21022017
Description
Flashcards by Raziel Rosas, updated more than 1 year ago
|
|
Created by Raziel Rosas
about 4 years ago
|
|
| Question | Answer |
| Ruling out coronary artery disease in primary care | *age/ sex: female >65 male >55 *know clinical vascular disease *pain worse during exercise *pain not reproducible by palpitation * patient assumes pain is of cardiac origin (Positive if 3-5pts, sen 87% spe 80%) Variations: In elderly women dizziness, back pain, lightheaded ness or weakness/ in diabetics dyspnea, syncope and fatigue |
| Mayor risk factors for CAD | *mayor: smoking, diabetes, HTN, hyperlipidemia, family history of CAD in 1st Degree relative male<55 female<65, untreated obstructive sleep apnea, chronic kidney disease |
| Minor risk factors for CAD | Obesity, sedentary lifestyle and age |
| Red flags for CAD | Severe pain, pain for >20min, new onset of pain at rest, severe SOB, loss of consciousness, hypotension, tachycardia, bradycardia, cyanosis |
| Must watch when prescribing salbutamol | Hypokalemia signs: lethargy, irritability, paresthesia, myalgia, weakness, palpitations, N/V, polyuria |
| Indications for BPH surgery | Absolute: renal failure with obstructive uropathy and refractory urinary retention Relative: recurrent UTI, hematuria refractory to medical treatment, renal insufficiency, bladder stones. |
| Signs of poorly controlled asthma | *B agonist use >4 times in a week * asthma related abscess from work/school *exercise induced asthma * night time symptoms >1 week * signs of adequate control: FEV 1 peak expiratory flow >90% of personal best with diurnal variation <10-15% |
| Complications of COPD | Polycythemia 2d to hypoxemia, chronic hypoxemia, pulmonary HTN from vasoconstriction, COR pulmonale, pneumothorax due to rupture of emphysema bullae, depression, bacterial infections |
| Antimicrobial management in acute otitis media ( s.pneumoniae, H influenzas, M. Catarrhalis, Group A strep, S. Aureus | .- Children’s< 6mo, 6-24 mo 48-72 hrs follow-up, >24mo, treat if worsen after 48-72hrs, 10d if course if <24mo, 5d if >24mo 1- Amoxicillin 80mg/kg/d p.o. C/12hrs (max 3gr/d = 37.5kg) +adults 500mg p.o. C/8hrsx7-10d 2.- Amo/ ac.clavulanate 40-80mg/kg/d p.o. C/12hrs or cefprozil 30mg/kg/d p.o. C/12hrs + adults 500-875mg p.o. C/12 x7-10d or cefprozil 250-500mg p.o. C/12 x 7-10d 3.- cefuroxime 30-40mg/kg/d p.o.c/12hrs or clarithromycin 15mg/kg/d p.o. *in TM perforation or ventilation tubes: ciprodex (cipro+dexa) 4drops c/6-12hrs x 5 days |
| Antimicrobial management in sinusitis ( S.pneumoniae, Hinfluenzae, M. Catarrhalis, S.aureus ) | 1.children: amoxicillin 80mg/kg/d p.o. X5-14d (max 3gr day = 37.5kg) +adults 500mg p.o.c/8hrs x 5-10d 2.-amo/clavulanate 40-80mg/kg/d or cefprozil 30mg/kg/d x10-14d +adults 500/850 mg p.o. C/8hrs x5-10d or cefuroxime 250-500mg p.o. C/12hrs x 5-10d 3.- cefuroxime 30-40mg/kg/d p,o. C/12hrs x10-14d or clarithromycin 15mg/kg/d p.o. C/12hrs x10-14d + adults levofloxacine 500mg p.o./d x 5-10d or same with moxifloxacin 400mg |
| Treatment for strep pharyngitis (group A B-hemolytic streptococcus) | Children: penicillin V or amoxicillin, 2. Erythromycin, 3. Cephalexin or cefprozil Adults: penicillin V, 2. Erythromycin, 3. Cephalexin or cefprozil |
| Most common causes of amenorrhea | Primary: 1. Müllerian agenesis, 2. Abnormal sex chromosomes (Turner syndrome) 3. Functional hypothalamic Secondary: functional hypothalamic |
| Wernickes encephalopathy (alcohol related) | Is a alcohol induce amnestic disorder due to thiamine deficiency, acute and reversible with ocullomotor dysfunction such as nystagmus (CN IVpalsy) gait ataxia and confusion. |
| Korsakoff’s syndrome (alcohol related) | Is a alcohol induced amnestic disorder due to thiamine deficiency, is chronic and only 20% reversible with treatment, anterograde amnesia and confabulation, cannot occur during an acute delirium or dementia and must persist beyond usual duration of intoxication with withdrawal |
| Low BMI associations | A low BMI is <18.5 Osteoporosis, eating disorders, under-nutrition, pregnancy complications. |
| Clinical definition of metabolic syndrome | Central obesity (men wc > 94cm women wc> 80cm) + any two of the following : TG >150mg/dL (1.7mmol) or HDL men <40mg/dL (1mmol/l) women <50mg/dL (1.3 mmol/l) or blood pressure >135/85 or fasting glucose >100mg/dL (5.6mmol/l) |
| Osteoporosis Canada recommendation for calcium and vitamin D daily requirements | Vit D: 800 -1000 UI/d in <50 years, 800 -2000 UI/d in >50years Calcium: 1000 mg/d from all sources for 19-50 years and pregnant/ lactating women and 1,200 mg/d for >50 years |
| Canadian cancer society recommendation for vitamin D use | In prevention of colorectal, breast and prostate cancer. 1000 UI/d during fall and winter, %all year who are older, dark skin, who don’t go outside often, and who wear clothing that covers most of their skin |
| Caloric intake for losing weight | Aim for caloric intake 500-1000 kcal/d less than total daily energy expenditure, (average 2000-2100 women, 2700-2900 men, roughly 35 kcal/kg/d) 3500 kcal energy expended / lb of fat burned result in 1-2 lb weight loss per week |
| Colorectal cancer screening in one second or third degree relative affected | Average screening begin at 50 years |
| Hyper triglyceridemia and pancreatitis | Serum triglycerides levels > 10mmol/l (885mg/dl) increase the risk of developing pancreatitis, even >5mmol/l (442mg/dL) |
| Colorectal cancer screening with polyps found at colonoscopy | 1-2 tubular adenomas <1cm =colonoscopy in 5years , >2 adenomas colonoscopy in 3 years, incomplete examination, numerous polyps, advanced adenomas, malignant or large sessile adenomas = colonoscopy after a short interval |
| Signs and symptoms of delirium tremendous (alcohol withdrawal delirium) | Autonomic hyperactivity (diaphoresis, tachycardia, increased respiration), hand tremor, insomnia, phychomotor agitation, anxiety, N/V, tonic-clonic seizures, visual/tactil/auditory hallucinations, persecutory delusions |
| When to suspect etiology from klebsiella | See red currant jelly sputum Think in the 3As. Aspiration pneumonia, alcoholics and diabetic, abscess in lungs. aspiration pneumonia’s more commonly manifest as infiltrates in the right middle or lower lobes due to the larger caliber and more vertical orientation of the right bronchus |
| Leading types of dementia | Alzheimers 40-50% mixed 20-25% levy body ( 5-15%), vascular 5-10%, frontotemporal 5-10% |
| Prevalence of depression in dementia | 20-60% , major depression decreases as dementia severity increases, vascular and mixed dementia have a higher prevalence |
| Dementia quick screen test | Mini cog (words immediate and delayed recall and clock hour ) + animal naming |
| Flags for differentiating most common causes of dementia | *Alzheimer’s disease: predominantly memory and learning issues * frontotemporal: language and behavior types * Lewy bodies: recurrent soft visual hallucinations, autonomic impairment, EPS, does not respond well to pharmacotherapy, fluctuating degree of cognitive impairment * vascular: vascular risk factors, focal neurological signs, abrupt unset, stepwise progression * normal pressure hydrocephalus: abnormal gait, early incontinence, rapidly progressive |
| 5 D of vertebrobasilar insufficiency | Drop attacks, diplopia, dysarthria, dizziness, dysphagia |
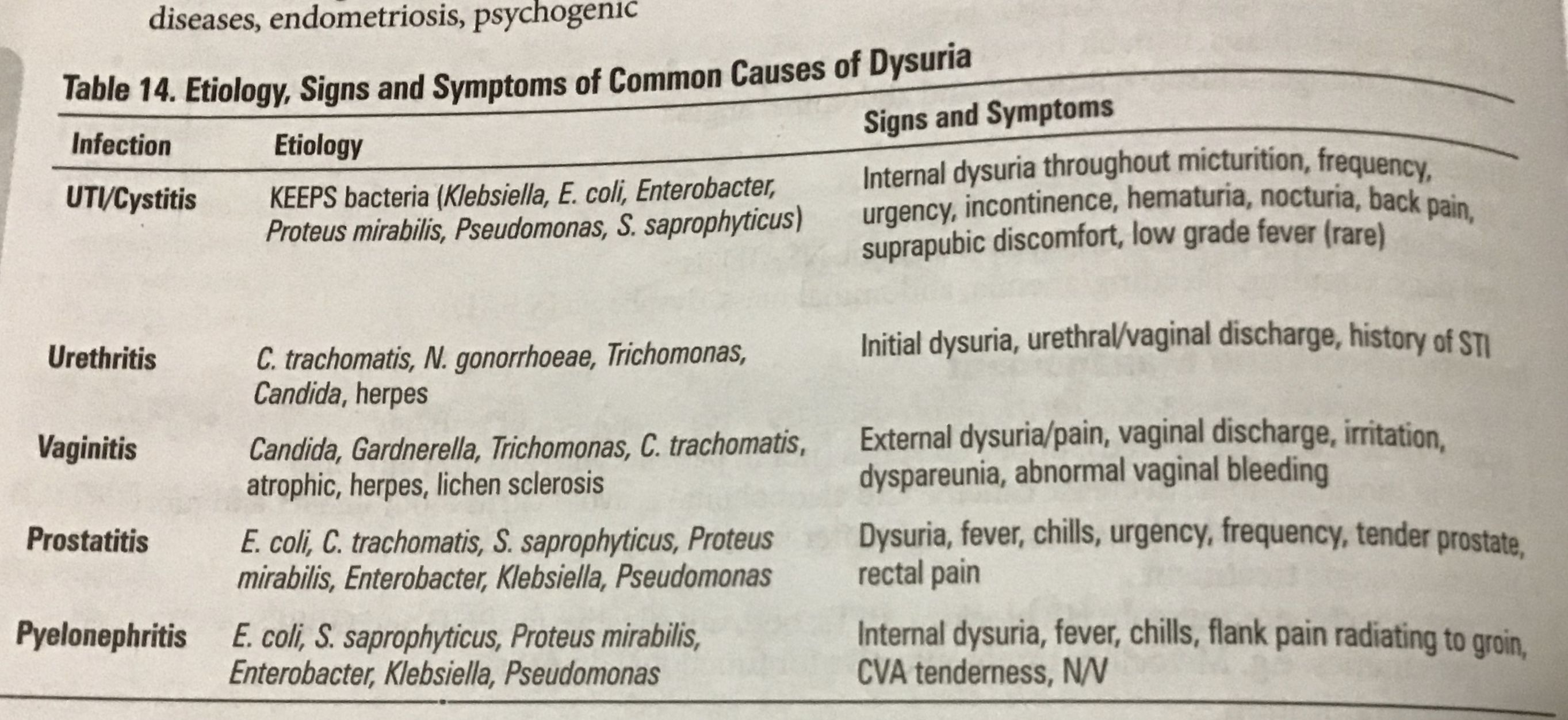
| Most common UTI/ cystitis bacterial etiology | KEEPS: klebsiella, e.coli, enterococcus, proteus, pseudomonas and s.saprophyticus |
| Signs and symptoms of common causes of dysuria | |
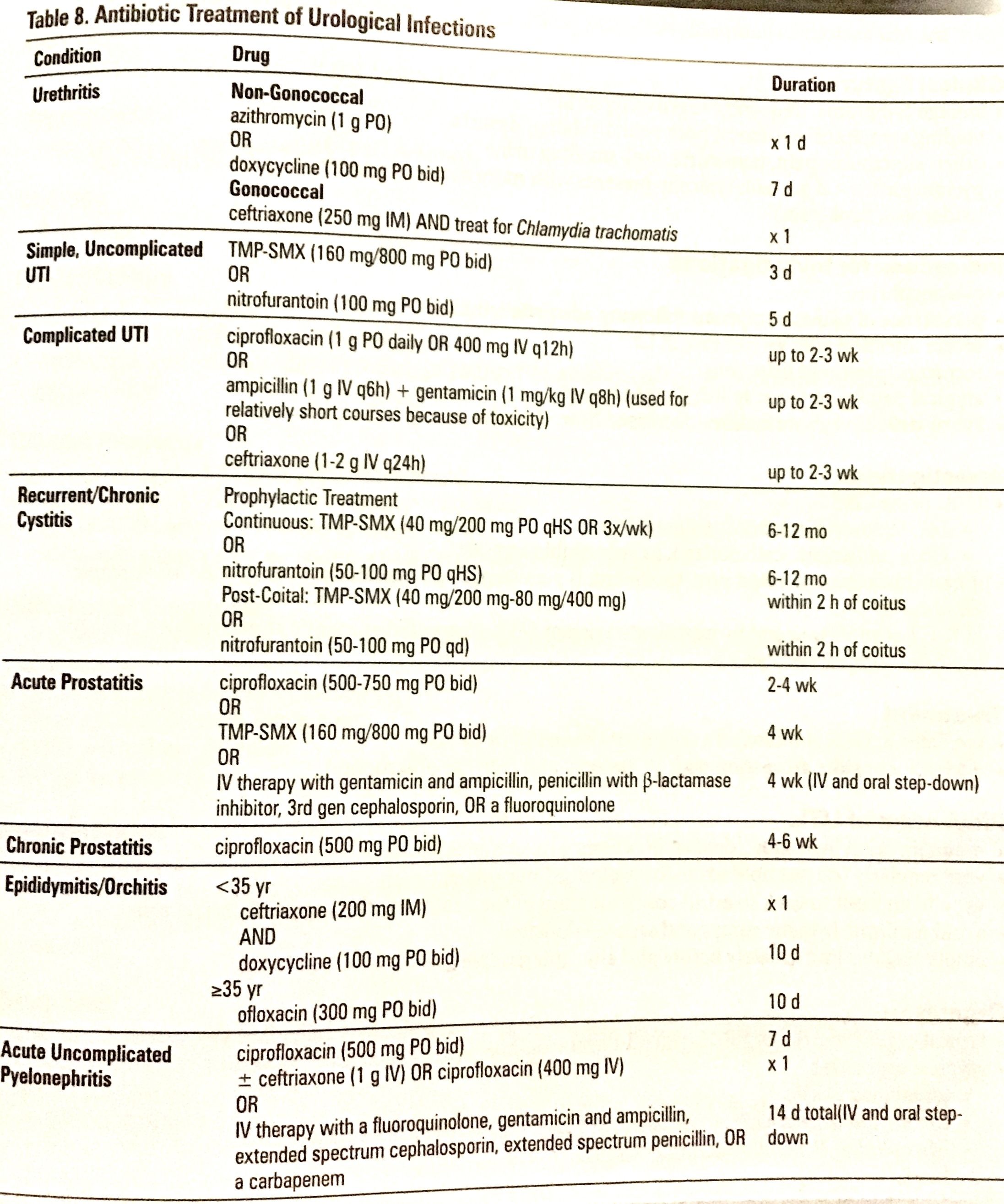
| Antibiotic treatment of urologic infections | |
| H.pylori eradication treatment | 1. PPI 1 tab 2x/day x 10 days 2. Amoxicillin 1g 1c/12 x 5 days (1-5 days) followed by 3. Clarithromycin 500 g 2x/day + 4. Metronidazole 500 mg 2x/day (day 6 to 10) |
| Most common etiology of epistaxis | #1Trauma: 90% of the nose bleeds occur in littles area witch contains the kiesselbachs plexus (anterior-inferior portion of the cartilaginous septum) * special causes: juvenile nasopharyngeal angiofibroma( most common benign tumor ) and trombocytopenic patients |
| First line Pharmacotherapy treatment for mayor depressive disorder (MDD) | 1.- ( SSRI) Sertraline 50-200mg (best in pregnancy and breast feeding) 2.- (SSRI) escitalopram 10-20mg ( the one with less drug interaction and are sleep awake neutral) 3.- (SNRI) venlafaxine 75-225mg useful for depression and anxiety disorder and neuropathic pain 4.- (NASSA) mirtazapine: 15-45 mg useful in depression with prominent features of insomnia, agitation or cachexia * physical improve at 2 wk and mood/cognition at 4wk |
| Management for depression | Acute phase 8-12 wk and 6-12 months maintenance after symptoms resolution. *for mild depression give a period of active support and monitoring Cbt or pit before initiating tx, * for moderate to sever pharmacologic + psychotherapy at least 6 months, * referral is recomended if there is no improvement after 6-8 wk / adolescent with moderate- severe depression and psychosis/ substance abuse |
| Common side effects of common medications in depression | SSRI ( paroxetine, fluoxetine, sertralin,escitalopram): sexual dysfunction, headache, GI, lost weight, tremors, insomnia, fatigue, elongated QT interval. SNRI (venlafaxine): insomnia, tachycardia,tremors, sweating. SDRI (bupropion): insomnia, nightmares, seizures, less sexual dysfunction than SSRI and are sinergic. TCA (amitriptyline) gain weight, and are lethal in overdose |
| Diagnostic criteria for DM | 1 if symptomatic 2 if not: FPG > 7.0mmol/ l HbA1c >6.5% 2hrs PG in a 75g OGTT > 11.1 mmol/L Random PG > 11.1 mmol/L |
| Genetic comparison between type 1 DM and type 2 | Type 1 is associated with HLA class 2 DRE 3 and DRE4 with either allele present in up to 95%. Type 2 have greater heritability, is polygenic and no HLA associated. |
| Most common auto antibodies (AB) In type 1 DM | Islet cell B AB Are present in 60-85% Of the patients and the most common is the GAD glutamic acid descarboxylase and 60%of patients also have anti insulin AB |
| Treatment with insulin in patients with type 1 and 2 DM | If initial HbA1c is 8.5% at dx you can initiate with metformin and insulin. Type 1: estimate total .5-.7 UI/Kg/Day 40% is basal at bed time and 20% as bolus in each meal. If premixed use 2/3 before breakfast and 1/3 before dinner. Type 2: estimate total 0.3-0.5 UI/kg/day (take as type 1) or adjust 10 UI until FPG 4-7 Adjust: <4 give 15mg carbohydrates and call MD, 4-8 same doses, 8+CF= 1UI, -8+2CF= 2UI - 8+3CF = 3UI (CF = 100/daily dose) |
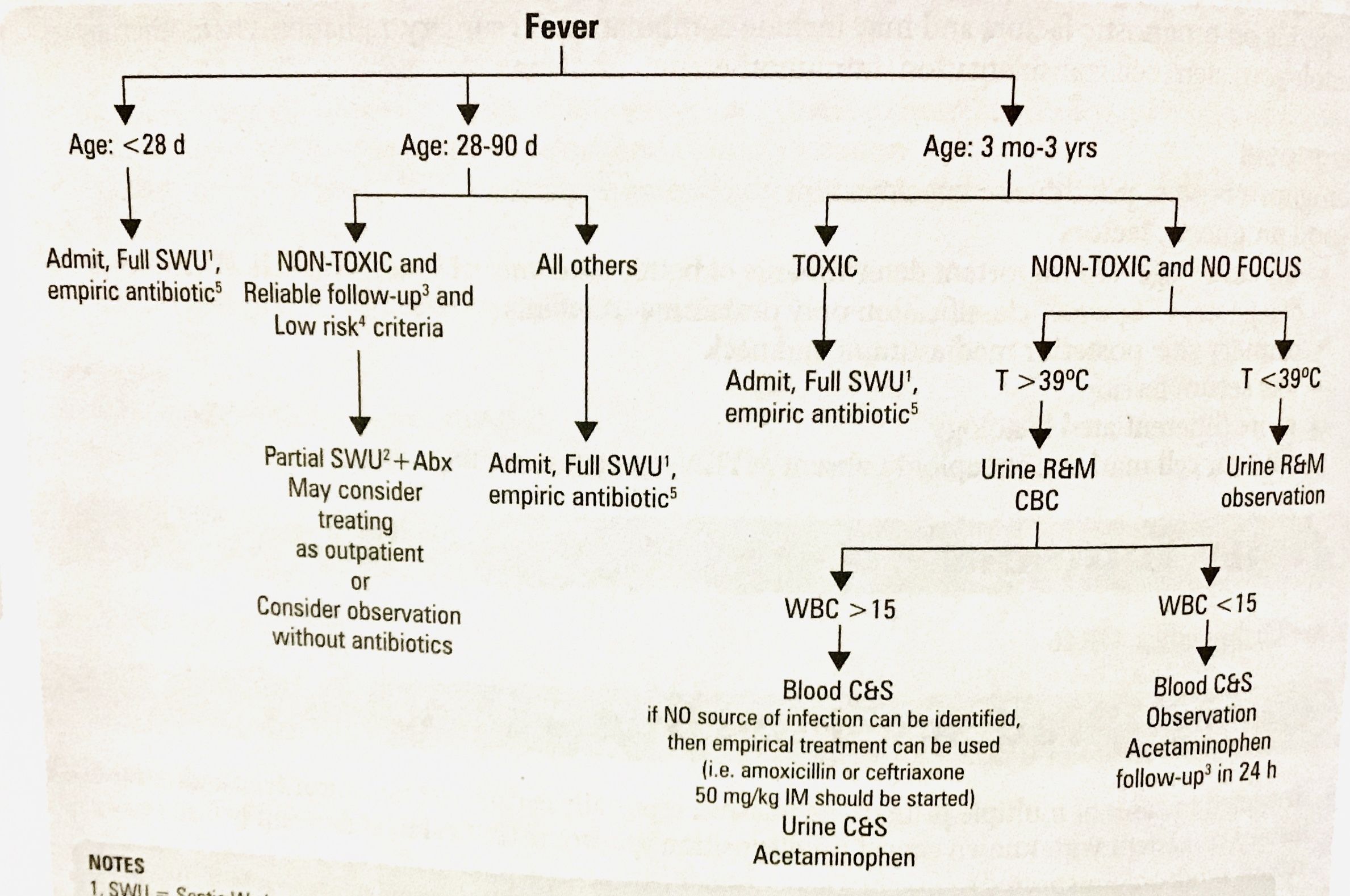
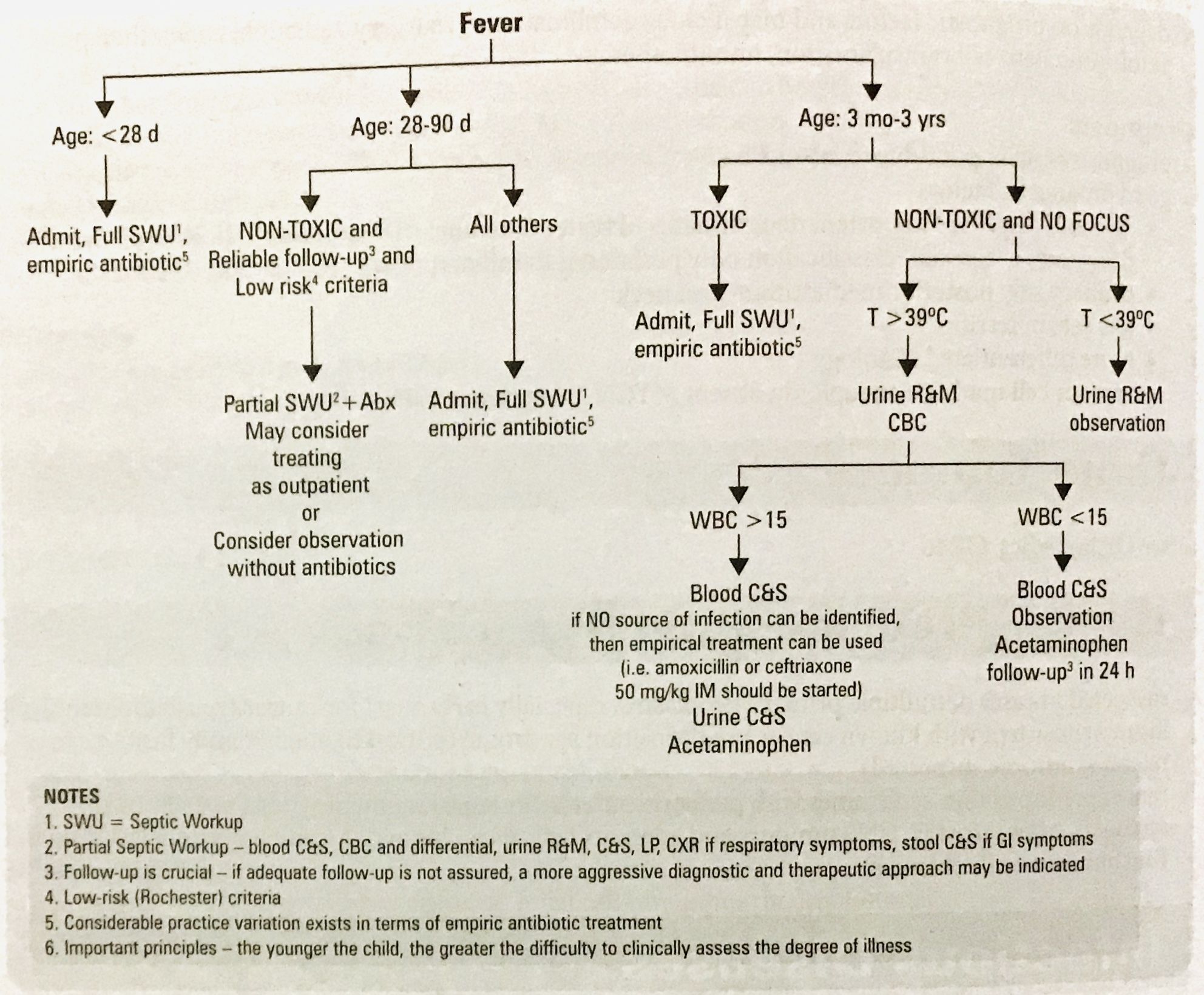
| Approach to febrile child | |
| Risk factors in erectile dysfunction | Glucose* (FPG and Hb1Ac), lipids profile*, TSH, CBC, urianalysis. Hypothalamic- pituitary- gonadal axis evaluation (testosterone, prolactin and LH) |
| Red flags / referral in erectile disfunction | “FAT PEN“ failed medical therapy, an atomic abnormality, trauma, psychogenic cause, endocrinophaty, need for neurological/ vascular assessment |
| Pharmacologic treatment for erectile disfunction | Phosphodiesterase type 5 inhibitors (sildenafil, tadalafil*longer, verdinafil) *never use with nitrates*. a-adrenergic blocker, serotonin antagonist and reputable blockers, testosterone. |
| Fatigue red flags | Fever, weigh loss, night sweating, neurological deficits, ill appearing |
| Definitions of fever in pediatrics | >38 C / 100.4 F, if <2 must be rectal >37.7C Fever without a source/focus it’s acute <10d, fever of unknown origin its daily or intermittent for at least 2 wk |
| Approach to febrile child | |
| Definition of migraine | >5 fulfilling each of the following: 4-72 hrs duration. >2: unilateral, pulsating, moderate-severe (interferes with daily activities) aggravated by physical activities. >1: N/V, photo/phono/osmophobia |
| Pharmacologic management in migraine headache | Mild-moderate: NSAIDs Moderate- severe: triptans (#1), ergots Prophylaxis: anticonvulsants (topiramate, gabapentin, divalproex), TCA, propranolol, CCBs, *oral contraceptive pills are contraindicated with complicated migraine due to the risk of stroke |
| Hypertension (HTN) definitions | Blood pressure (BP) >140/90, or 135/85 if ambulatory, >130/80 if DM or >150/90 if >80yr. Isolated Systolic HTN sBP> 140/<90 HTN urgency: >210 sBP or >120dBP with minimal or no target-organ damage. Malignant HTN: evidence of vascular damage on fundoscopy but without papilledema |
| Investigation in specific patients with HTN | DM or chronic kidney disease: urinary protein excretion. Renovascular HTN: renal usg, captopril renal scan, MRA/CTA, suspected if >2: sudden onset or worsening at>55/<30yrs, presence of abdominal bruit, resistance to 3or more drugs, rise in Cr of 30% or more associated with and ACEi or ARB, other atherosclerotic vascular disease, recurrent pulmonary edema associated with HTN surges. Endocrine cause: plasma aldosterone and renin ( ald/ren ratio) suspected when HTN resistant to 3or more drugs, spontaneous hypokalemia (<3mmol/L), incidental adrenal adenoma Pheochromocytoma: 24 hrs urine for metanephrine and creatinine |
| Management in HTN | DASH is the best way to decrease the BP, moderate exercise, BMI 18.5-24.9 and waist <102 men <88 women, avoid combining a non-DHP CCB (like diltiazem or verapamil) with a BB, monitor K and Cr when administering and ACEi/ARB + K sparing diuretic, not recommended BB as first line in >60yr, not recommended ACEi as monotherapy in African American, Long acting thiazides- type ( like chlorthalidone) diuretics are superior Than others for prevention of CVD, CAD and decreasing BP, |
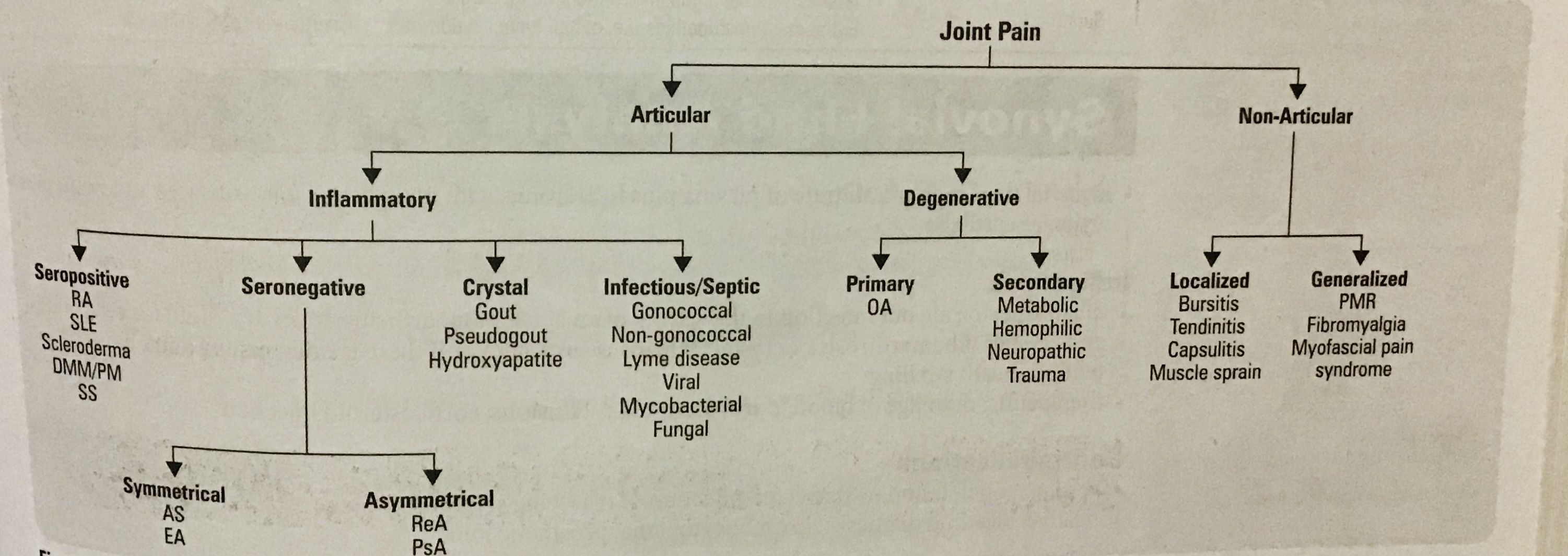
| Clinical approach to joint pain | |
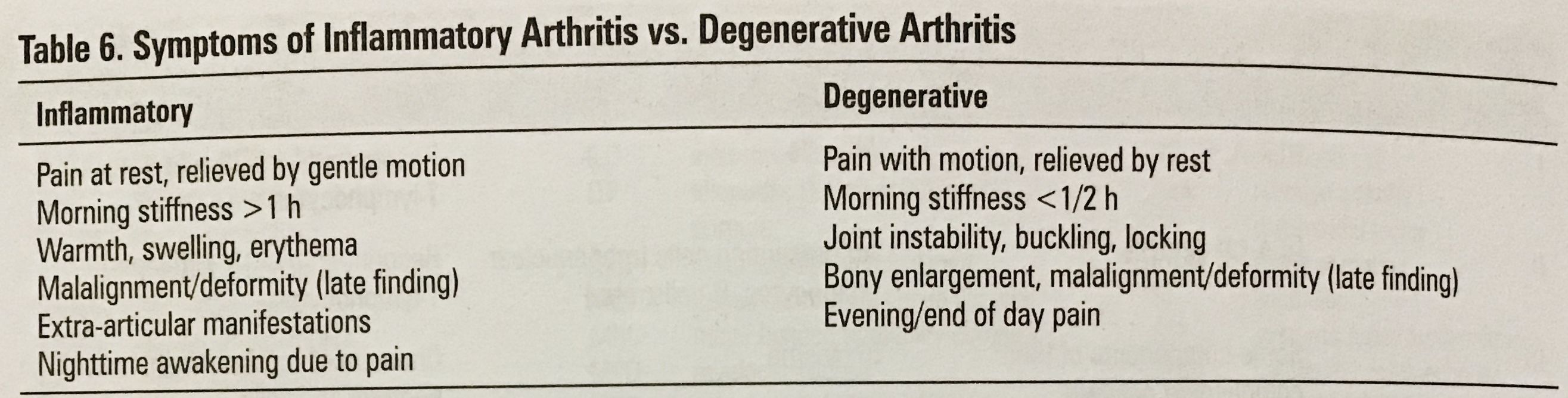
| Difference between inflammatory and degenerative arthritis | |
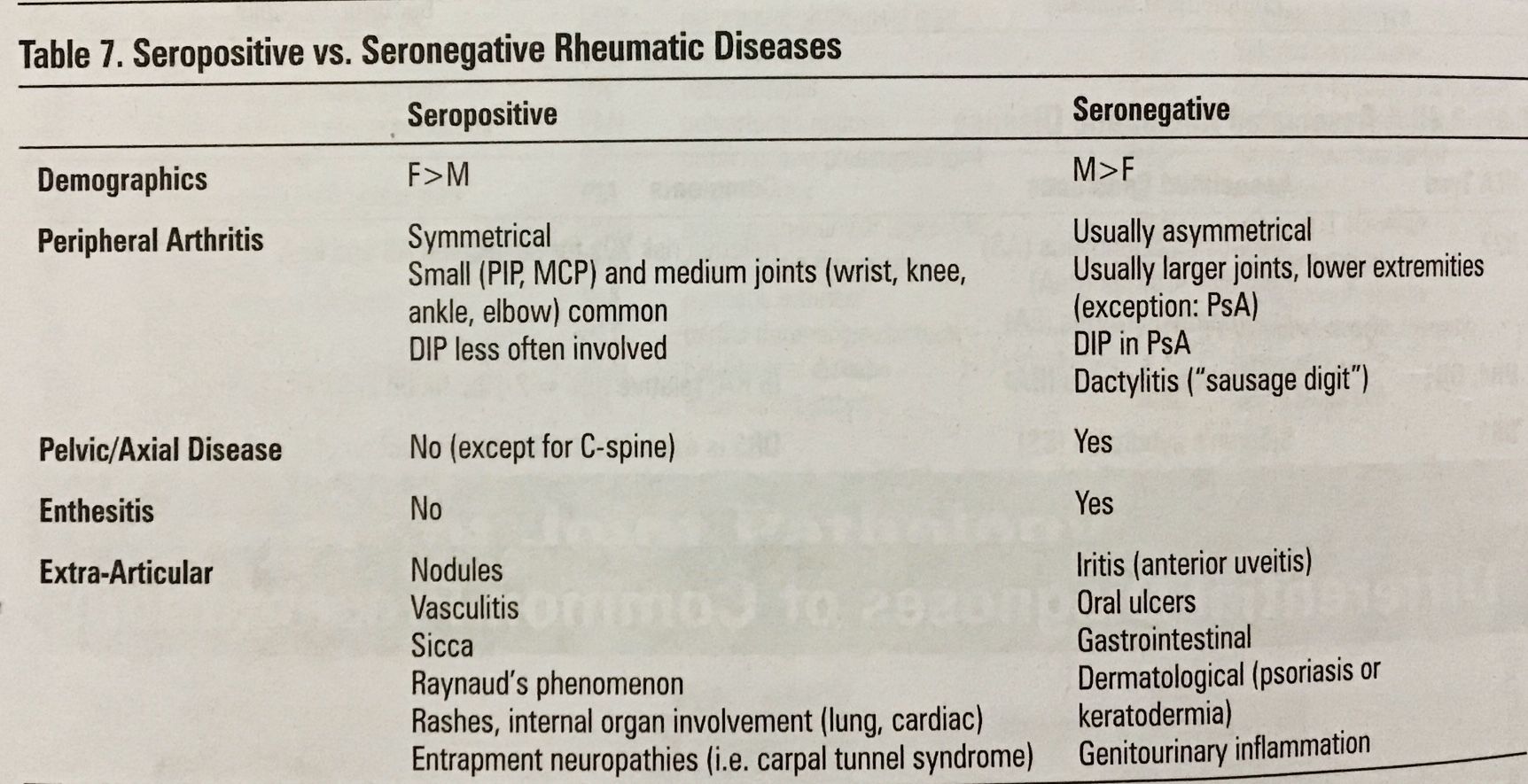
| Difference between seropositive and seronegative rheumatic disease | |
| Investigation in menopause | ▪️FSH and LH: increased levels of FSH (>35UI/L) on day 3 and FSH>LH. Decreased levels of estradiol are a late find. ▪️Osteoporosis: is the most important health hazard associated. ▪️CVD: its the leading cause of mortality in women post menopause. |
| Management for menopause symptoms | ▪️Vasomotor instability: HRT(#1), SSRI, venlafaxine, gabapentin, propranolol, clonidine and acupuncture. ▪️Vaginal atrophy: local estrogen, lubricants, HRT ▪️Urogenital: lifestyle changes, local estrogen, surgery ▪️Osteoporosis: 1000-1500mg Ca/d, 800-1000 vit D, weigh bearing exercises, smoking cessation, biphosphonates, selective estrogen receptors modifiers (SERM) like raloxifen. ▪️Decreased libido: vaginal lubrication and androgen replacement ▪️ CVD: evaluate risk factors ▪️Mood and memory: antidepressants (1#) , HRT Augments effects |
| Indications And benefits of hormone replacement therapy in menopause | The primary indication is vasomotor instability, helps with osteoporosis and ca of colon. Keep low doses (.3mg) and short duration (<5yrs). In the HRT there is an increased risk of breast cancer with estrogen + progesterone but not with estrogen only, progestin combinations are used in women with intact uterus to prevent developement of endometrial hyperplasia (the SERM don’t have this side effects on breast/uterine cancer, but does not help with vasomotor symptoms) |
| Side effects, risk and contraindications of HRT in menopause | ▪️Side effects: abnormal uterine bleeding, mastodynia, edema, bloating, heartburn, nausea, mood changes (progesterone), ▪️ Relative contraindications : uncontrolled HTN, hypertriglyceridemia, migraine, family history of cancer (estrogen ), chronic thrombophlebitis, DM related to CVD, gallbladder disease, fibrocystic disease (breast)▪️Absolute contraindications: “ABCD“ Acute liver disease, Undiagnosed vaginal Bleeding, Cancer history/ CVD, DVT. ▪️Risk: stroke, PE/DVT, breast ca, dementia and mild cognitive impairment |
| Definition and etiology of osteoporosis | Definition: bone mineral density (BMD) >2.5 standar deviations below. Osteopenia is a score between 1-2.5. Primary osteoporosis is the etiology in 95% of women and 80% in men. Secondary can be due to GI disease, bone marrow disorder, endocrinopathies, malignancy, drugs or COPD. |
| Clinical signs of fracture in osteoporosis | 1- height loss >3cm 2.- weight <5 kg 3.- kyphosis 4.- tooth count < 20 5.- grip strength 6.- arm span height difference > 5 cm 7.- wall occipital 0cm 8.- rib-pelvis distance <2 finger breadth (The most common fracture are hip, vertebrae, humerus and wrist) |
| Investigation in a patient with osteoporosis | 1.- all patients: calcium corrected for albumina, CBC, Cr, ALP, TSH 2.-consider serum and urine protein electrophoresisin vertebral Fx, celiac work up and 24 hrs urinary calcium to rule out secondary causes. 3.- 25-OH vit D levels shoul only be measured oafter3-4 mo of adequate supplementationand should not be repeated if > 75mmol/L 4.- consider X ray 5.- assess 10 yrs risk with WHO Fx risk (FRAX) and the Canadian tool (CAROC) |
| Indications for BMD test in younger adults (50yrs) | Fragility Fx, prolonged use of glucocorticoids or other high risk drugs (aroma tase inhibitors, androgen deprivation, anticonvulsivants), hypogonadism or premature menopause, malabsorption syndrome, Primary hyperparathyroidism |
| Management of osteoporosis based on a 10 yrs risk stratification | 1.- low risk <10%, encourage lifestyle changes reassess in 5 yrs 2.- medium risk 10-20% discuss preferences for management and consider risk factors, repeat BMD and reasses in 1-3 yrs 3.- high risk >20% or prior fragility Fx |
| Osteoporosis treatment | 1.-lifestyle: diet, elemental calcium 1000-1200 mg/day + 1000 UI/d, exercise 3 x 30min, stop smoking decrease caffeine intake and other drugs related to osteoporosis 2.- pharmacotherapy: *bisphosphonate: inhibit of osteoclasts binding (alendronate, risedrnate, zolendronic acid iv) * RANKL inhibitors (denosumab) * parathyroid hormone (teriparatide) for 18-24 mo duration followed by one of the ones above 3.- post menopausal women: selective estrogen receptor modulator (SERM) (raloxifen) prevent osteoporosis, improve lipid profile, decrease breast cancer risk but increase risk of DVT/ PE, Stroke, hot flashes and leg cramps |
| Disorders strongly associated with osteoporosis | Primary hyperparathyroidism, type 1DM, osteogenesis imperfects, uncontrolled hyperthyroidism, hypogonadism or premature menopause (<45ys), Cushing disease, chronic malnutrition or malabsorption, chronic liver disease, COPD, chronic inflammatory condition. |
| Treatment for seborrheic dermatitis | Face: ketoconazole cream 1d Or bid and or mild steroid d or bid Scalp: salicylic acid in olive oil or derma scotch lotion (peanut oil, mineral oil, fluocinolone 0.01%) to remove dense scales, 2% ketoconazol shampoo, steroid lotion. |
| Red flags in sinusitis | Altered mental status, headache, systemic toxicity, swelling of the orbit or change in visual acuity or EOM, neurological findings, signs of meningeal irritation, suspected I.C. Complication, |
| Rhinosinusitis clinical diagnose | 2 or more major symptoms + at least one of the symptoms is either nasal obstruction or purulent / discoloured nasal discharge: ▪️Major: facial pain/ pressure / fullness. Nasal obstruction, purulent / discoloured nasal discharge, hyposmia / anosmia ▪️Minor : headache, halitosis, fatigue, dental pain, cough, ear pain or fullness |
| Rhinosinusitis management | Mild- moderate: I.N. Corticosteroids if no response within 72hrs add Abx. Severe: I.N. Corticosteroids + Abx. 1st line amoxicillin x10d ( macrolide or TMP-SMX ir allergy) if no response within 72hrs switch to fluoroquinolones or amo-clavulanate + adjuvant therapy:saline or hypochlorous acid irrigation, analgesics, decongestant for symptomatic relief |
| Rhinosinusitis red flags | CT if complications are suspected. Consider hospitalization if any of the following: ▪️orbital cellulitis, abscess or thrombosis. ▪️I.C. : meningitis, abscess ▪️Bony: frontal bone abscess (Potts puffy tumor), osteomyelitis. ▪️Neurological: superior orbital syndrome (CN 3,4,6 palsy, immobile globe, dilated pupils, ptosis) Orbital apex syndrome ( same, plus neuritis, papilledema, decreased visual acuity) |
| Chronic rhinosinusitis | ▪️If polyps: I..N. Corticosteroids, oral steroids %Abx, reference ▪️No polyps: I.N.Corticosteroids, Abx for 3-6 wks, saline irrigation, %oral steroids ▪️Surgery( rare) |
| Antimicrobial treatment for Strep pharyngitis (GABHS) in children | ▪️1st: penicillin V 40mg/kg/P.O. Bid-tid x10d (max 750mg/d =27kg use adult dose) Or amoxicillin 40mg/kg/d P.O. Bid-tid x10d (max 500mg/dose =37kg) ▪️2nd etyrhomycin 40mg/kg/d P.O. Bid-tid x10d. (Max for severe infections 4000mg/d) ▪️3rd cephalexin 25-50mg/kg/d P.O. Qid x10d (max 2000mg/d =40kg) |
| Antimicrobial treatment for Strep pharyngitis (GABHS) in adults | ▪️1st penicillin V300mg p.o. Tid or 600mg bid x10d ▪️2nd erythromycin 250mg P.O. Qid x10d ▪️3rd cephalexin 250mg P.O. Qid x10d |
| Sinusitis treatment in children ( S. Pneumoniae, H. Influenzae, M. Catharralis, S.aureus ) | ▪️1st amoxicillin 80mg/kg/d P.O. Bid-tid x5-10d (max 3gr/d x10-14d = 37kg) ▪️Amo-clavulanate 40-80 mg/kg/d bid (max 3gr/d) x10-14d or cefprozil 30mg/kg/d P.O. Bidx10-14d. ▪️3rd cefuroxime 30-40mg/kg/d P.O. Bid x10-14d, clarithromycin 15mg/kg/d P.O. Bidx10-14d |
| Sinusitis treatment in adults (S. Pneumoniae, H. Influenzae, M. Catharralis, S.aureus ) | ▪️1st amoxicillin 500mg P.O. Tidx5-10d ▪️2nd amo-clavulanate 500-875mg P.O. Bid x5-10d or cefuroxime 250-500mg P.O. Bid x5-10d ▪️3rd levofloxacin 500mgP.O/d x5-10d |
| Acute otitis media treatment (S.pneumoniae, H.influenzae, M. Catarrhalis, GABHS, S.aureus) in children | Treat if <6mo. If 6-24mo follow up for 48-72hrs. If>24mo treat if worsen after 48-72hrs. If >24mo 5d treatment, <24mo 10d. ▪️1st amoxicillin 80mg/kg/d P.O. Bid-tid (max 3gr/d) ▪️2nd amo-clavulanate 40-80mg/kg/d P.O. Bid ▪️3rd cefuroxime 30-40mg/kg/d P.O. Bid or clarithromycin 15mg/kg/d P.O. Bid ▪️If chronic TM perforation use ciprodex optic suspension 4drops bid x5d |
| Acute otitis media treatment (S.pneumoniae, H.influenzae, M. Catarrhalis, GABHS, S.aureus) in adults | ▪️1ts amoxicillin 500mg P.O. Tidx7-10d ▪️2nd amo-clavulanate 500mg P.O tid or 875 mg P.O. Bid7-10d or cefprozil 250-500mg P.O. Bid x7-10d |
| Otitis externa treatment (S.aureginosa, coliforms, S.aureus) | Cortisporin (hydrocortisone, neomycin, polymyxin B) optic solution 4 drops tid-qid (3 in children) in necrotizing use ciproflozacin 750 mg P.O. Bid x 4-8wks |
| Dental infection / periodical and periodontal abscess treatment | Penicillin V potassium 500mg P.O. Qid x7-10d or Clin day in 300 mg P.O. Qid or 600mg bid x7-10d |
| Diarrhea- enteritis treatment (e.coli, campylobacter, salmonella, shigella, virus, Protozoa) | Mild to moderate: loperamide 4mg PO. STAT then 2mg after each loose (max 8 doses/day) or bismuth subsalicylate (pesto bismol) 2 tabs or 30ml repeat q30min prn (Max 8 doses per day) ▪️Moderate to severe: ofloxacin 400mg PO.S.D. Or 300mg P.O bid x3d or ciprofloxacin 750mg PO.S.D. Or 500mg bidx3d or levofloxacin 500mg p.o./d 1-3d or azithromycin 1gr P.O.S.D. Or 500mg x3d. (Azithromycin 10mg/kg/d is recommended in children and in high resistance to quinolone from campylobacter ) |
| Head and pubic lice (crabs) treatment | Permethrin cream 1% apply as liquid into washed hair for 10min then rise and repeat in 1 wk |
| Vulvovaginal candidiasis (VVC) treatment | Treat if patient is symptomatic, fluconazole 150mg P.O.S.D. Or metronidazole 2% cream intracranial qhs x 7 d |
| Bacterial vaginosis (BV) management and treatment | Treat in high risk pregnancy, prior IUD insertion, gynecological surgery, induced abortion or instrumentation. ▪️1st line metronidazole 500mg P.O. Bid x7d or cream, Clindamycin 2%cream x 7d. ▪️2nd 2gr metronidazole P.O.S.D. Or clindamycin 300mg P.O. Bid x 7 d |
| Mastitis treatment (S.aureus, S. Pyogenes) | Cloxacillin 500mg PO. Qid x 7d or cephalexin 500mg P.O. Qid x7d |
| Uncomplicated cellulitis treatment (S.aureus, S.pyogenes) | ▪️Children 1st cephalexin 50-100mg/kg/d qid x10-14d 2nd cloxacillin 50mg/kg/d qid x10-14d or clindamycin 25mg/kg/d x10-14d ▪️Adults: 1s cephalexin 500mg PO. Qidx10-14d 2nd cloxacillin 500mg PO.qid x10-14d or clindamycin 300mg qid x10-14d |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.