12118466
Description
Flashcards by Dolu Falowo, updated more than 1 year ago
|
|
Created by Dolu Falowo
almost 8 years ago
|
|
| Question | Answer |
| What is Poiseuille's law? | Resistance is proportional to 1/radius^4 |
| Where is the highest resistance found? | In the large airways to medium-sized bronchi |
| Describe the general histology of the trachea | -Ciliated epithelium -Goblet cells -Mucous glands -Elastic cartilage ring -Smooth muscle in ligament |
| Describe the general histology of the bronchioles | -Smooth muscle -Ciliated epithelium |
| Describe the innervation of the airways How is it stimulated? | Parasympathetic nervous system ACh stimulates M3 receptors causing bronchoconstriction. The muscarinic antagonist, atropine reduces airway resistance |
| What type of innervation is not present in the airways? What is present instead? | There is no sympathetic innervation -Adrenaline can cause bronchodilation by binding to B2 receptors on smooth muscle -Also binds to B2 receptors on mast cells inhibiting activity -B2 stimulation promotes muco-ciliary escalator activity (moving foreign particles) |
| How does CO2 affect the airway diameter? | -Causes bronchodilation -Feedback mechanism builds up in under ventilated parts of the lung -Important for ventilation-perfusion matching |
| What do mast cells do? | -Present in airway walls -Mediators are released during degranulation causing bronchoconstriction -Releases histamines, platelet aggregating factor and leukotrienes |
| What do mechanical receptors do to airway diameter? | -Rapidly adapting receptors (RAR) cause bronchoconstriction -Slowly adapting pulmonary stretch receptors (PSR) cause bronchodilation eg. during a large breath |
| What is NANC innervation? | Non-adrenergic, non-cholinergic innervation -Causes bronchodilation -Transmitters included VIP and NO -Substance P can also cause bronchoconstriction is asthma |
| Describe radial traction | -Airways are embedded in lung parenchyma which splints airways open -Inflation increases radial traction and airway resistance is reduced |
| Describe alveolar interdependence Why is there higher resistance in COPD patients? | -Neighbouring alveoli share walls so mechanical tethering keeps airways open There is loss of radial traction and alveolar interdependence eg. emphysema destroys lung parenchyma |
| Describe what anti-cholinergics/muscarinic antagonists such as Ipratropium do? | -Blocks the bronchoconstricting action of ACh Ipratropium. Structure prevents systemic absorption (reducing systemic side effects) and blocks anti-inflammatory effect |
| Describe the physiology of those who have asthma | -Episodes of bronchoconstriction -Bronchial hypersensitivity -Mucosa inflammation and infiltration of immune cells (releases mediators causing bronchoconstriction) -Increased airway secretions |
| Describe the action of B2 agonists such as salbutamol and salmeterol/turbutaline | -Stimulates the AC/cAMP/PKA pathway to cause bronchodilation and reduce inflammation Salbutamol s/e: tachycardia, tremor, airway hyper-responsiveness. Symptomatic relief Salmeterol/turbutaline: slow-onset/long-acting |
| Describe the action of methylxanthines such as PDE inhibitors and theophylline/aminophylline | PDE inhibitors: increase cAMP, causing bronchodilation and reducing inflammation Theophylline/aminophylline: has a narrow therapeutic window. S/e: headache, restlessness, abdominal symptoms, arrhythmias. Use has declined |
| How would you test for asthma? | -Lower FEV1:FVC -Use low doses of a cholinergic agonist. There would be more bronchoconstriction than in a healthy person |
| Describe how monoclinal anti-IgE antibodies such as Omalizumab work | -S.c. injection -Reduces circulated IgE, mast cell degranulation and inflammation -Used to treat severe allergic asthma -Can cause anaphylaxis in rare instances |
| Describe aspirin-induced asthma Treatment adjunct? | -Sensitivity develops in adulthood -Women>men -Symptoms: rhinorrhea (runny nose), nasal congestion, sinusitis Montelukast |
| Describe how sodium cromoglicate/cromolyn works | -Prophylactic treatment (prevents disease) -Inhibits release of inflammatory mediators from mast cells and RAR axon reflexes -Mild s/e: coughing, wheezing, dry throat -Reduces need for corticosteroids/bronchodilators |
| Describe how corticosteroids such as Bleclamethazone work | -Reduces airway inflammation and hyper-responsiveness -Prevents rather than relieves Beclamethazone is metabolised to the active form in the lungs reducing systemic s/e. It represses genes used in inflammatory processes |
| Describe how drugs such as Zileuton and Montelukast targets leukotriene pathways | Zileuton: -leukotriene antagonist -has to be take 3-4x day (problems with patient compliance) Montelukast: -leukotriene antagonist -single daily dose -Used in severe chronic and exercise induced asthma -Bronchodilates -Reduces mucus secretion and inflammation |
| How do histamine receptor antagonists such as Ketotifen work? | -Hi-receptor antagonist -Anti-inflammatory -Reduces reliance on steroids and bronchoconstrictors -S/e: drowsiness |
| Describe the alveolar gas tensions. What do they set? What sets the PCO2 and PO2 in the blood leaving the lungs? | They are stable and so set stable arterial gas tensions The alveolar partial pressures |
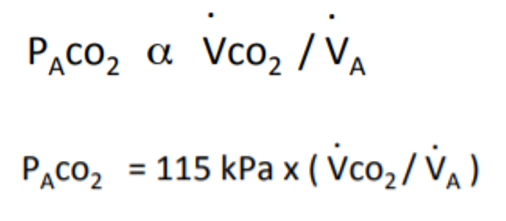
| What 2 factors determine alveolar PCO2 tensions? Describe their effects | Increasing V(dot) CO2 concentrates PACO2 Increasing V(dot)a dilutes PACO2 |
| What 2 calculations can be used to calculate PACO2? | |
| How does PACO2 remain constant? At what value is this? What is PaCO2 a clinical measure of? | If VA increases in proportion with VCO2 5kPA The adequacy of V(dot)A |
| Define hyper/hypoventilate | Hyper: ventilating alveolar gases more than metabolic need Hypo: not breathing enough for metabolic need |
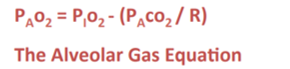
| What is the alveolar gas equation? | |
| Uses of the alveolar gas equation | Used to calculate PAO2 -P(A-a)O2 difference is calculated -If more than 1kPa, there is an impairment in the respiratory system |
| What is Graham's law? Does CO2 diffuse slower or faster than O2? | Diffusion in the gaseous phase is dependent on deltaP and is proportional to 1/(square root) MW MW= molecular weight Slower |
| What does diffusion of a gas through liquid depend on? | Concentration difference A more soluble gas maintains a higher concentration difference and diffuses easier |
| What is Henry's law? | Concentration of gas= partial pressure x solubility coefficient (alpha) |
| CO2 diffuses 20 times more easily than O2. What are the clinical implications of this? | Any diffusion limitations will show up firstly with O2 rather than CO2 transfer ie. hypoxia before hypercapnia |
| What is uptake of a gas into blood dependent on? | The partial pressure difference which is dependent on: -solubility -chemical combination |
| Equation for the diffusion constant How is it measured in a real life scenario? | Using CO as it has a high affinity for haemoglobin |
| What is the pulmonary diffusing capacity reduced by? | Reduced effective surface area: loss of lung tissue, airway obstruction, capillary obstruction, VQ mismatch Increased diffusion path length: thickened alveolar-capillary membrane, accumulation of lung fluid, increased intracapillary distance |
| How might a patient present clinically is their pulmonary diffusing capacity (DL) is reduced? | -Hypoxic -Cyanosis aggravated by exercise -Increased alveolar ventilation -Decreased PaCO2 -Normal ventilatory capacity |
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.