30021564
Description
Flashcards by Cyrielle Saba, updated more than 1 year ago
|
|
Created by Cyrielle Saba
about 3 years ago
|
|
| Question | Answer |
|
Image:
Pge1 (binary/octet-stream)
|
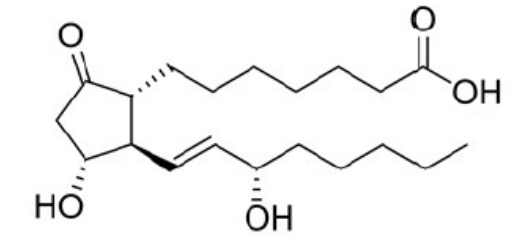
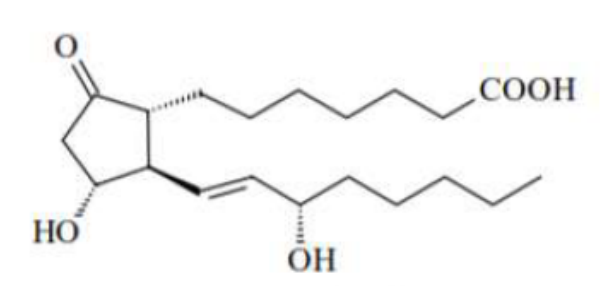
PGE1 increases renal blood flow + vasodilation inhibits gastric acid production-->increases the secretion of bicarbonate ion and mucus and maintains the mucosal blood flow cervical ripening, induction of labor/termination of pregnancy and postpartum hemorrhage limited use to reduce NSAIDs-induced gastric damage bcz ineffective orally and degrades rapidly parenterally by ox of 15-OH |
|
Image:
Pge2 (binary/octet-stream)
|
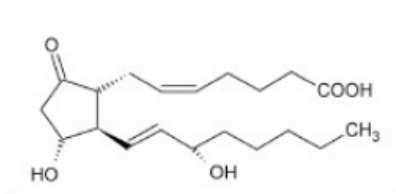
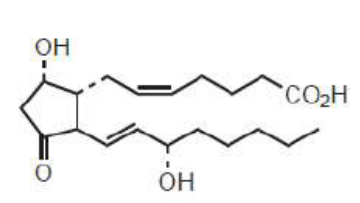
PGE2 (Dinoprostone) increases pain and fever promotes inflammation inhibits gastric secretions increases renal blood flow + vasodilation cervical ripening, induction of labor/termination of pregnancy |
|
Image:
Pgf2a (binary/octet-stream)
|
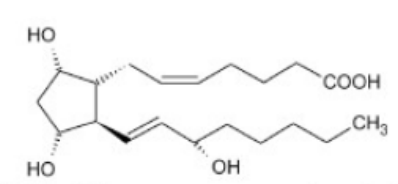
PGF2a (Dinoprost) mediates many aspects of reproduction decrease progesterone increase uterine contractions and termination of pregnancy and postpartum hemorrhage vasoconstriction bronchoconstriction |
| Carboprost (15-(S)-methyl-PGF2a) resistant to metabolic inactivation by ox at C15 | |
|
Image:
Pgi2 (binary/octet-stream)
|
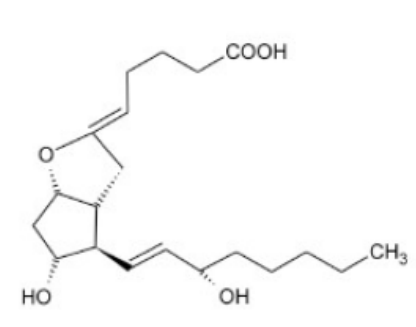
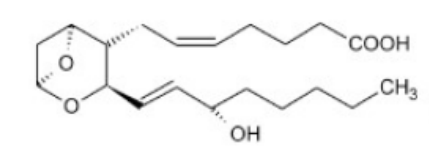
PGI2 decreases clotting and platelet aggregation relaxes smooth muscles increases renal blood flow + vasodilation inhibit gastric acid secretion |
|
Image:
Txa2 (binary/octet-stream)
|
TXA2 promotes clotting and platelet aggregation vasoconstriction |
|
Image:
Pgd2 (binary/octet-stream)
|
PGD2 increases renal blood flow inhibit gastric acid production |
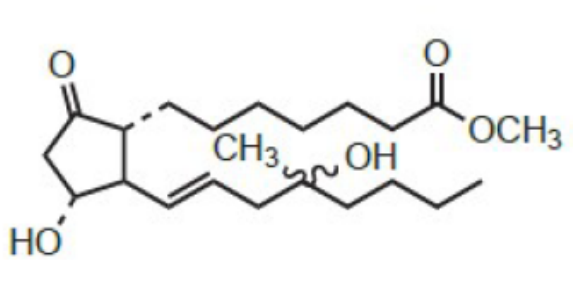
| Misoprostol PGE1 prodrug analog methyl ester ameliorates oral activity oxidation of 15-OH was overcome by moving OH to 16 +CH3 at 16 mixture of stereoisomers at 16 prevents NSAID-induced gastric ulcers can be misused for abortion | |
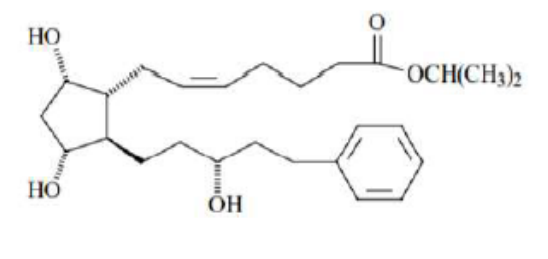
| Lanatoprost PGF2a prodrug analog eye drops to treat glaucoma by lowering intraocular pressure ester functionality facilitates penetration to ocular tissues aromatic ring protects from omega-ox | |
| Alprostadil PGE1analog vasodilation, inhibits platelet aggregation and stimulates intestinal and uterine smooth muscles to treat erectile dysfunction | |
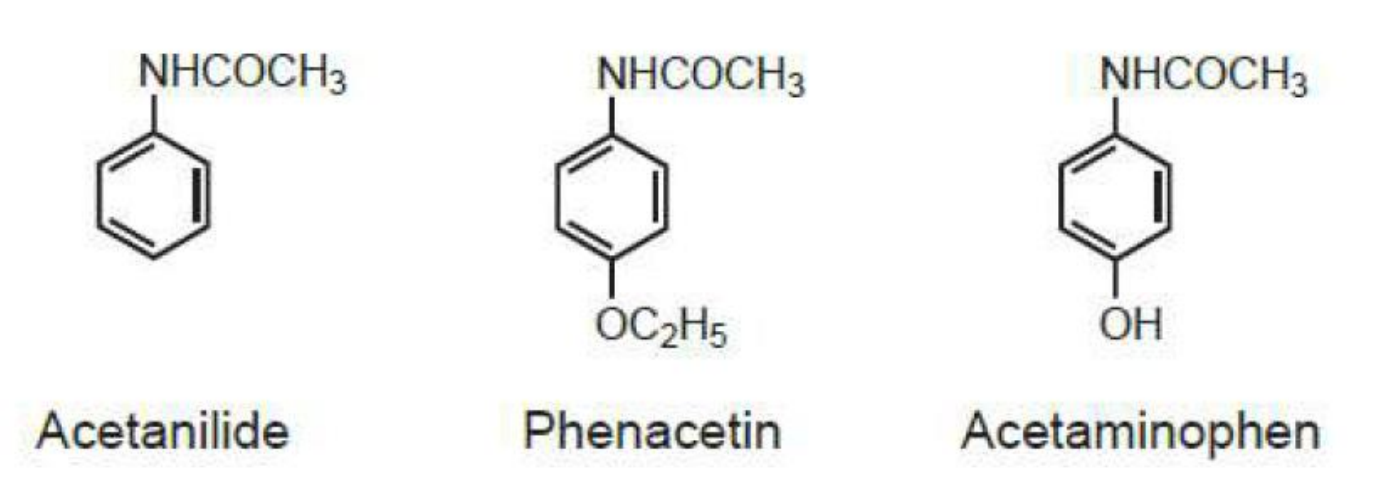
| p-aminophenols analgesics and antipyretics toxic (but less than aniline): methemoglobinemia and hemolytic anemia methyl/propyl ether on phenol--> more SE N-substitutiants that reduce basicity-->reduce activity unless can be metabolized like acetyl major metabolites of acetaminophen: sulfate and glucuronide but with alcohol (CYP2E1 and CYP3A4)-->NAPQI-->hepatotoxicity (detoxified with glutathione and N-acetylcysteine) | |
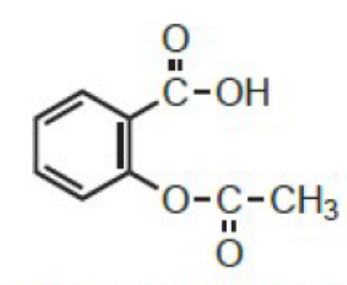
| Acetylsalicylic acid (aspirin) Salicylate covalently (irreversibly) modifies COX by acetylating COX1 (and COX2: more potent against COX1 than 2) hydrolyzed to salicylic acid in vivo-->salicylate anion is active (CA-->GI effects) acetyl group improves activity removal of hydroxyl-->weak activity no activity if phenol meta or para antipyretic, analgesic, anti infl, inhibit platelet aggregation by blocking COX1-->irreversibly blocks formation of TXA2 SE: GI tox, bleeding bcz of inhibition of platelet aggregation, aspirin hypersensitivity, Reye's syndrome, high PPB bcz of acidic grp-->DDI | |
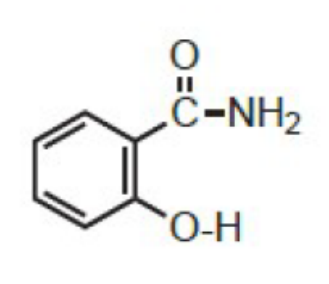
| Salicylamide Salicylate amide maintains analgesic action but no anti inflammatory no gastric irritation for individuals hypersensitive to aspirin | |
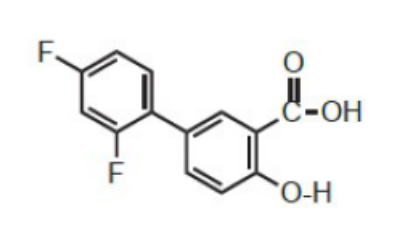
| Diflunisal Salicylate 5-substitution-->increases anti-inflammatory activity antipyretic, analgesic, anti infl, inhibit platelet aggregation by blocking COX1-->irreversibly blocks formation of platelet aggregating factor TXA2 SE: GI tox, bleeding bcz of inhibition of platelet aggregation, aspirin hypersensitivity, Reye's syndrome, high PPB bcz of acidic grp-->DDI | |
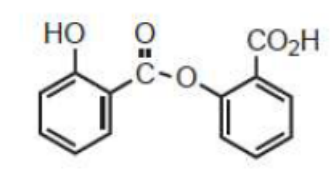
| Salsalate= salicylsalicylic acid (dimer of salicylic acid) Salicylate partially hydrolyzed to 2 salicylic acid antipyretic, analgesic, anti infl, inhibit platelet aggregation by blocking COX1-->irreversibly blocks formation of platelet aggregating factor TXA2 SE: GI tox, bleeding bcz of inhibition of platelet aggregation, aspirin hypersensitivity, Reye's syndrome, high PPB bcz of acidic grp-->DDI | |
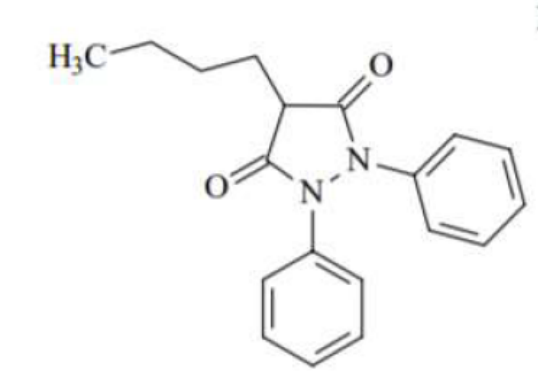
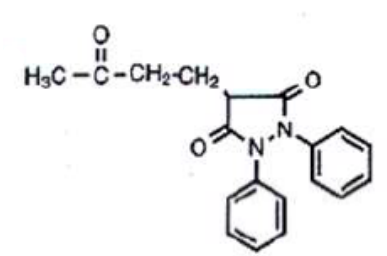
| Phenylbutazone pyrazolidinedione 4-H essential for anti infl 4-alkyl (n-butyl most) enhances anti infl discontinued bcz of agranulocytosis gives Oxyphenbutazone t1/2=50-65h to treat symptoms of gout, and RA CI if less than 14 y.o bcz of Na+ retention less potent than tolmetin also metabolized to γ-ketophenylbutazone (kebuzone) which is oxidized, active, and commercialized on its own | |
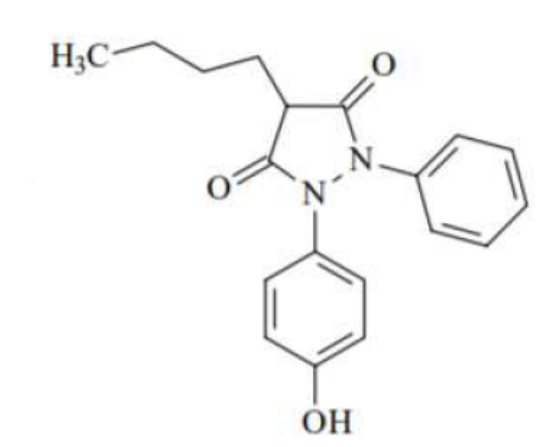
| Oxyphenbutazone pyrazolidinedione 4-H essential for anti infl 4-alkyl (n-butyl most) enhances anti infl active metabolite of phenylbutazone t1/2=50-65h to treat symptoms of gout, and RA CI if less than 14 y.o bcz of Na+ retention | |
| γ-ketophenylbutazone (kebuzone) active metabolite of phenylbutazone | |
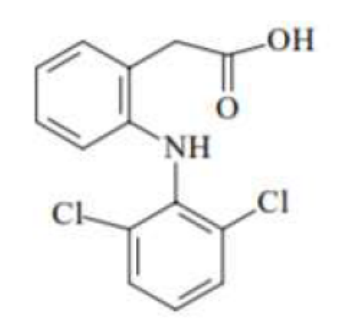
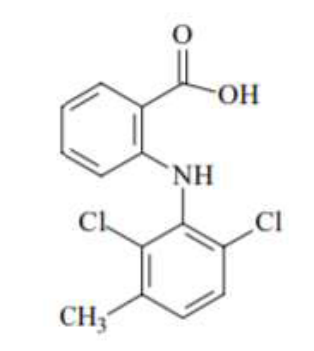
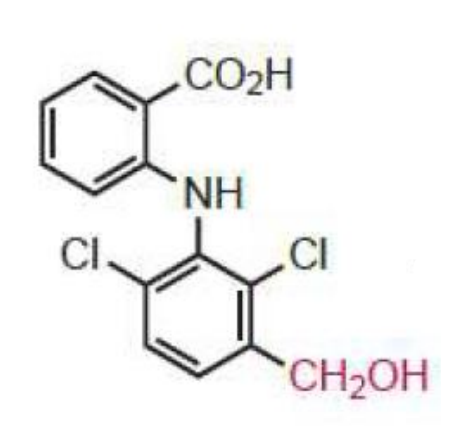
| Diclofenac Arylacetic acid (also anthranilic acid) 2o-chloro groups force the anilino-phenyl ring out of the plane of the phenylacetic acid portion one of the most potent inhibitors of COX associated with the high risk of heart attack and stroke inhibits COX and lipoxygenase inhibits arachidonic acid release and stimulates its uptake-->decrease arachidonic acid availability major metabolite: 4'-OH (weak activity) | |
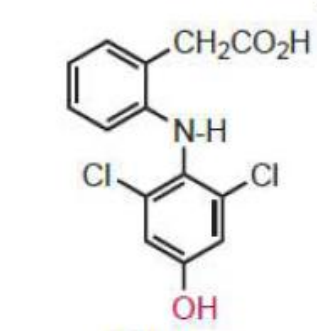
| 4'-OH major metabolite of Diclofenac (weak activity) | |
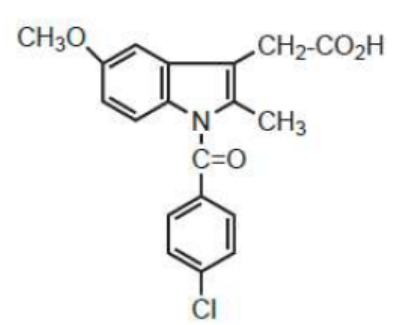
| Indomethacin Benzoylated indole nitrogen Methyl group at 2- of indole keeps the two aromatic rings noncoplanar highly PPB inactive metabolites more potent than tolmetin one of the most potent COX inhibitors but limited use bcz of severe SE (cardiovascular & GI) | |
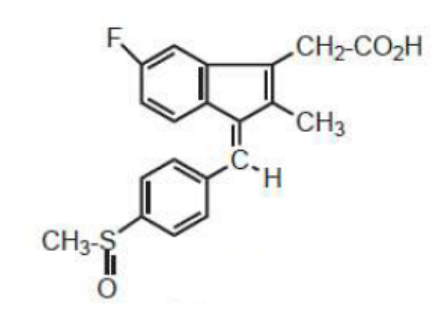
| Sulindac indene benzylidene replaces p-chlorobenzoyl-->decreased water solubility compensated by sulfinyl group C-C double bond restricts rotation-->noncoplanar ring inactive prodrug (1 active metabolite sulphide obtained by reduction to the sulfide) Z>potent than E | |
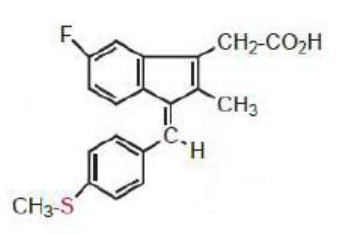
| Sulphide only active metabolite of Sulindac | |
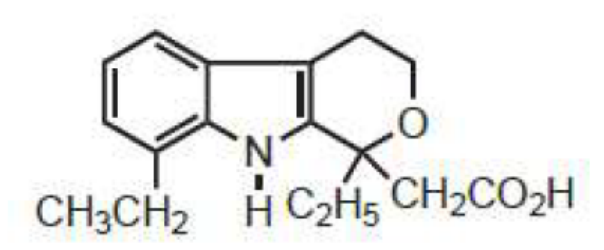
| Etodolac tetrahydropyranocarboxylic acid lengthening the acid chain or ester or amide derivatives gave inactive compounds inhibits COX2, uricosuric action, low risk of GI SE, highly PPB hydroxylated metabolites are all inactive | |
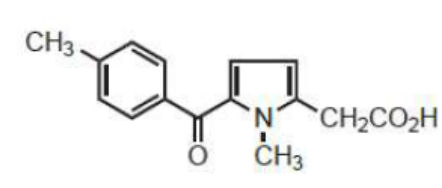
| Tolmetin pyrrole acetic acid(pyrrole ring containing noncoplanar benzoyl group and acetic acid function) short t1/2=1h due to rapid phase I ox of p-methyl to benzylic alcohol initially and to the acid (inactive metabolites) more potent than phenylbutazone and less than indomethacin | |
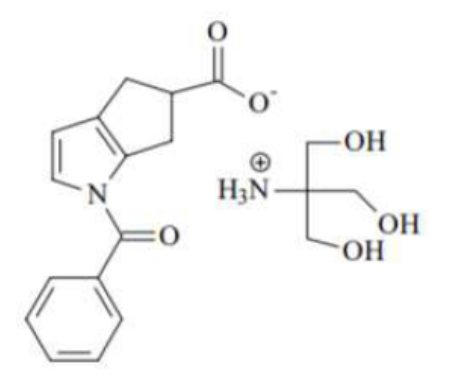
| Ketorolac pyrrole acetic acid longer t1/2=4-6h lacks benzylic methyl group most potent and effective NSAID analgesic (moderate anti-infl) very selective COX1 inhibitor-->highest incidence of SE (more gastrotoxic than other NSAIDs) | |
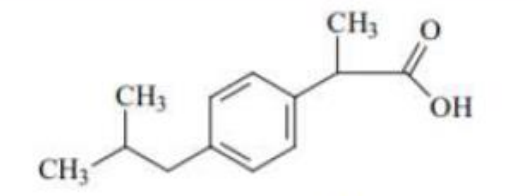
| Ibuprofen profen aryl/heteroarylpropionic acid anti-infl with analgesic and antipyretic increased COX inhibition activity ((S) is more potent) and less toxicity racemate no active metabolites | |
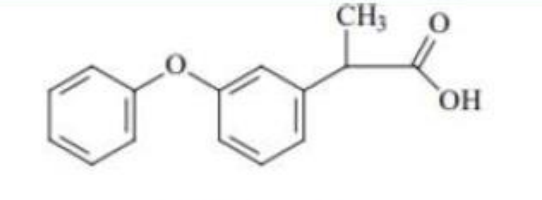
| Fenoprofen profen aryl/heteroarylpropionic acid anti-infl with analgesic and antipyretic increased COX inhibition activity ((S) is more potent) and less toxicity racemate | |
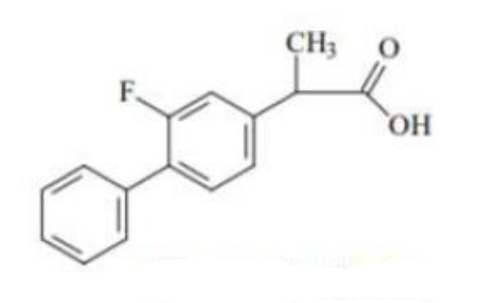
| Flurbiprofen profen aryl/heteroarylpropionic acid anti-infl with analgesic and antipyretic increased COX inhibition activity ((S) is more potent) and less toxicity racemate | |
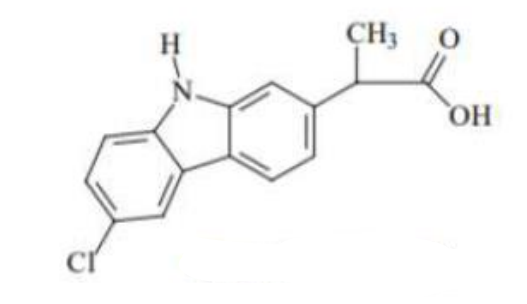
| Carprofen profen aryl/heteroarylpropionic acid anti-infl with analgesic and antipyretic increased COX inhibition activity ((S) is more potent) and less toxicity racemate | |
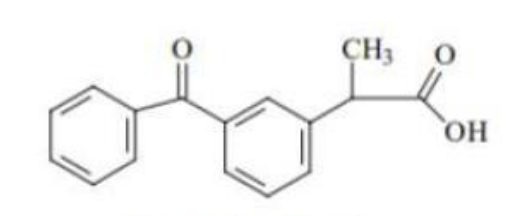
| Ketoprofen profen aryl/heteroarylpropionic acid anti-infl with analgesic and antipyretic increased COX inhibition activity ((S) is more potent) and less toxicity racemate | |
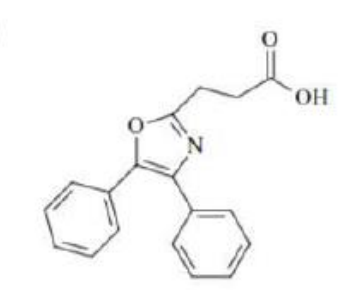
| Oxaprozin arylpropionic acid (profen) anti-infl with analgesic and antipyretic increased COX inhibition activity and less toxicity exception: substitution of propionic moiety is at 3- not 2-, prolonged DOA uricosuric properties to treat Gout | |
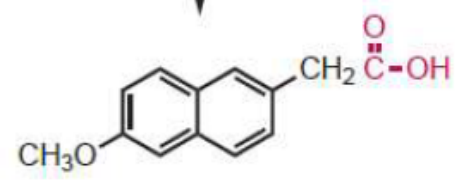
| Naproxen aryl/heteroarylpropionic acid (profen) anti-infl with analgesic and antipyretic increased COX inhibition activity ((S) is more potent) and less toxicity preferred nonselective NSAID when high cardiovascular risk not marketed as racemate | |
| Mefenamic acid Fenamate (N-phenylanthranilic acid derivative) substituents increase activity 2' and 3' force N-aryl ring out of coplanarity with anthranilic acid no active metabolites | |
| Meclofenamate Fenamate (N-phenylanthranilic acid derivative) substituents increase activity 2' and 3' alkyl or halogen--> no coplanarity 1 major active metabolite | |
| Meclofenamic acid major active metabolite | |
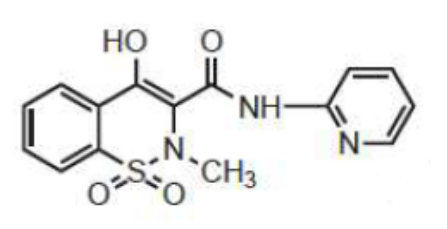
| Piroxicam Oxicam (Enolic acid) 4-hydroxy-1,2-benzothiazine carboxamide acidity attributed to 4-OH optimal activity obtained with methylamino and 2-pyridinyl groups pKa=6.3 (less acidic than CA NSAIDs-->less GI SE) long t1/2 no active metabolites | |
| Meloxicam Oxicam (Enolic acid) 4-hydroxy-1,2-benzothiazine carboxamide acidity attributed to 4-OH optimal activity obtained with methylamino and 2-pyridinyl groups thiazole-->selectivity over COX2 pKa=6.3 (less acidic than CA NSAIDs-->less GI SE) long t1/2 | |
| Nabumetone Naphtylalkanone non acidic prodrug-->low GI SE 6-methoxynaphthaleneacetic acid is major active metabolite Cl, CH3S, CHF2O at 6- -->retain activity replacement of carbonyl by CHO, CH2OH, COOCH3-->retain activity | |
|
Image:
6 Mna (binary/octet-stream)
|
6-NMA active metabolite of Nabumetone |
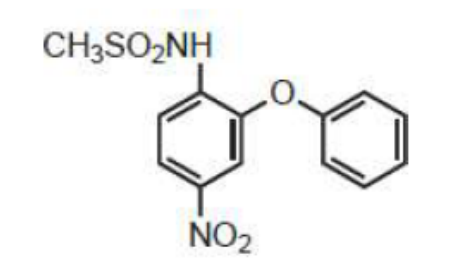
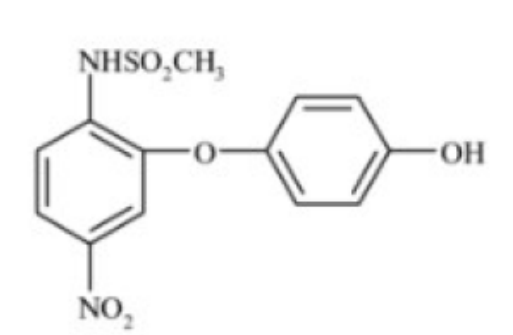
| Nimesulide Sulid COX2 selective inhibitor methyl sulfonamide-->selectivity 1 active metabolite (4'-hydroxynimesulide) | |
| 4'-hydroxynimesulide Nimesulide active metabolite | |
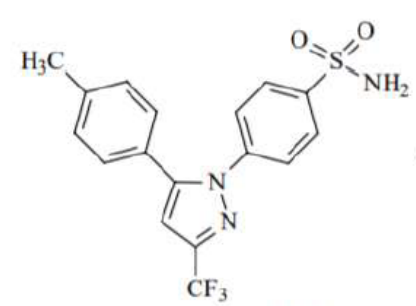
| Celecoxib Coxib COX2 selective inhibitor sulphonamide binds to hydrophilic region on COX2 only gastroprotective in the short term (6 months) but not in the long term (12 months)-->upper GI events potential for severe cardiovascular effects (suppress formation of PGI2-->high BP-->atherogenesis) inactive metabolites | |
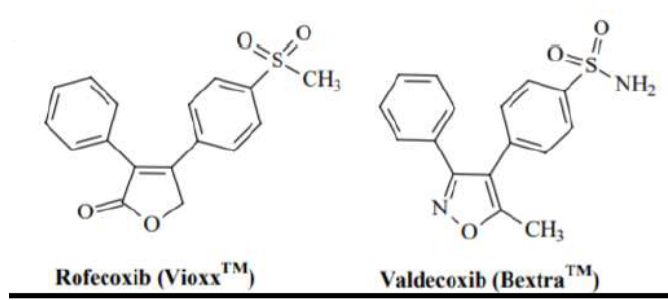
| Coxib COX2 selective inhibitors potential for severe cardiovascular effects (suppress formation of PGI2-->high BP-->atherogenesis)-->withdrawn from markets | |
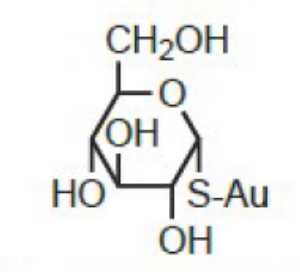
| Aurothioglucose Gold salt synthetic DMARD gold alters morphology and capabilities of human macrophages-->inhibit production of interleukins SE: dermatitis, mouth sores excretion (in case of toxicity) enhanced by chelating agents like Dimercapol (BAL) and Penicillamine high levels of gold persist after 20 days of injection decompose in aq solution after longstanding-->IM as suspension in sesame oil highly PPB | |
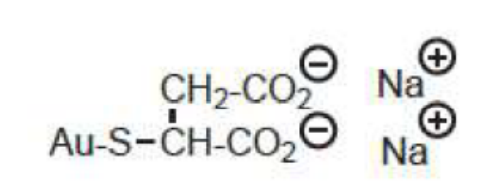
| Sodium aurothiomalate Gold salt synthetic DMARD gold alters morphology and capabilities of human macrophages-->inhibit production of interleukins SE: dermatitis, mouth sores excretion (in case of toxicity) enhanced by chelating agents like Dimercapol (BAL) and Penicillamine high levels of gold persist after 20 days of injection effective in slowing the development of progressive joint diseases orally ineffective-->IM water soluble highly PPB | |
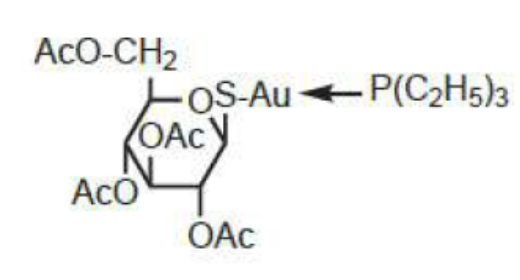
| Auranofin Gold salt synthetic DMARD gold alter morphology and capabilities of human macrophages-->inhibit production of interleukins SE: dermatitis, mouth sores excretion (in case of toxicity) enhanced by chelating agents like Dimercapol (BAL) and Penicillamine high levels of gold persist after 20 days first orally effective gold compound for arthritis complexation with triethylphosphine enhances oral bioavailability repurposed as potential antimicrobial agent +++against gram+ including multidrug resistant strains | |
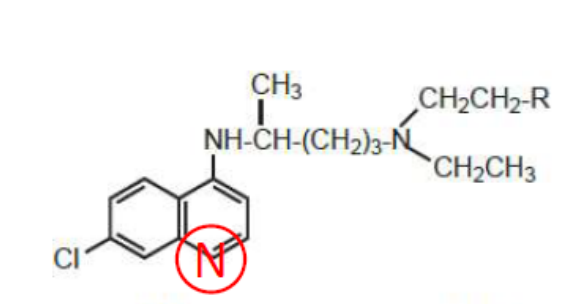
| Chloroquine (R=H) and Hydroxychloroquine (R=OH) 4-aminoquinoline synthetic DMARD (originally antimalarial drugs) Chloroquine has renal and corneal toxicity-->limited use Hydroxychloroquine sulfate (oral, water soluble) is less toxic but less effective | |
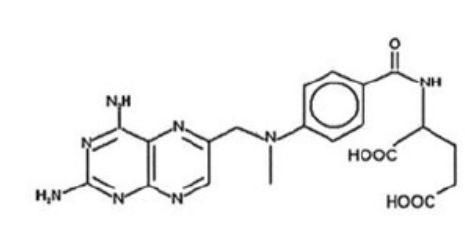
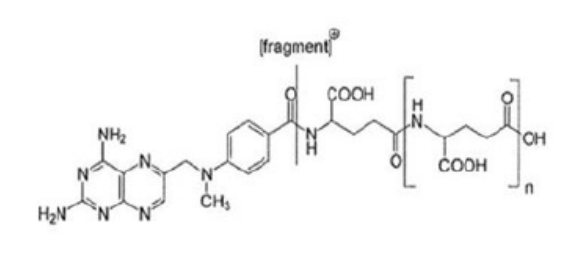
| Methotrexate immunosuppressant synthetic DMARD-->cytotoxic causes an increase in adenosine (anti-infl effect)+reduction in # activated T cells amd reduction in TNFa levels orally (food delays absorption) 2 active metabolites: methotrexate polyglutamates and 7-hydroxymethotrexate synergistic combination with TNF inhibitors | |
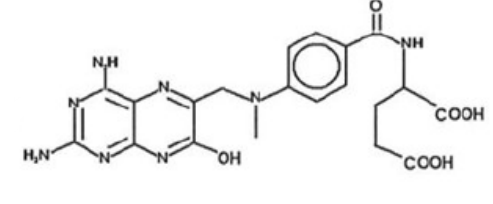
| methotrexate polyglutamates active metabolite of methotrexate | |
| 7-hydroxymethotrexate active metabolite of methotrexate | |
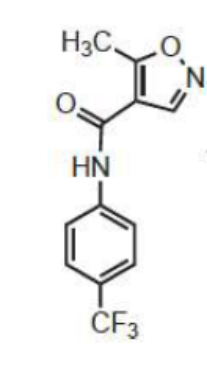
| Leflunomide immunosuppressant synthetic DMARD-->cytotoxic orally prodrug-->teriflunomide (active a-cyanoenol metabolite) C3-H of isoxazole ring is required ring opening | |
| Teriflunomide active a-cyanoenol metabolite of Leflunomide inhibits pyrimidine denovo synthesis by inhibiting dihydroorotate dehydrogenase-->decreases B cell and T cell proliferation, blocking the synthesis of immunosuppressive cytokines undergoes primarily enterohepatic circulation, extending its DOA | |
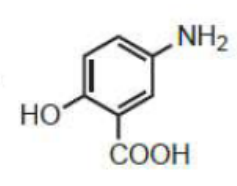
| Sulfasalazine immunosuppressant synthetic DMARD-->cytotoxic prodrug: hydrolyzed by colonic bacteria into 5-ASA and sulfapyridine | |
|
Image:
5 Asa (binary/octet-stream)
|
5-ASA inhibitor of prostaglandin biosynthesis inhibits release of inflammatory cytokines and TNFa inhibits lipoxygenase to treat colon inflammation: Crohn's disease |
| Tofacitinib orally active immunosuppressant synthetic DMARD-->cytotoxic specifically inhibits JAK3, blocking proinflammatory cytokine signaling-->prevents expression of B and T cells to treat adults with RA who cannot take methotrexate | |
| Soluble TNFR; Etanercept anti-TNFa antibodies; Infliximab, Adalimumab, Certolizumab | TNF inhibitors (cytokine inhibitor) biologic DMARD neutralize the effects of TNF-->reduce symptoms of RA within 1-2 weeks and slow progression of disease work synergistically with methotrexate |
| Rituximab | Biologic DMARD monoclonal AB that targets B lymphocytes originally used to treat non-Hodgkin lymphoma, also used in chronic lymphocytic leukaemia high risk to infections |
| Anakinra | Interleukin-I receptor antagonist Biologic DMARD high risk to infections IL-I binds to IL-1R1 and increases formation of NO, PGE2 and collagenase in synovial cells-->cartilage degradation and stimulation of bone resorption Anakinra is a recombinant IL-IRa that prevents binding of IL-I to IL-1R1-->decrease inflammatory response |
| Tocilizumab | IL-6 antagonist Biologic DMARD high risk to infections recombinant anti-human IL-6 receptor monoclonal AB that binds to soluble and membrane-bound IL-6 receptors, inhibiting IL-6 mediated signaling has efficacy slightly higher than methotrexate but with slightly higher incidence of SE |
| Abatacept | T-cell costimulation blocker Biologic DMARD high risk to infections prevents the generation of positive costimulation signals and stimulation of T-cell activation-->suppresses the proliferation of reactive T-cell and the release of more cytokines that destroy tissue-->reduce symptoms of arthritis |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.