15090573
Description
Flashcards by Chloe Reynolds, updated more than 1 year ago
|
|
Created by Chloe Reynolds
about 6 years ago
|
|
| Question | Answer |
| What is primary PPH? | Loss of 500ml or more blood from the genital tract within 24 hours of the birth of the baby |
| What is Secondary PPH? | Abnormal or excessive bleeding from the birth canal between 24 hours and 12 weeks postnatally |
| Minor PPH? | 500ml-1000ml |
| Major PPH? | >1000ml |
| Gran-Mulltip? | >4 babies. Increase risk of PPH |
| 2 signs look for to establish if placenta has separated? | 1) Lengthening of the cord 2) Fresh blood |
| What is the risk of forcing the placenta prior to separation? | Uterine inversion |
| 4 general causes of PPH? | 1) Tone- uterus not contracted down. 2)Trauma-tear 3) Tissue- retained placenta tissue left in uterus 4) Thrombin- coagupathy |
| Drugs to use to pharmacologically promote uterine contraction? | 1) Syntometrine (2 doses) 2) Oxytocin (Syntocion infusion) 3) Misoprostol 4) Hemabate (PGF2a) |
| How to manually promote uterine contraction? | 1) uterine massage 2) Bimanual compression |
| 4 procedures used to stop bleeding? | 1) Hysterectomy 2) Balloon in uterus 3) embolisationof uterus 4) B-linch procedure |
| How much increased risk of thromboembolism by pregnancy? | X6 |
| How much increased risk of thromboembolism by C-section? | X10 |
| What % is the incidence of non-fatal PE or DVT in pregnancy normally compared to when have C-section? | Pregnancy= 0.5%-1.0% C-Section= 0.5% |
| What are the odds of maternal mortality from a thromboembolism? | Less than 1 in 1000 |
| What treatment for a woman who is pregnant with suspected VTE? | LMWH- e.g Enoxaparin (clexane) and dose is based on BOOKING WEIGHT of woman |
| What method is used to deliver placenta actively? | Syntometrine given and use of 'controlled cord traction' |
| Define an 'Ectopic' pregnancy? | Pregnancy occuring outside the uterine cavity |
| Rate of ectopic pregnancies? | 11/1000 (but is increasing ) |
| Maternal mortality with ectopic pregnancies? | 1/2500 |
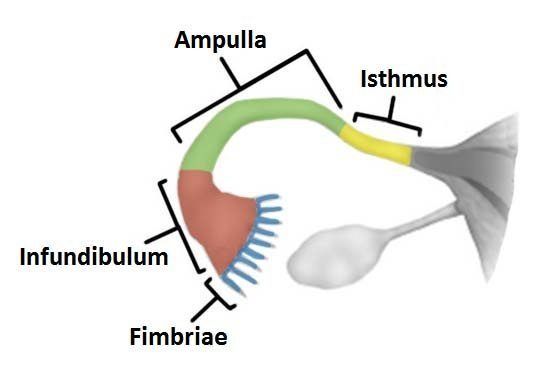
| Most common site of ectopic pregnancy? | In the Ampullary region of the fallopian tube (70%) |
| RF for an ectopic pregnancy? (6) | -Previous PID -Previous ectopic -Previous tubal pregnancy (steriliation, reversal) -Pregnancy in the presence of IUCD -POP -IVF |
| Symptoms of ectopic pregnancy? | -Lower abdo pain (due to distention of the tube or peritoneal irritation) -Vaginal bleeding -Should tip pain- diaphragmatic irritation -fainting- hypovolaemic |
| Signs of ectopic pregnancy? | - abdo tenderness + rebound/guarding -adnexal tenderness -Shock- tachy, hypotension, pallor |
| How to diagnose an ectopic pregnancy? | -Transvaginal USS |
| What is PUL? | Preganacy of Unknown Location- a positive pregnancy test with no signs of intra or extrauterine pregnancy on USS |
| What % of early pregnancies are PUL? | 15-20% |
| Methods of managing ectopic pregnancies? | 1) Expectant management (watch and wait) 2) Medical (methotrexate) 3) Surgical (salpingectomy or salpingotomy) |
| What is a 'threatened miscarriage'? | Vaginal bleeding at <24 weeks gestation |
| What is 'delayed (missed) miscarriage'? | Where there is a gestational sac but no fetal heartbeat |
| What defines 'recurrent misscarriages'? | 3 or more consecutive misscarriages without a known cause |
| What % do misscarriages make up on clincally diagnosed pregnancies? | 15-20% (1 in 5 pregnancies are misscarriages) |
| Most common cause of misscarriage? | Genetiv abnormalities (50-85%) |
| What test determines future management of PUL? | -hCG (but clinical symptoms better give better indication of future managment) |
| When would expectant managment for ectopic pregnancy be apropriate? | If minimal symptoms, stable patient, painfree and falling hCG |
| When is medical management for ectopic pregnancy first line treatment? | -women can return for follow up -no significant pain -unruptured ectopic with adnexal mass <35mm -no visible heart beat -Serum hCG <1500 -USS confirming no intrauterine pregnancyIs first line for women who can return for follow up) |
| When is surgery first line management for women with ectopic pregnancy? | Is first line if woman is unable to return for follow up after methotrexate or if symptoms/signs of: -significant pain -adnexal mass >35mm -fetal heartbeat on USS -serum hCG of >5000 |
| What is surgical treatment for ectopic pregnancy? | Salpingectomy- removal of fallopian tubes |
| What is offered to rhesus negative women following removal of ectopic? | Anti-D |
| If a woman is less than 6 weeks pregnant and is bleeding but not in pain- how manage her ectopcic? | Expectant management: -repeat pregnancy test 7-10 days later and return if test is positive or if symptoms get worse (then need to refer to EPAC) |
| What is the rate of reoccurance of ectopic pregnancy? | 18.5% |
| What percentage of women expperience bleeding in ealry pregnancy? | 30% |
| How to diagnose and manage a misscarriage? | 1) transvaginal USS to assess location and viability of pregnancy 2) if location not found- repeat scan, measure hCG, laparoscopy 3) if viability not established- repeat scan in 7 days |
| From how many weeks can we see a viable fetus? | 5.5 weeks transvaginally |
| How does bHCG change within a viable pregnancy and with miscarriage? | -viable pregnancy- doubling time is 2 days -complete miscarriage- 1-2 days |
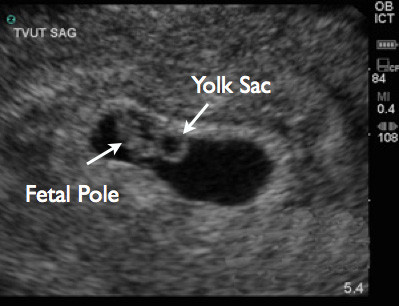
| What is the fetal pole? | thickening of the margin of the yolk sac of a fetus during pregnancy. Should see if bHCG is 1500-2000 |
| Management of miscarriage? | 1) Expectant- first line approach lasts 7-14 days. 2) Medical uterine evacuation- vaginal or oral misoprostol used to stimulate uterine expulsion. 3) Surgical treatment- manual vacuum aspiration under local or general |
| What 'suggests' a complete miscarrigae? | If bleeding and pain settle. Woman will be advised to take a urine pregnancy test after 3 weeks to confirm. |
| What 'suggests' an incomplete miscarriage? | If bleeding and pain persist or increasing |
| What suggests a 'missed' misscarriage? | Is a 'silent' miscarriage and no bleeding or pain |
| How much misoprosol used if missed miscarriage or incomplete? | 1) missed miscarriage- 800ug oral/vaginally 2) incomplete miscarriage- 600ug oral/vaginally. --> bleeding should start 24 hours after treatment *also offer pain relief and anti-emetics* *must repeat preganacy test 3 weeks post to confirm Tx has worked* |
| What is Gestational Trophoblastic disease? | A group of conditions in which there is abnormal proliferation of gestational trophoblast tissue. |
| Examples of Pre-Malignant Gestational trophoblastic disease? | 1) Partial Molar pregnancy 2) Complete molar pregnancy |
| Examples of Malignant gestational trophoblast disease? | 1) Invasive mole 2) Choriocarcinoma 3) Placental site trophoblastic tumours |
| How common is a molar pregnancy? | 1 in 1000 live births |
| Presentation of a Molar pregnanacy? | -Vaginal bleeding -Excessive Nausea and Vomitting (Hypermesis Gravidarum) -Uterus is large for dates -hyperthyroidism? |
| What is the risk that may follow complete molar pregnancy? | 10% of complete molar pregnancies will go on to develop invasive disease! |
| If women continue bleeding after pregnancy- what must we always consider? | Choriocarcinoma! Give methotrexate to treat and monitor bHCG fir 6 months- 2 years |
| Genetics of partial and incomplete molar pregnancies? | Complete mole: 2 sets of paternal genes, and no maternal genes. Partial mole: 3 sets of genes, 1 maternal and 2 paternal. |
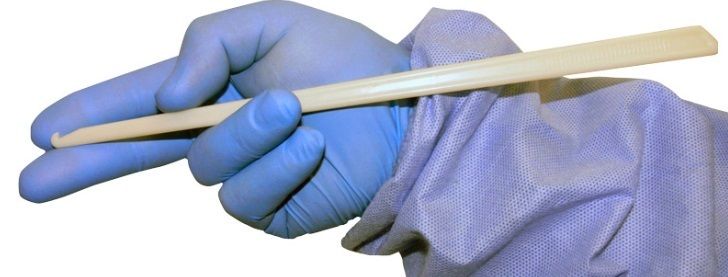
| What is this and used for? Risks? | Amnihook- used for amniotomy for inducton of labour. Risks- cord prolapse if lying between babies head and cervix. Can cause fetal asphyxia if untreated. |
| How to treat cord prolapse? | Decompress the cord by elevating the fetal head manually or by putting the mother in a prone knee-chest position or by filling the maternal bladder with saline. -Emergency C-section may be needed. |
| When use membrane sweep? Evidence for use? | Offered at 40-41 weeks in nullips and 41 weeks in multips. 8 women are membrane swepts to prevent one formal induction. (NNT- 7) |
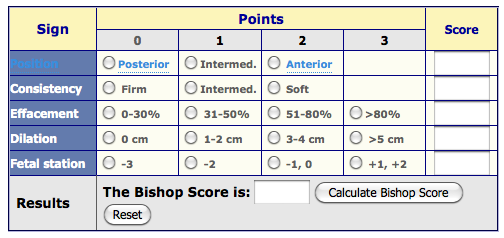
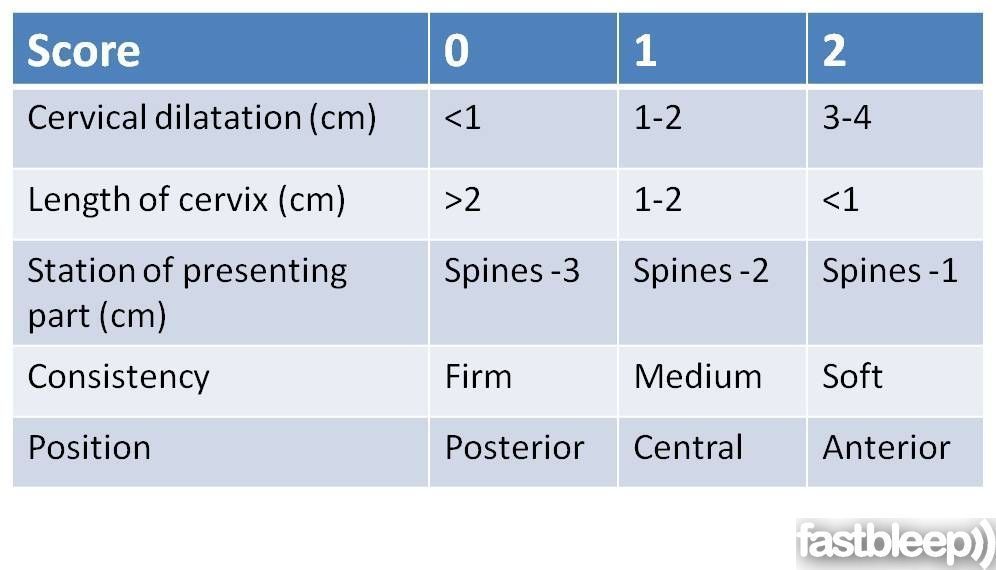
| What determines a 'favourable' induction? | A bishops score of >5. |
| Contraindications for inductions of labour? | -Breach -Fetal distress -placenta previa -vasa previa -cervical fibroid |
| What is Vasa Previa? | Where fetal BV run across or through uterus opening- and these BV could rupture when when the supporting membranes rupture. |
| What is determines an 'unfavourable' induction? | Bishops score <3. |
| What % of labours are induced? | 20% |
| Indications for induction of labour? | -Post-dates (>42) -IUGR -Pre-Eclampsia -diabetes -previous stillbirth -pre-labour prolonged rupture of membranes -twins |
| Risks of induction of labour? | -prolonged labour duration -more likely to require regional anaesthesia- as sudden, V painful contraction- and therefore more likely to require instrumental delivery -Uterine hyperstimulation -Uterine rupture -Umbilical cord prolapse -Failed induction- LSCS |
| What is Bishop's score system based on? | >8- woman likely to go into labour & cam break waters easily. |
| Methods of induction of labour? | 1) Prostaglandins (Pessary/propress= 24 hour tampon) or Gel= applied locally 4 hours, and can repeat 4 horus later) which ripens the cervix to enable amniotomy 2) Amniotomy- artificial rupture of membranes 3) Syntocinion (oxytocin) infusion 4) Mechanical cervical dilators |
| What is risk of inducing labour in a woman with a previous C-section? | Increased risk of uterine rupture (1 in 100 if induced, or 1 in 200 if spontaneous labour anayway) |
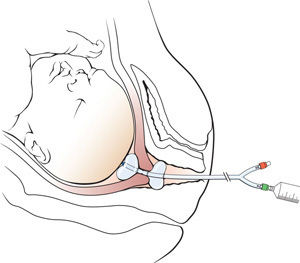
| What is this method called and what for? | Cook cervical ripening balloon which is used to mechanically dilate the cervix |
| What is 'Naegeles rule'? | A rule to work out EDD= LMP- 3 months + 7 days |
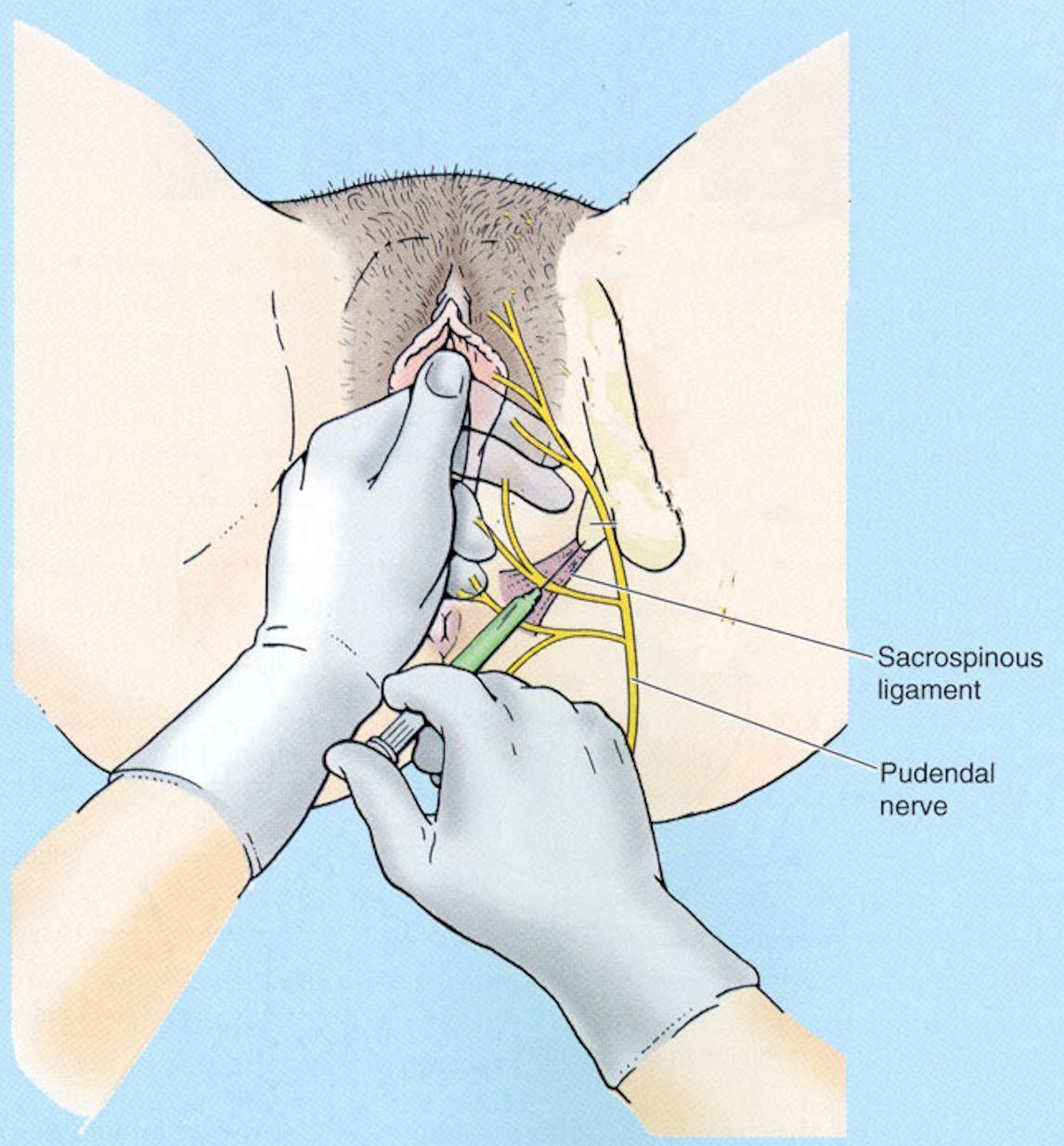
| What anagesia should be used in Labour? | non-pharmacological: -Hypnotherapy/relaxation -Aromatherapy -Tens- transcutaneous electrical nerve stimulation -water Pharmacological: -paracetamol, codiene, diamorph, pethidine (short term effects on neonate if delivered within 2 hours of taking) -Epidural -Entonox- gas and air (nitric oxide) -Transpudendral nerve block |
| What % of pathological CTGs mean that fetus is compromised? | 50% of pathological CTGS mean that fetus is in danger and needs urgent delivery |
| What is a better marker of fetal wellbeing if CTG is pathological? | Fetal blood sampling- take blood from fetus scalp -PH>7.25 then need repeating in 1 hour if CTG the same -PH 7.2-7.25 then repeat in 30 mins -PH <7.20 then fetus is risk of hypoxia and needs delivery |
| What is the Harmony test? | Measures free fetal DNA from mothers blood (blood taken from vein in mothers arm) and gives a strong indication if fetus is high or low risk of having a triosomy 21 (downs), 18 (edwards) or 13 (patau syndrome) |
| How births are Trisomy 21? | 1 in 700 births (risk increases with maternal age) |
| What further tests used if high chance of trisomy from Harmony test? | 1) Chorionic villus sampling- small sample of cells taken from the placenta either transabdominally or transcervically and checks if chromosomal abnormailities. Usually perfromed between 11-14 weeks 2) Amniocentesis- small sample of amniotic fluid taken. Carried out between 15-18 weeks of pregnancy. |
| What medication is given to women as first line treatment for moderate to severe HTN (pre-eclampsia) in pregnancy? | oral labetalol |
| If birth is considered likely within 7 days in women with pre-eclampsia, and woman is 24-34 weeks pregnant- what give? | Give two doses of betamethasone* 12 mg intramuscularly 24 hours apart in women between 24 and 34 weeks |
| What is the name of the validated questionnaire to assess the severity of nausea and vomiting in pregnancy? | Pregnancy-Unique Quantification of Emesis [PUQE] score |
| If moderate to high risk pre-eclampsia- what is recommended that women take? | 75mg/day of aspirin from 12 weeks onwards to reduce risk of blood clots |
| Common symptoms of obstetric cholestasis? | -Itching on palms and sole of feet |
| What surgical approach is used with severely overweight women for C-sections? | supra-panus |
| Risk factors for pre-eclampsia? | |
| From what gestation can a fetus heart beat be heard? | 6 weeks |
| From what date is a pregnancy counted from? | From the first date of last period |
| What steps should be used by scanner in EPAC to determine a viable pregnancy? | 1) Look for fetal heartbeat 2) (If not) then look for fetal pole, and if (identiy then measure crown-rump length (7mm cut off) 3) (if not) then measure mean gestational sac diameter (25mm cut off) |
| What is deemed 'early pregnancy'? | 13 weeks |
| what is Expectant management? | A management approach in which treatment is not administered, with the aim of seeing whether the condition will resolve naturally. |
| What must be offered to women who attend EPAC? | A transvaginal ultrasound scan to identify the location of the pregnancy and whether there is a fetal pole and heartbeat |
| What management should be offered as first line for a woman with confirmed diagnosis of miscarriage? (when not?) | Use expectant management for 7–14 days, but NOT when: 1) woman at increased risk of haemorrhage (e.g- she is in the late first trimester) 2) previous adverse and/or traumatic experience associated with pregnancy (for example, stillbirth, miscarriage or antepartum haemorrhage) 3) At increased risk from the effects of haemorrhage (for example, if she has coagulopathies or is unable to have a blood transfusion) 4) there is evidence of infection. |
| surgical management of miscarriage offered? | 1) LOCAL anaesthetic manual vacuum aspiration in OP or clinic 2) surgical management in a theatre under general anaesthetic. |
| When to refer to EPAC? | Woman with bleeding and other symptoms of early pregnancy complications (pain) |
| If a pregnancy is <6 weeks, and woman bleeding but not in pain, what do? | Advise to: - repeat a urine pregnancy test after 7–10 days and to return if it is positive. (If negative then misscarriage) |
| What factors may mean that a women in EPAC requires a transabdominal scan rather than a transvaginal? | -woman has enlarged uterus -fibroids -ovarian cysts *but there is limitation to transabdo scans* |
| If crown-rump length of fetus is <7mm with trasnvaginal USS scan, and no visible heart beat- what do? | -need to perform a second scan minimum of 7 days later to confirm miscarriage diagnosis |
| For a woman with an increase in serum hCG concentration greater than 63% after 48 hour- what is likely? | -inatruterine pregnancy is likely as HCG doubles every 48 hours in a viable pregnancy |
| Degree classification of tears in labour? | SULTAN CLASSIFICATION 1st degree- injury to perineal skin and/or vaginal mucosa 2nd degree- injury to perineum involving perineal muscles but not involving sphincters 3rd degree- injury to perineum involving sphincter.... 3a- <50% external anal sphincter torn 3b- >50% external anal sphincter torn 3c- internal anal sphincter torn 4th degree- injury to perineum involing sphincter complex and anorectal mucosa |
| What type of episitomy be considered with instrumentla delivery? | Medio-lateral episiotomy (cut 60 degrees away from perineum) |
| What cell type lines the proximal anal canal? | rectal mucosa (columnar epithelium) |
| What cell type lines distal anal canal? | modified squamous epithelium |
| Which techniques should be used to accomplish the repair of the anorectal mucosa? | sutures using either the continuous or interrupted technique |
| techniques should be used to accomplish the repair of the internal anal sphincter? | Interrupted or mattress sutures without any attempt to overlap the IAS |
| Which techniques should be used to repair the external anal sphincter? | overlapping or an end-toend (approximation) method |
| Prognosis following an anal repair? | Women should be advised that 60–80% of women are asymptomatic 12 months following delivery and EAS repair. |
| Incidence of twins in UK? | 1 in 65 births in UK are twins |
| Most common type of twin? | DCDA (Dichorionic Diamniotic)- usually dizygotic from 2 eggs and 2 sperm and often due to IVF |
| What do monochorionic twins mean? | one fertilsed egg that then divides to form identical twins. Can be diamniotic so babies in 2 seperate sacs or monoamniotic where babies in 1 sac. |
| What is twin-twin transfusion syndrome and what related to? | Often caused by twins sharing a placenta (monochorionic twins). It is where there is abnormal vessels through the shared placenta which mean that blood flows mainly from one baby (donor) which becomes malnourished, to another baby which can develop heart failure. |
| How treat twin-twin transfusion syndrome? | Detect early and treat: laser ablation of connecting vessels in utero |
| What type of twin is most likely to be still birth? | MCMA |
| Incidence of conjoined twins worldwide? | 1 in 90,000 |
| Most rare form of twins? Risk? | MCMA: High risk of cord entanglement |
| Risks of multiple pregnancies? | 1) Anaemia 2) Congenitial- more likely to have false positive from downs screening & more likely ot suffer complications from amniocentesis 3) Pre-term labour 4) HTN and pre-eclampsia- 2-3 times more likely to suffer. need to take aspirin daily, and BP/urinalysis taken at every scan. 5) Fetal Growth restrction |
| What % of twins are born pre-term? | 50% born pre-term 10% born <32 weeks |
| Delivery planning for different types of twins? | DCDA elective delivery- 37-38 weeks MCDA elective delivery- 36-37 weeks MCMA elective delivery by C-section at 32 weeks |
| Circumstances which would enable a normal vaginal delivery for twins? | If twin 1 is cephallic and there is an uncomplicated twin pregnancy (DCDA or MCDA) then vaginal birth should be offered. **There is an increased risk of morbidity for twin 2 at delivery, and increased risk of C-section even after successful 1st vaginal birth** |
| What would be offered if first twin is not cephallic? | Elective C-Section should be offered and administration of corticosteriods to help prevent respiratory distress |
| When routine growth scans for differing twins? | DCDA twins- every 4 weeks from 24 weeks MCDA- every 2 weeks from 16 weeks *must always annoate twins on scans to ensure monittoring growth correctly** |
| How manage anaemia of mother if twins? | FBC on booking, 20, 28, 34 weeks and treat if >115 with feroud sulphate 200mg orally bd. |
| How best to screen for chromosomal abnormailites if twins, and at what gestation? | 11-13 + 6 days- mucal translucency anomaly scan- 18-20 weeks |
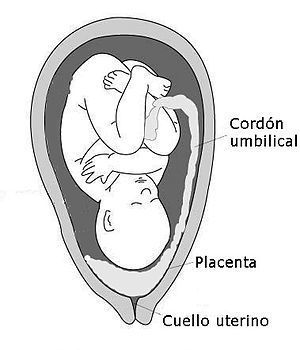
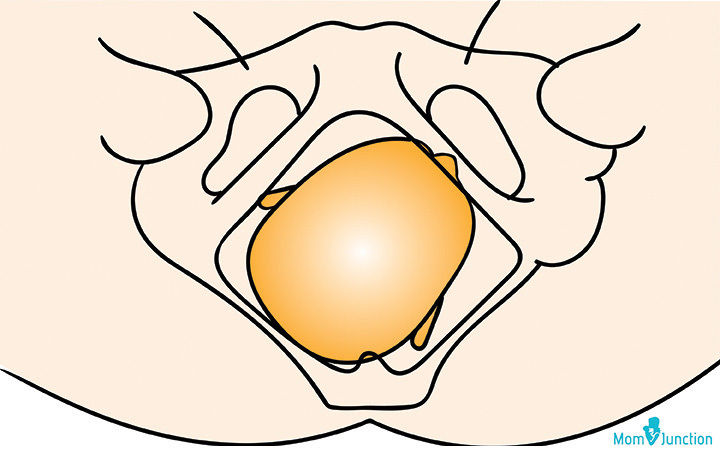
| What is this conditon? Incidence? | Total placenta previa- where the placenta cover the os and is graded by how close/how much it covers the Os -10% risk at 20 weeks, 1% risk at term *avoid PV exams and sex* |
| What is this? | Low lying placenta |
| RF for placenta Praevia? | -Previous Termination of pregnancy -Previous Praevia -Increased maternal age -Multi-parity -Previous LSCS -deficient endometrium (uterine scar, endometriopsis, fibroids) -Multiple pregnancies -Smoking |
| Significance of vasa previa? | Fetal blood (cord) vessels run through the membranes covering the cervix. These vessels can rupture which can cause massive heamorrhage and baby can die. |
| Classic presentation of Vas previa? | painless vaginal bleeding, rupture of membranes, and fetal bradycardia |
| How diagnose vasa previa? | Transvaginal ultrasonography *Differential is 'funic presenation' where on US the cord moves away |
| statistics of placental abruption? | -70% happen in low risk pregnancies |
| RF for placental abruption? | -previous placental abruption -blunt trauma -early pregnancy bleeding -Pre-eclampsia -Fetal Growth restriction -malpresentation -polyhydraminos -increased maternal age >35 -low BMI -IVF -Infection -premature rupture of membranes -smoking -drug misuse- *cocaine causes VC and increase in BP) -maternal thrombolphilia |
| A theory for why placenta previa happens? | Upper endometrium may not be well vascularised due to damage to this area. therefore the placenta implants in lower uterus. Damage may be from: -previous C-section -abortion -uterine surgery -multiparity |
| Types of placenta previa? | 1) complete- placenta completely covers cervical Os 2) Partial- placenta partially covers cervical os 3) Marginal- placanta egde extends to within 2cm of cervical os |
| When does placenta previa generally cause bleeding? | from 20 weeks, when the lower uterine segment begins to grow and stretches the placenta |
| What condition is placenta previa related to? | Placenta Accreta- where the placenta grows into the myometrium wall |
| What does placenta previa increase the risk of? | -fetal hypoxia -pre-term delivery -ante-partum haemorrhage |
| What is happening physiologically in a placental abruption? | There is a seperation between the uterine wall and the decidua basalis due to degeneration of the uterine arteries that supply blood to placenta (due to smoking/HTN) |
| Types of placental abruption? | 1) partial 2) complete **can be concealed (hidden pocket of blood behind the baby) or apparent (see vaginal bleeding) |
| Maternal complications of placental abruption? | -Hypovolaemic shock -Sheehan's syndrome (perinatal pituitary necrosis) -renal failure -DIC- decidualis basilis is rich in thrombolplastin which causes widespread clotthing |
| Fetal complications of placental abruption? | -hypoxia and asphyxia -premature birth |
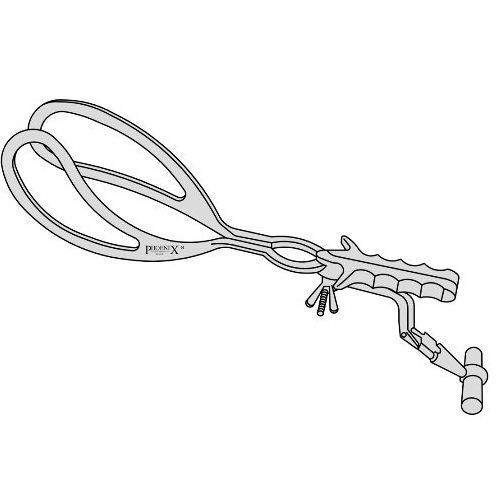
| Types of forcep? Uses? | Wrigley's (smaller and shorter) - used in C-section -used when babys head is very low and visible |
| What is a Neville Barnes forcep used for? | If the baby’s had was looking down at the floor (direct OA – occipito-anterior position) or looking straight up (direct OP – occipito-posterior position) and the obstetrician does not want to rotate the baby’s head, and the baby is in mid/low cavity |
| When is Kiellands forceps used? | ROTATES BABY- if the baby’s head is not a direct OA or OP. |
| What is most common forcep that is used? | Neville Barnes forcep |
| Advantages of forceps? | -faster than ventouse -less cephalohaematoma -less retinal haemorrhage -can be used for face/breech -can be used if <34 weeks -less likely to fail |
| Risks of forceps? | More maternal risk of tearing or lacerations and needing an episiotomy |
| Pain relief for an instrumental delivery? | Pudendral nerve block (if head not past ischial spine already) |
| Fetal complications with instrumental delivery? | -bruising -skin abrasions -facial nerve palsy -cephaloheamatoma -retinal haemorrhage -intracranial haemorrhage -skull fracture |
| What is this? | Kiwi Omnicup ventouse |
| What is this used for? |
Metal ventouse cup used if the baby is in the occipital posterior position and so head is up and need to get a ventouse on back on head to pull baby out
Image:
Images (binary/octet-stream)
|
| Where is a ventouse cup ideally placed? | Places anterior to the posterior fontanelle |
| What must be done/given to patient before ventouse used? | 1) Local anasthetic into perineum 2) Bladder catheterised |
| Most common reasons for a delay in 2nd stage of labour? | [POWER, PASSAGE, PASSENGER] 1) Insufficient maternal effort: due to exhaustion or because of an epidural 2) Malposition: baby may be in such a way that it physically cannot be pushed out e.g- OT or OP 3) Malpresentation- Brow/Face (1 in 1000) |
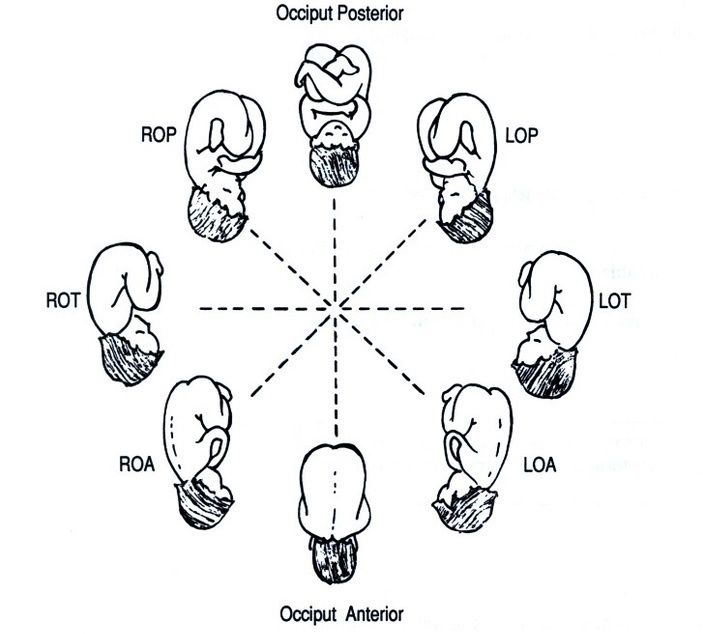
| What is OP and can a baby be delivered in this positon? | Occipital-Posterior- where the back of the babies head is towards bum and the babys face is to pubes. Babies in this postion can be delivered however the pelvis needs to be larger than normal or the baby needs to be smaller than normal. |
| Right Occipital-posterior | |
| Main fetal positions? | 1) Occipital-anterior (ideal)- face down back up 2) Occipital-transverse 3) Occipital-posterior- face to pubes |
| What is deemed a normal length of time for second stage of labour in a nulliparous and multiparous woman? | Nulliparious- within 3 hours. If >2 hours then diagnosed as 'delay' Multiparous- within 2 hours. If >1 hour then deemed delay. |
| Normal length of active labour in a nulliparous woman? | 1st stage (dilating)- average 8 hours. Can be up to 18 hours but is unlikely. 2nd stage (pushing)- up to 3 hours active |
| Normal length of active labour in a multiparous woman? | 1st stage- 5 hours often. no more than 12 hours. 2nd stage- 2 hours (considered delay if >1) |
| What assessing when doing a vaginal examination in labour? (5) | 1) Dilatation 2) Position of cervix 3) Effacement of cervix- length 4) Fetal position 5) Fetal station- station 0 is when the head is at the ishial spines and is narrowest part of pelvis |
| When a baby is occipital-anterior- how large is the smallest diameter of the head to fit through the pelvic outlet? | The suboccipitobregmatic diameteris 9.5cm which is the smallest diameter to fit through the pelvic outlet. It is the diameter of the fetal head from the lowest posterior point of the occipital bone to the center of the anterior fontanelle. |
| When a baby is occipital posterior- what is the smallest diameter in which a head can fit through the pelvic outlet? | 11cm! -reason why we like babies to be OA. |
| If a baby is presenting as 'brow' how big is the diameter of head to get through pelvis outlet? | 13cm- won't get through |
| Advantages of ventouse over forceps? | -Less analgesia -Less perineal trauma -Less vaginal trauma -Less post delivery pain -less force needed |
| Criteria for instrumental delivery? | -consent -anagesia -cervix needs to be fully dilated -head not palpable abdominally and below spines vaginally -know presentation/positon -bladder empty |
| Where is ventouse applied onto head? | 'Maximum fliction point'- 1.5cm anterior from posterior fontanelle |
| At what rate does cervix dilate during active labour? | 1cm per hour |
| C-section risks? | -Bleeding -Infection -Damage to pelvic viscera -Fetal laceration in 1% -DVT/Thromboembolism |
| Mneumonic to looking at CTGs? | DRCBRAVDO DR- determine risk C- contractions BR- baseline rate A- accelerations V- variability- time between babies heart beats D- decelerations O- overal assessment |
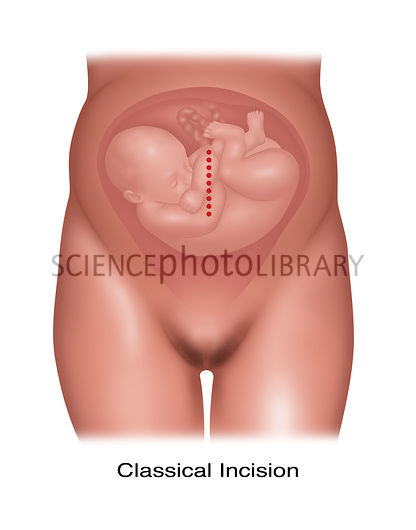
| What is a classical C-section? When used? | -Vertical incision on uterus, with either a transverse or vertical skin incision *Rarely used, but when is due to: premature fetus, structural abnormality making lower segment not useful/formed* |
| Risks of classical C-section? | adhesions more likely, infection, and CI to have VD following |
| Categories of CS? What means? | Determines the timing of the C-section Cap1- Crash- immediate threat to life of woman or fetus and baby needs to be delivered in 30 mins (fetal brady, placent abruption) Cap2- maternal or fetal compromise- 30-60mins (failure to progress) Cap3- 'semi-elective'- (pre-eclampsia, failed induction of labour) Cap4- elective. |
| When should elective C-sections be carried out? | Always after 39 weeks- as risk of TTN (transient tachypnoea of newborn) **if before 39 weeks then corticosteriods need to be givenfor fetal lung development** |
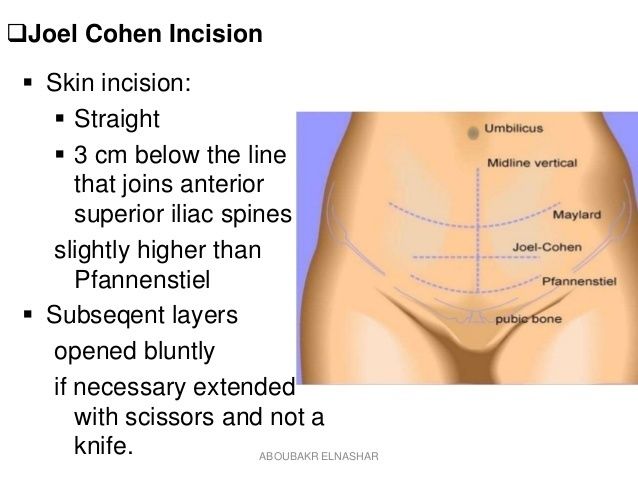
| What is most common C-section? | Lower caesarean C-section- 'Cohen' straight incision 3cm above symphysis pubis. If transverse then reduced adhesion formation, less blood loss, lower risk of scar de-hiscence (uterine rupture) |
| Why can caffeine be used in pre-term infants? | Used as a respiratory stimulant to prevent apnoeas of prematurity (>20secs of no breathing with desats and brady) and faciliate etubation. |
| Is use of caffieine safe? | (yes) -It has a long half-life (>100 hrs)- so can be given once daily safely and has less toxicity -It has a wide therapeutic to toxic ratio (risks) -tachycardia, agitation, tachpnoea, tremors, vomitting, worsens reflux |
| What dopplers can be used in addition to umbilical artery dopplers? | Middle cerebral artery dopplers. They can be used to determine ratio of placental flow to MCA perfusion. |
| Why do we worry if there is meconium stained liquor? | As there is a risk that baby will inhale the meconium and and cause 'meconium aspiration syndrome' |
| Risk factors for babies to release meconium in-utero? | -Increasing gestational age -fetal hypoxia |
| What are the risk that meconium aspiration? | Meconium is a lung irritant and can result in both mechanical obstruction as well as chemical pneumonitis and predisposes to infection |
| Intrapartum care if meconium stained liquor? | 1) There should be continuous electronic fetal monitrroing 2) If signs of fetal distress (brady, decelerations)- then need fetal blood sample and if ph <7.21 then emergency delivery needed 3) No suction prior to delivery |
| What is a cervical stitch (cervical cerclage) for and when put it? | -Is a stitch in neck of uterus to prevent a woman going into pre-term labour -Normally put in between 12 and 24 weeks of pregnancy and then removed at 36–37 weeks unless you go into labour before this. |
| What length cervix determines if a woman needs a cervical stitch or not? | -if less than 25mm |
| What procedure can be done to try and turn a breech baby? | External cephalic version (ECV) |
| What pain relief medication is given to women post C-section? | Diclofenac in the bum |
| What medication is given to all women having a C-section? | -Ranitidine- prevents acid in stomach -Prophalytic antibiotics |
| How does cell salvage work? | Patients blood is suctioned and then is present in a container with heparin and saline- to then be processed before going back into womans body. ***Useful if woman is a Jehovahs witness*** |
| Define Pre-Eclampsia | New HTN presenting after 20 weeks gestation with significant proteinuria |
| Define Eclampsia... | Convulsive conditon associated with pre-eclampsia |
| Define gestational hypertension... | New HTN presenting after 20 weeks gestation without significant proteinuria |
| What is chronic hypertension as related to pregnancy? | HTN that is present before before 20 weeks of pregnancy OR if hypertensive medication is required prior to pregnancy |
| Define HTN... | Persistently raised BP (>140/90) |
| Define severities of HTN in pregnancy (mild, moderate and severe)? | 1) Mild hypertension= 140/90- 149/99 mmHg 2) Moderate hypertension=150/100 to 159/109 mmHg 3) Severe hypertension= 160/110 mmHg or higher |
| What is HELLP syndrome? | Haemolysis with elevated liver enzymes and low platelet count |
| Symptoms of pre-eclampsia? | 1) severe headache 2) visual issues- 3) blurring/flashing/photophobia 4) Epigastric pain (liver) 5) Nausea/ vomitting 6) Odema (hands, feet, face |
| What % of pregnancies worldwide are complicated by HTN disorders? | 5-10% |
| How many women with severe pre-eclampsia/eclampsia need admission to ITU? | 1 in 20 women |
| Risk factors that make a woman at risk for developing pre-eclampsia? | 1) Chronic HTN or HTN during previous pregnancy 2) Diabetes 3) Chronic kidney disease 4) Autoimmune disease (lupus, anti-phospholipid) 5) First pregnancy 6) >40 yrs old 7) pregnancy interval >10 years 8) BMI >35 9) FMHX of pre-eclampsia 10) Multiple pregnancies |
| How to manage development of pre-eclampsia for a woman with risk factors? | 75mg of aspirin daily from 12 weeks until birth of baby |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.