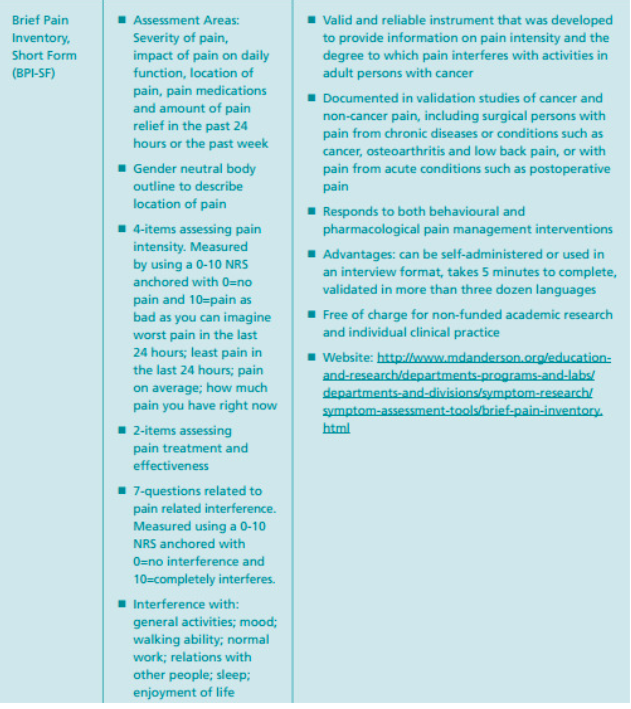
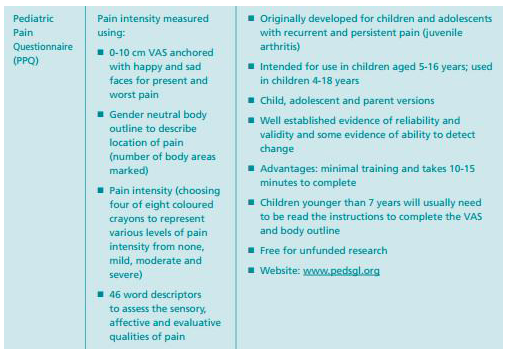
Pain Management Tools (RNAO, pp 82-4) I found it interesting to read the pain scales in more detail including the considerations and indicators. I could see it being useful to make flash cards listing some of the key points of each in case they want to ask when we might use them.
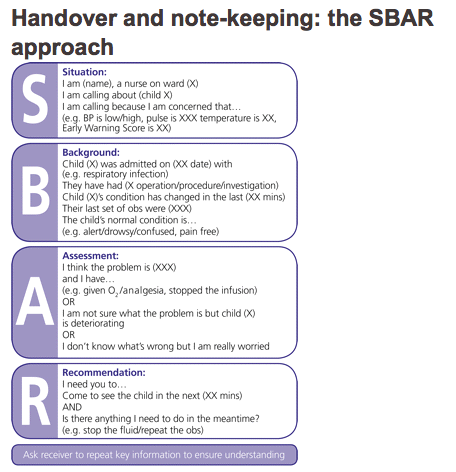
Learning Aims: Discuss the care of a patient who is experiencing an imbalance in fluids and electrolyte status Interpret diagnostic test results as they apply to pathophysiology and care of the patient. Identify appropriate communication with members of the health care team when reporting assessments/data using organized approach/tool such as SBAR Discuss the assessments and interventions related to acute pain Identify how the nurse can include the involvement of family members/significant others in the care of Mrs. Newman SBAR S – Situation - Briefly describe the current situation - Give a clear, succinct overview of pertinent issues B – background - Briefly state the pertinent history - What got us to this point? A –Assessment - Summarize the fact and give your best assessment - What is going on? Use your best judgement R – Recommendation - What actions are you asking for? - What do you want to happen next? SBAR technique provides a standardized framework for communication between members of the healthcare team about a patient’s condition. SBAR is an easy-to-remember mechanism useful for framing conversations, especially critical ones, requiring immediate attention and action. Using the SBAR model allows for an easy and focused way to set expectations for what will be communicated between members of the team, which is essential for developing effective teamwork and fostering a culture of patient safety. http://www.nursingcenter.com/journalarticle?Article_ID=715155 NG Tubes - Candidates include patients who have adequate digestion and absorption but cannot ingest, chew, or swallow food safely or in adequate amounts - A feeding tube is administered into the stomach or small intestine - For short term feeding nasal or oral feeding tubes are appropriate - NG feeding tubes are often inserted at the bedside without technological assistance - Most serious complication is inadvertent pulmonary intubation – enter the airway undetected and can lead to serious pulmonary injury - Feeding tubes are positioned into the small bowel to reduce the incidence of pulmonary aspiration of stomach contents - Variation in colour and pH of fluid withdrawn from feeding tube can help indicate tubes positioned in the stomach from those in the small intestine but the best measure is an X-ray - Carbon dioxide detectors can help locate the position of tubes during insertion by changing the colour of the sensor but X-ray is still more reliable - Maintaining and monitoring tube location during feeding and keeping the head-of-bed elevation at a minimum of 30 degrees effectively reduces aspiration and subsequent pneumonia - Measurement of gastric residual volumes is done routinely to identify risk for regurgitation and pulmonary aspiration of gastric contents; involves withdrawing and measuring the contents of the stomach at regular intervals - Oral hygiene and care of the nasal passage or tube insertion site promote patient comfort during tube feeding and can reduce complications Lewis, S.L., Heitkemper, M.M., Dirksen, S.R. (2014). Medical-surgical nursing in Canada: Assessment and management of clinical problems (3rd Canadian Ed.). Toronto, ON: Elsevier/Mosby.
{kind=link}
Normal ranges for an adult female Hematocrit: 0.37-0.47 - high Hemoglobin: 120-160 - normal WBC: 5-10 - high RBC: 4.2-5.4 Electrolytes: Na: 136-145 - low K; 3.7-5.2 - low Mg: 1.7-2.2 Ca: 8.5-10.2 Cl: 96-106 - low Amylase: 31-107 - high BUN: 3.6-7.1 Platelets: 150-400 CO2: 21-28 Creatinine: 44-97 Her results: what do they mean? Hct: high - may reflect hemoconcentration Hgb: normal WBC: high - can indicate strangulation or perforation Na: low - associated with small bowel obstruction K: low - associated with small bowel obstruction Cl: low - associated with small bowel obstruction CO2: low Amylase: high BUN: high - due to dehydration Creatinine: normal Platelets: normal Care for E & F balance: Strict input and output record IV fluids administered: solution of normal saline and potassium Serum electrolytes should be monitored Do labs diagnose her pain? Don't really diagnose her pain as much as they are used with the pain to diagnose the area of the bowel the obstruction occurs Reference: Med-Surg pg. 1194-1195
Want to create your own Notes for free with GoConqr? Learn more.