11715679
Description
Flashcards by Camille Bassil, updated more than 1 year ago
More
|
|
Created by lola_smily
over 9 years ago
|
|
|
|
Copied by Camille Bassil
almost 7 years ago
|
|
| Question | Answer |
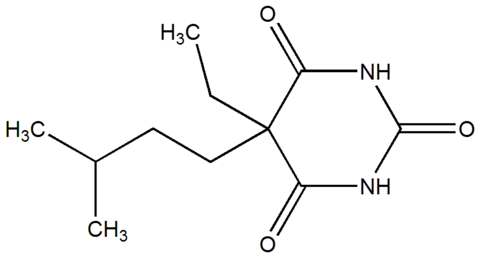
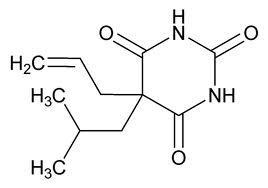
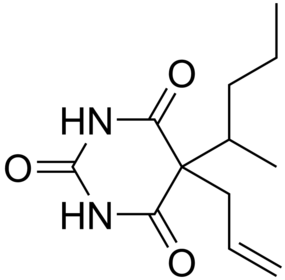
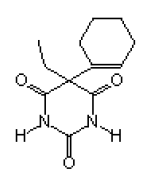
| amobarbital (barbituric acid derivatives) | |
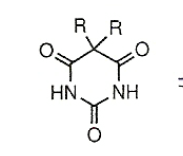
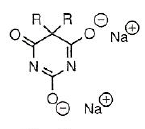
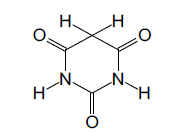
| barbituric acid | |
| butabarbital (barbituric acid derivatives) | |
| butalital (barbituric acid derivatives) | |
| dilactim | |
| hexahydropyrimidine 2,4,6-trione | |
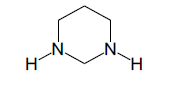
| hexahydropyrimidine | |
| mephobarbital (barbituric acid derivatives) SHORT doa RAPID ONSET | |
| methohexital (barbituric acid derivatives) | |
| monolactim | |
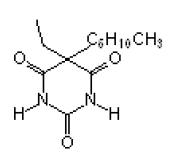
| pentobarbital (barbituric acid derivatives) | |
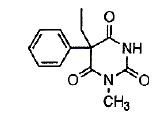
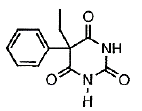
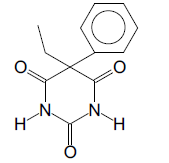
| phenobarbital (barbituric acid derivatives) | |
| pyrimidine | |
| secobarbital (barbituric acid derivatives) | |
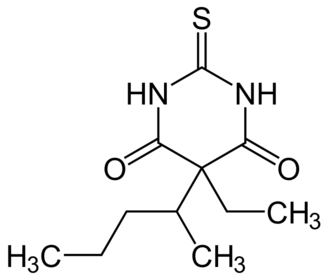
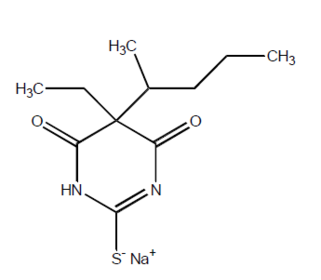
| thiopental (barbituric acid derivatives) | |
| butabarbital (barbituric acid derivatives) | |
| butathal (barbituric acid derivatives) | |
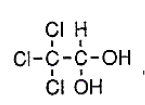
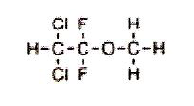
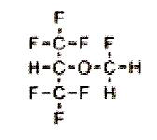
| chloral hydrate (non barbiturates) aldehydes useful for insomnia not analgesic initial acitivity | |
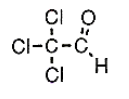
| chloral (non barbiturates) | |
| cyclobarbital (barbituric acid derivatives) | |
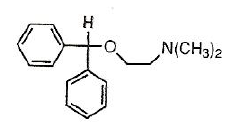
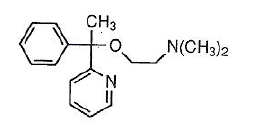
| diphenhydramine (antihistamine) cross BBB cause CNS effects | |
| doxylamine (antihistamines) | |
| hexethal (barbituric acid derivatives) | |
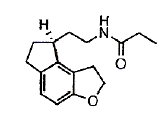
| indeno (5,6b) furan (modified melatonin receptor agonist) | |
| mephobarbital (barbituric acid derivatives) | |
| phenobarbital (barbituric acid derivatives) | |
| phenobarbital (barbituric acid derivatives) | |
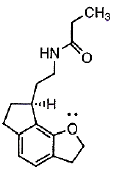
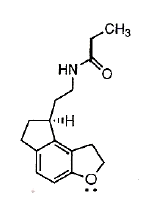
| ramelteon indeno (5,4b) furan (modified melatonin receptor agonist) higher affinity to MT1 receptor | |
| ramelteon (modified melatonin receptor agonist) | |
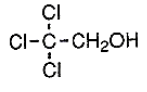
| trichloroethanol (non barbiturate) | |
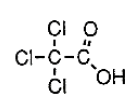
| tricholoroacetic acid (non barbiturate) | |
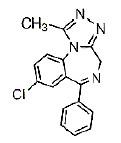
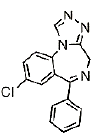
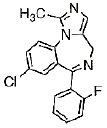
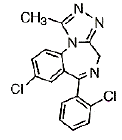
| alprazolam (xanax) | |
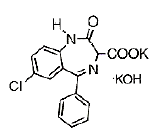
| clorazepate (tranxene) only BZD prodrug | |
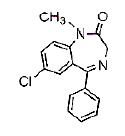
| diazepam (valium) long DOA Diazepam is metabolized to: Nordiazepam Temazepam oxazepam All metabolites are active | |
| estazolam sleep inducer in elderly onset of activity: 30min | |
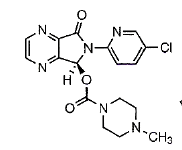
| eszopiclone cyclopyrrolone orally active well absorbed t 1/2: 6h •“S” isomer of zopiclone •Longer t ½ around 6hrs | |
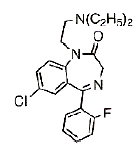
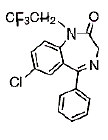
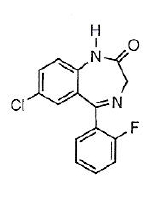
| flurazepam (dalmane) sleep inducer short half life: 2.4h very long DOA onset of activity: 30min The t ½ of flurazepam is 2.4hrs, metabolized into hydroxyethylflurazepam and N-desalkylflurazepam, both are active with t ½ of 3-4hrs and 47-100hrs, respectively. | |
| halazepam (paxipam) | |
| hydroxyethylflurazepam active long DOA half life: 3-4h | |
| metabolite of estazolam active short acting | |
| metabolite of triazolam active short acting | |
| midazolam (versed) | |
| n-desalkylflurazepam active long DOA half life: 47-100h | |
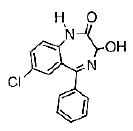
| oxazepam (serax) | |
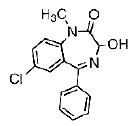
| temazepam (restoril) sleep inducer onset of activity:1-2h Temazepam is rapidly metabolized via direct conjugation with glucuronic acid | |
| triazolam (halcion) sleep inducer in elderly onset of activity:1-2h | |
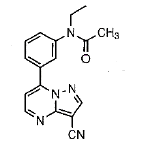
| zaleplon pyrazolopyrimidine orally active rapidly absorbed low bioavailabity: 30% t 1/2: 1hImidazopyridine food delays its effect all metabolites are inactive | |
| zopidem imidazopyridine orally active rapid onset: 1.4 h short acting t 1/2: 2h Food delays its effects •Short acting due to rapid oxidative metabolism into inactive metabolites highly bound to plasma proteins | |
| (+-) - nisoxetine non TCA secondary amines SNRI (NE) | |
| amoxapine non typical TCA secondary amine SNRI | |
| clorgyline MAOI (selective A) hypertensive crisis with tyramine | |
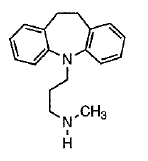
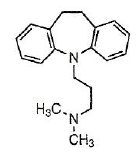
| desipramine 10,11-dihydrodibenzazepine ring secondary amine orally active TCA SNRI block muscarinic, alpha 1, H1 , Na channel CI with MAOI and TCA and SNRI => HYPERTENSION metabolized by CYP ( n desmethyl or hydroxylation Aadditive anticholinergic and sympathomimetic Na channel inhibitors : slow ventricular conduction at therapeutic dose | |
| iproniazid MAOI (non selective) hydrazine hypertensive crisis with tyramine | |
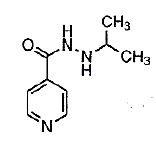
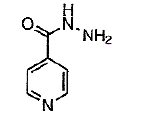
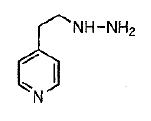
| isoniazid antituberculosis MAOI | |
| maprotiline TCA tetracyclic (bicyclic ring) SNRI block muscarinic, alpha 1, H1 , Na channel CI with MAOI and TCA and SNRI => HYPERTENSION metabolized by CYP ( n desmethyl or hydroxylation Aadditive anticholinergic and sympathomimetic Na channel inhibitors : slow ventricular conduction at therapeutic dose | |
| moclobemide MAOI (selective A) hypertensive crisis with tyramine | |
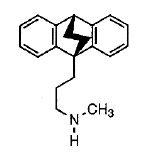
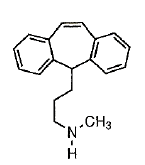
| nortriptyline 10,11-Dibenzocyclohepten-5- orally active TCA SNRIblock muscarinic, alpha 1, H1 , Na channel CI with MAOI and TCA and SNRI => HYPERTENSION metabolized by CYP ( n desmethyl or hydroxylation Aadditive anticholinergic and sympathomimetic Na channel inhibitors : slow ventricular conduction at therapeutic dose | |
| phenelzine MAOI (non selective) hydrazine hypertensive crisis with tyramine | |
| protriptyline dibenzocycloheptene ring orally active TCA SNRI block muscarinic, alpha 1, H1 , Na channel CI with MAOI and TCA and SNRI => HYPERTENSION metabolized by CYP ( n desmethyl or hydroxylation Aadditive anticholinergic and sympathomimetic Na channel inhibitors : slow ventricular conduction at therapeutic dose | |
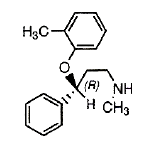
| R(-) - atomoxetine non TCA SNRI | |
| S,S- reboxetine non TCA SNRI | |
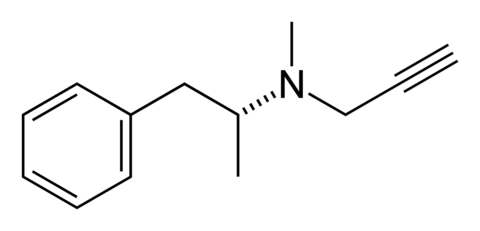
| selegiline MAOI (selective B) | |
| tranylcypromine MAOI (non selective) non hydrazine hypertensive crisis with tyramine | |
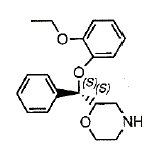
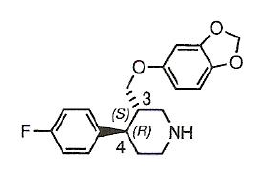
| (-) 3S,4R- paroxetine 2 chiral center with 4 possible stereoisomer 3S,4R (-) PAROXETINE Phenoxyphenylalkylamines piperidine ring SSRI non TCA potent and selective SERT little affinity for NET orally active metabolized by CYP2d6 into inactive catechol than methyl or glucuronide | |
| (+-)- talopram Phenoxyphenylalkylamines SSRI non TCA | |
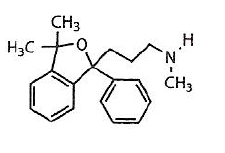
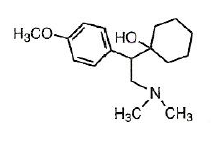
| (+-)- venlafaxine NSRI non TCA methoxyphenylethylamine metabolized into equipotent O-desmethyl venlafaxine 30x more potent for SERT than NET | |
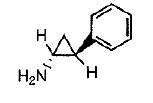
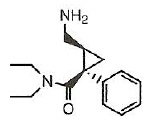
| (+-)-cis-milnacipran NSRI non TCA Phenylcyclopropanecarboxamide antidepressant similar to TCA and SSRI safe | |
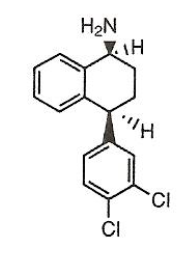
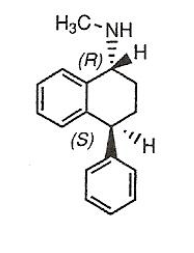
| 1S,4S-N-desmethylsertraline Phenylalkylamine derivatives SSRI active t 1/2=60-104h | |
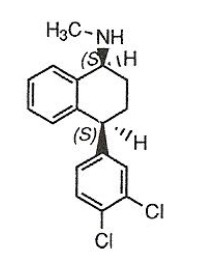
| 1S,4S-sertraline (zoloft) Phenylalkylamine derivatives SSRI potent 2 chiral centers t 1/2=26h active metabolite n desmethyl weak inhibitor of CYP3A4 | |
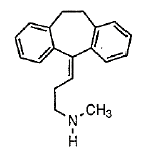
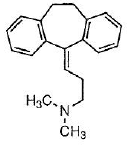
| amitriptyline NSRI TCA tertiary amine selective to serotonin as compared to 2ary greater anticholinergic, antihistaminic, antiadrenergic potent inhibitors of sodium channels increased cardiotoxicity and higher frequency of seizures SEROTONIN syndrome in DDI | |
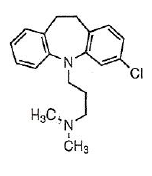
| clomipramine NSRI Dihydrodibenzazepine TCA most powerful antidepressant desmethyl active | |
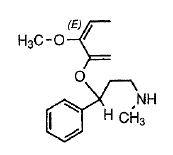
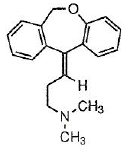
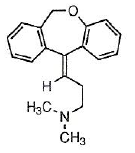
| doxepin (E-isomer) NSRI dibenzoxepine derivative less active Z ISOMER > E n desmethyl active | |
| doxepin (Z-isomer) NSRI dibenzoxepine derivative more active | |
| imipramine NSRI TCA tertiary amine selective to serotonin as compared to 2ary greater anticholinergic, antihistaminic, antiadrenergic potent inhibitors of sodium channels increased cardiotoxicity and higher frequency of seizures SEROTONIN syndrome in DDI | |
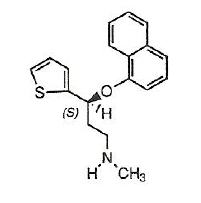
| S (+)- duloxetine NSRI non TCA fluoxetine analogue SERT > NET CYP2D6 Ndesmethyl active CYP3A4 4 hydroxyl active with sert>net | |
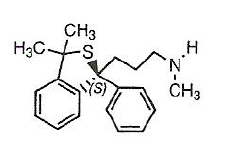
| S- talsupram Phenoxyphenylalkylamines isobenzothiophene potent NET INHIBITOR active | |
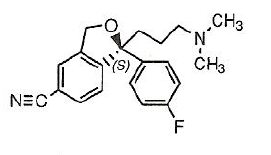
| S-citalopram Phenoxyphenylalkylamines isobenzofuran SSRI orally active N DESMETHYL ACTIVE S enantiomer 27 X more potent | |
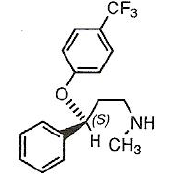
| S-fluoxetine (prozac) Phenoxyphenylalkylamines 3-phenoxy-3phenylpropylamine SSRI S isomer more potent (2x) than R orally active | |
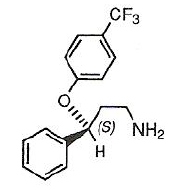
| S-norfluoxetine Phenoxyphenylalkylamines SSRI S isomer more potent (7x) than R | |
| tametraline Phenylalkylamine derivatives SSRI | |
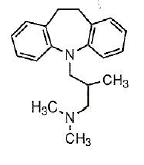
| trimipramine NSRI dihydrodibenzazepine TCA low affinity by 100 to both transporters desmethyl is active | |
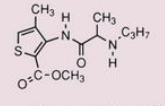
| articaine local anesthetic amino amides | |
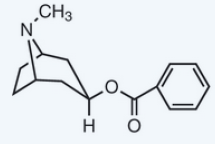
| atropine local anesthetic low activity toxic/eye irritation | |
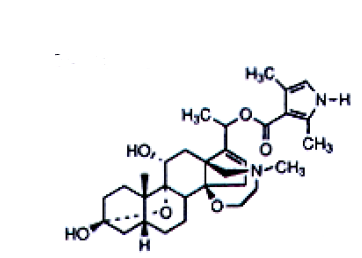
| batracotoxin local anesthetic alkaloid from skin of poison arrow frog extremely toxic/not used | |
| benoxinate local anesthetic amino ester | |
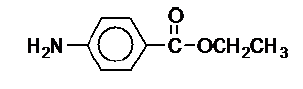
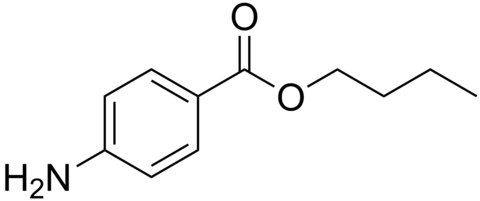
| benzocaine local anesthetic amino ester tongue numbness poor water solubility | |
| benzoyltropine local anesthetic decarbomethoxy derivative potent no addiction tissue irritation | |
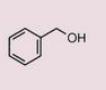
| benzyl alcohol local anesthetic alcohol | |
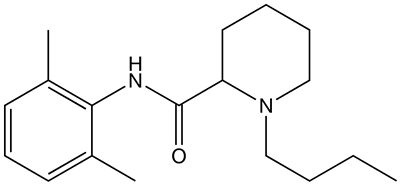
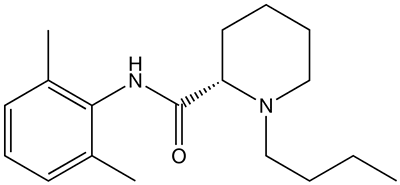
| Bupivacaine local anesthetic amino amides long acting | |
| Butamben local anesthetic amino ester | |
| chloroprocaine local anesthetic amino ester | |
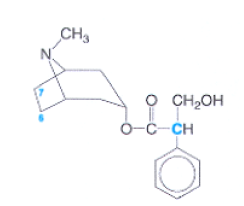
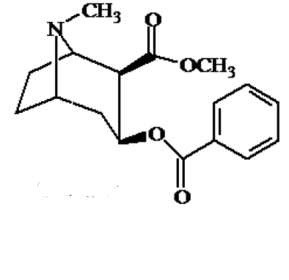
| cocaine local anesthetic addictive toxic unstable allergic | |
| dibucaine local anesthetic amino amides | |
| dyclonine local anesthetic amino ketone | |
| etidocaine local anesthetic amino amides long acting | |
| eugenol local anesthetic phenol | |
| glycinexylidide metabolite of lidocaine active toxic (CNS side effect) | |
| homatropine weak local anesthetic more active less irritating | |
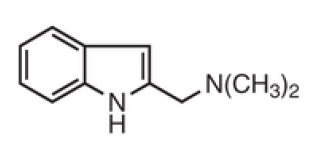
| isogramine local anesthetic amide type indole tongue numbness | |
| Levobupivacaine local anesthetic amino amides | |
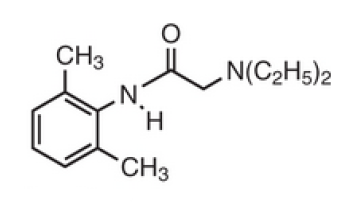
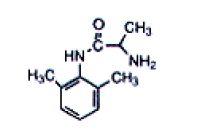
| lidocaine local anesthetic amide type non irritating stable less allergic potent | |
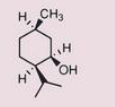
| menthol local anesthetic alcohol | |
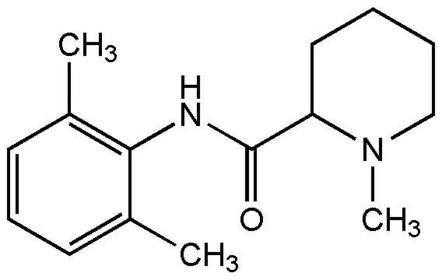
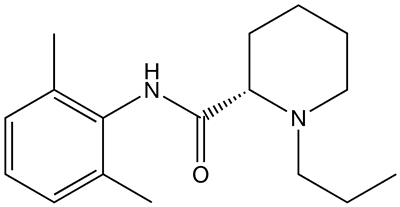
| mepivacaine local anesthetic amino amides | |
| monoethylglycinexylidide metabolite of lidocaine active toxic (CNS side effect) | |
| phenol local anesthetic | |
| pramoxine local anesthetic amino ether | |
| prilocaine local anesthetic amino amides | |
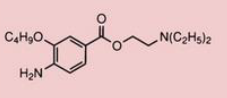
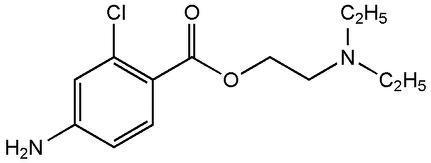
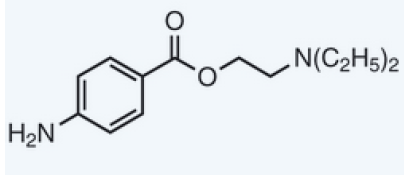
| procaine local anesthetic N,N-diethyaminoethyl ester water soluble less potent safe short acting stable at low pH | |
| proparacaine local anesthetic amino ester | |
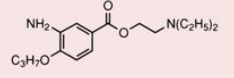
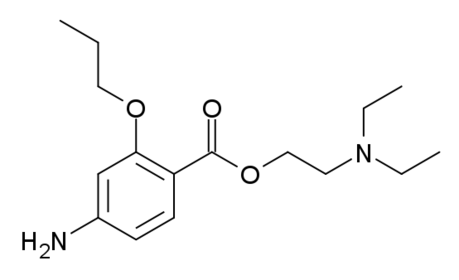
| Propoxycaine local anesthetic amino ester | |
| Ropivacaine local anesthetic amino amides | |
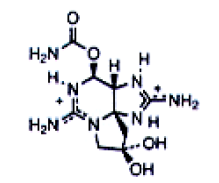
| saxitoxin STX local anesthetic alkaloid marine neurotoxin from ovaries of puffer fish clam poison extremely toxic/not used | |
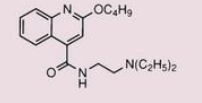
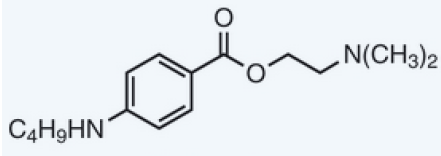
| tetracaine local anesthetic n-butylamino derivative high lipophilicity most potent (50x) long acting | |
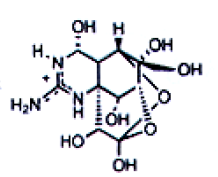
| tetrodotoxin TTX (hemiacetal form) local anesthetic alkaloid marine neurotoxin from ovaries of puffer fish extremely toxic/not used | |
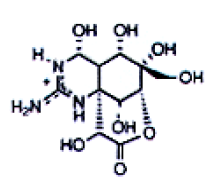
| tetrodotoxin TTX (lactone form) local anesthetic alkaloid marine neurotoxin from ovaries of puffer fish extremely toxic/not used | |
| tocainide lidocaine analogue no CNS side effect | |
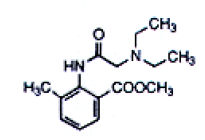
| tolycaine lidocaine analogue no CNS side effect | |
| cyclopropane volatile general anesthetic | |
| desflurane volatile general anesthetic potent rapid induction/ recovery (outpatient) no hepatotoxicity/ nephrotoxicity non corrosive to metals( stable) PUNGENT volatile | |
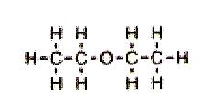
| diethyl ehter volatile general anesthetic high potency analgesic Neuromuscular relaxing effects flammable slow induction/recovery | |
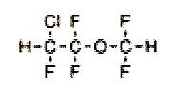
| enflurane volatile general anesthetic high potency high dose: convulsion and circulatory depression give F- and fluoromethoxy difluro acetic acid | |
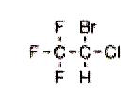
| halothane volatile general anesthetic potent sweet odor agent of choice in children rapid onset/recovery give HCL HBr HEPATOTOXICITY | |
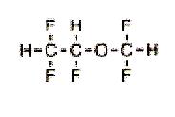
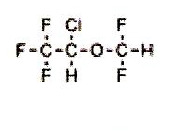
| isoflurane volatile general anesthetic pungent odor given IV fewer cardiovascular effects give F- and CF3COOH potent | |
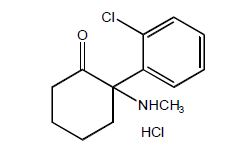
| ketamine hydrochloride IV general anesthetic very potent slow onset short DOA no muscle relaxation produce hallucination dissociative anesthesia norketamine in liver blocks NMDA receptor increase BP AND HR | |
| methoxyflurane volatile general anesthetic most potent highest solubility in blood slow inducto and recovery chemically unstable NEPHROTOXICITY | |
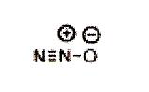
| nitrous oxide volatile general anesthetic least potent adjunct therapy colorless tasteless odorless irreversible oxidation of Co atom in VitB12 inactivation of enzymes methionine synthetase (myeline) thymidilate synthetase ( thymidine) | |
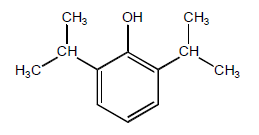
| propofol IV general anesthetic rapid induction and recovery increase GABA ergic neurotransmission within the CNS poor water soluble (soybean) glucuronude abd sulfate conjugayte outpatient (rapid induction/recovery vomiting ) | |
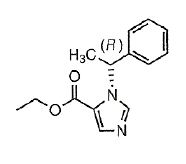
| R-etomidate IV general anesthetic Ester of carboxylated imidazole potent solubilized in 35% Propylene Glycol rapid/short acting lacks analgesia hydrolyzed by esterase SEIZURES | |
| sevoflurane volatile general anesthetic higher potency than desflurane low blood solubility rapid induction and recovery low pungency metabolized to hexafluoro isopropanol low hepato and nephrotoxicity | |
| thiopental IV general anesthetic rapid and pleasant induction short DOA enhance GABA ergic effect | |
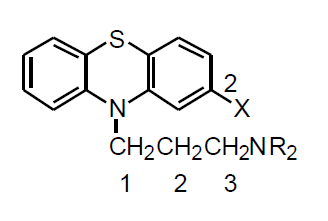
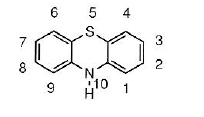
| phenothiazine typical neuroleptic | |
| phenothiazine typical neuroleptic | |
| piperazine moiety highest potency | |
| piperidine moiety | |
| pyrolidine moiety | |
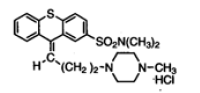
| thiothixene thioxanthene typical antipsychotic synthetic cis > trans double bond reduction reduce activity | |
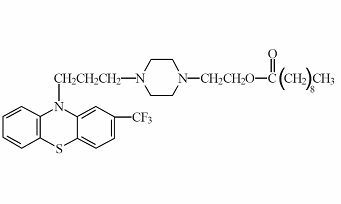
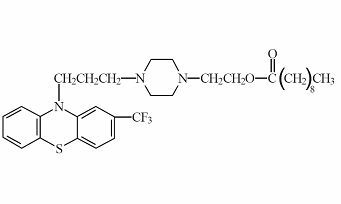
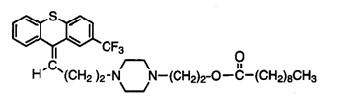
| fluphenazine decanoate phenothiazine typical neuroleptic prodrug long acting IM | |
| fluphenazine enanthate phenothiazine typical neuroleptic prodrug long acting IM | |
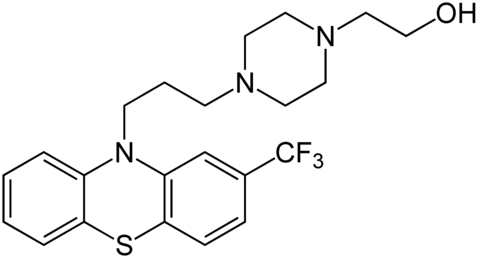
| fluphenazine phenothiazine typical neuroleptic most potent | |
| perphenazine enanthate phenothiazine typical neuroleptic pro drug | |
| flupenthixol decanoate thioxanthene typical neuroleptic pro drug | |
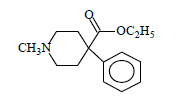
| meperidine metabolite of butyrophenone typical neuroleptic analgesic | |
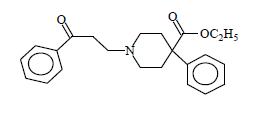
| propophenone metabolite of butyrophenone typical neuroleptic (200x) more potent than meperidine as analgesic | |
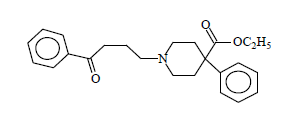
| butyrophenone typical neuroleptic analgesic | |
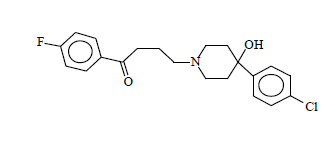
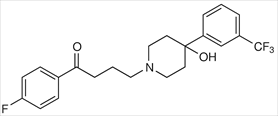
| haloperidol (haldol) prototype butyrophenone typical neuroleptic | |
| droperidol analogous of haloperidol typical neuroleptic short acting antiemetic | |
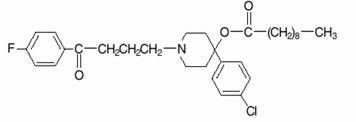
| haloperidol decanoate analogues of haloperidol typical neuroleptic | |
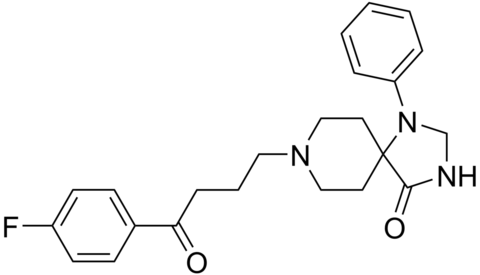
| Spiperone analogues of haloperidol typical neuroleptic | |
| trifluperidol analogues of haloperidol typical neuroleptic | |
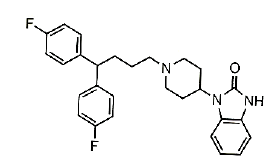
| primozide diphenylbutylpiperidine long DOA against schizophrenia against tourette's syndrome | |
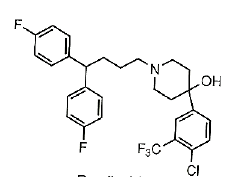
| penfluridol diphenylbutylpiperidine long DOA typical neuroleptic against schizophrenia | |
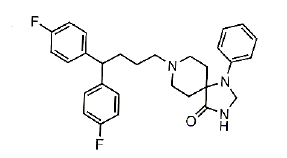
| fluspirilene diphenylbutylpiperidine long DOA typical neuroleptic against schizophrenia | |
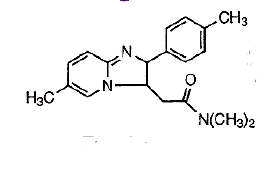
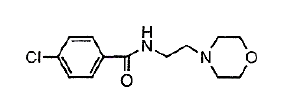
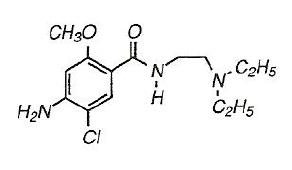
| metoclopramide benzamide derivative atypical neuroleptic antiemetic local anesthetic activity | |
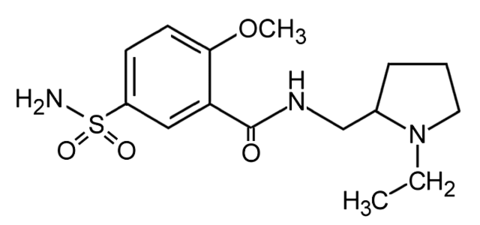
| S(-)-Sulpiride benzamide derivative atypical neuroleptic metoclopramide pyrrolidine ring derivative low EPS hydrophilic (poor oral absorption,low CNS--> low potency) | |
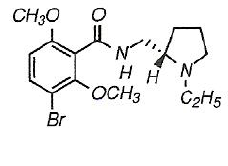
| S(-)-remoxipride benzamide derivative atypical neuroleptic metoclopramide pyrrolidine ring derivative potent low EPS/autonomic side effect APLASTIC ANEMIA | |
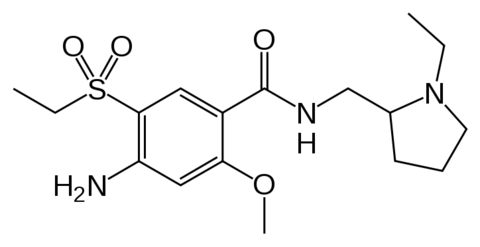
| Amisulpride benzamide atypical neuroleptic | |
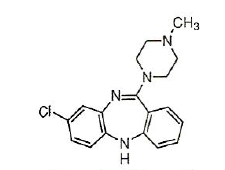
| clozapine (clozaril) benzazepine dibenzodiazepine derivative atypical neuroleptic low EPS orally active orally active and metabolized mainly by CYP3A4 to inactive desmethyl, hydroxyl, and N-oxide derivatives, with a half-life of approximately 12 hours. t1/2= 12h fatal agranulocytosis | |
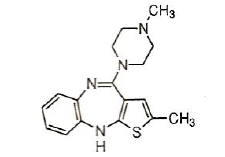
| olanzapine (zyprexa) benzazepine thienobenzodiazepine derivative atypical neuroleptic potent high EPS orally absorbed Olanzepine is well absorbed after oral administration and is metabolized mainly by CYPIA2 to inactive metabolites, with a variable half-life of approximately 20 to 50 hours. t1/2= 20-50h | |
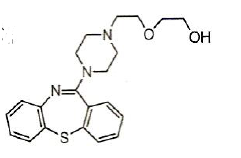
| quetiapine (seroquel) benzazepine dibenzothiazepine derivative atypical neuroleptic 100% bioavailable (orally active) first pass metabolism t1/2= 6hQuetiapine is 100% bioavailability first-pass metabolism yields at least 20 metabolites via CYP3A4 7-hydroxyl and N-desalkylquetapine are active metabolites | |
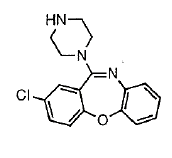
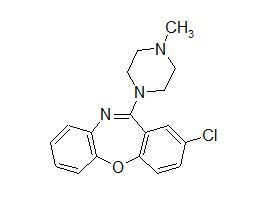
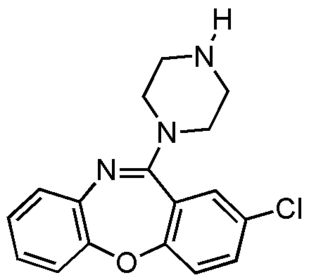
| loxapine benzazepine dibenzo-oxazepine derivative atypical neuroleptic more typical profile undergoes aromatic hydroxylation to yield several phenolic metabolites that have higher affinity for D2 receptors than the parent. undergoes N-demethylation to form amoxapine, which is used clinically as an antidepressant. | |
| amoxapine benzazepine dibenzo-oxazepine derivative n-demethylation of loxapine antidepressant | |
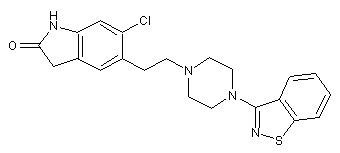
| risperidone benzizoxazole derivative atypical neuroleptic potent some EPS decrease schizophrenia orally absorbed give active metabolites undergoes hepatic CYP2D6 catalyzed 9-hydroxylation (active metabolite) and N-dealkylation. The half-life of risperidone and hydroxyrisperidone is about 22 hours t1/2= 22h | |
| Ziprasidone benzisothiazole derivative atypical neuroleptic potent orally active (60% bioavailable) t1/2= 6h extremely metabolizedorally active with 60% bioavailability t ½ is about 6 hours (increased by food) metabolized by aldehyde oxidase, which results in reductive cleavage of the S-N bond, and then by S-methylation. •Ziprasidone also can undergo N-dealkylation and S-oxidation by CYP3A4catalyzed | |
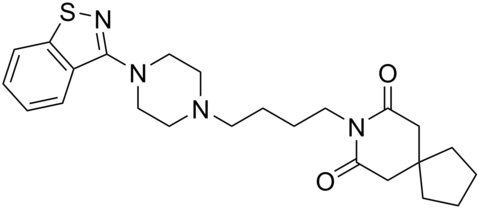
| Tiospirone benzisothiazole derivative atypical neuroleptic | |
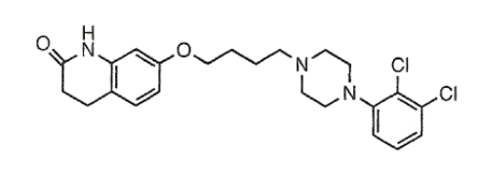
| aripiprazole arylpiperazine quinolinone derivative atypical neuroleptic low EPS/low hyperprolactinemia partial agonist activity at some D2 receptors | |
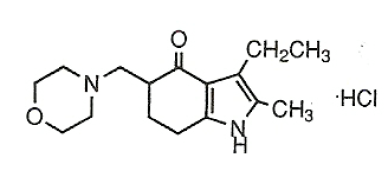
| molindone tetrahydroindolone derivative atypical neuroleptic less potent high EPS orally active/ rapidly absorbed some metabolites are active t1/2>24 h | |
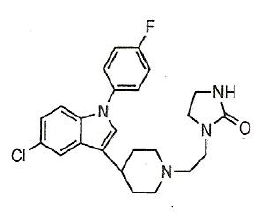
| sertindole indole derivative atypical neuroleptic low EPS against schizophrenia long acting non sedating |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.