30056005
Description
Flashcards by Nour Chidiac, updated more than 1 year ago
|
|
Created by Nour Chidiac
almost 5 years ago
|
|
| Question | Answer |
| How are Leukotrienes synthesized? | - From arachidonic acid which is a precursor to all leukotrienes. - Arachidonic acid is a carboxylic acid with a 20-carbon chain and four double bonds 20:4(ω-6), or 20:4(5, 8, 11, 14). - Arachidonic acid is metabolized by 5-lipooygenase to 5-hydroperoxyeicosatetraenoic acid (HPETE) - Leukotrienes are divided into 2 classes: 1. Hydroxylated eicosatetraenoic acids (LTs), e.g., LTB4 (2 OH) 2. Peptidoleukotrienes (pLTs) or cysteinyl leukotrienes, e.g., LTC4, LTD4, and LTE4 (DO NOT memo structures, easy to recognize bcz they have an AA) |
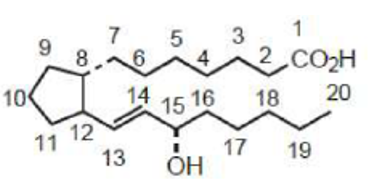
| What do all naturally occurring prostaglandins possess? | -15α-hydroxyl group (α; dotted, going into the page) - Trans double bond at C-13 - Classified (A, B, C, D, E, F, G, H, and I) depending on the nature and stereochemistry of oxygen substituents at the 9- and 11- positions (main structures we’re going to see are D, E, F, and I). - A subscript, 1 to 3, indicates the number of double bonds in the molecule. - Prostaglandin F has an additional subscript, either α or β, that designates the configuration of the hydroxyl at C-9. |
|
Image:
1 (binary/octet-stream)
|
General structure of naturally occurring prostaglandins. |
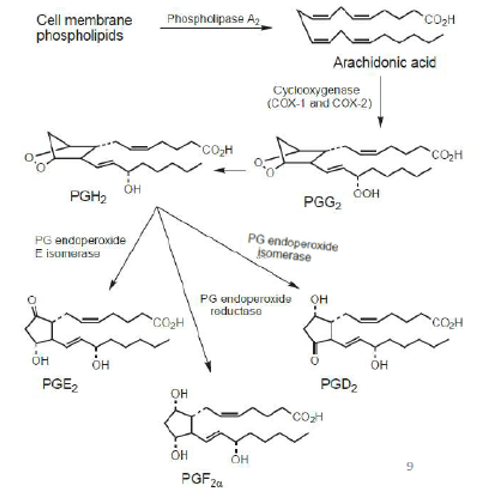
| How are prostaglandins synthesized? |
Image:
2 (binary/octet-stream)
|
| What are some properties of PG? | - Are synthesized in virtually every cell in the body, but different PGs are produced by different cell types. - Work right within the cells where they are synthesized; act locally because of short T1/2. Are involved in the inflammatory response, causing edema, swelling and prolonged erythema by increasing capillary permeability. - Play a cytoprotective role in maintaining the integrity of the gastric mucosa: * PGEs and PGI2 inhibit gastric secretion. * PGE1 stimulates the secretion of an alkaline mucus and bicarbonate ion and maintains mucosal blood flow. The use of PGE1 to reduce NSAID-induced gastric damage is limited because it is ineffective orally and degrades rapidly on parental administration, primarily by oxidation of the 15-hydroxy group. To overcome this, they produced a drug called misoprostol (Cytotec) * Inhibition of PG biosynthesis in the GIT disruption of mucosal integrity ? peptic ulcers - Inhibition of PG formation in joints ? reduces fever, pain and swelling |
|
Image:
3 (binary/octet-stream)
|
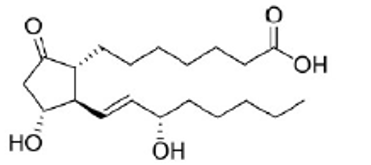
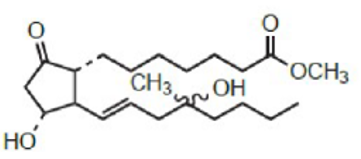
PGE1 - Inhibits gastric acid secretion - Cervical ripening, induction of labor on termination of pregnancy - Increase renal blood flow |
|
Image:
4 (binary/octet-stream)
|
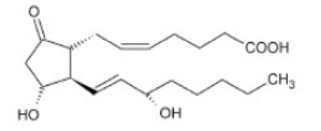
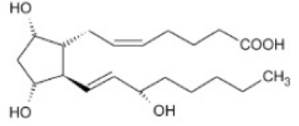
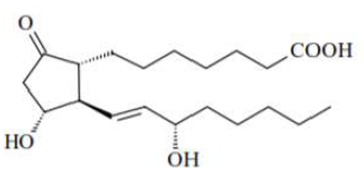
PGE2 • Increases pain and fever • Promotes inflammation • Inhibits gastric acid secretion • Increase renal blood flow • Cervical ripening, induction of labor, pregnancy termination and postpartum hemorrhage |
|
Image:
5 (binary/octet-stream)
|
PGF2α • Mediates many aspects of reproduction • Decreases progesterone • Increases uterine contraction, cervical ripening and induction of labor • Vasoconstriction • Bronchoconstriction • Can be formulated as 15-(S)-methyl-PGF2α which is resistant to metabolic inactivation by oxidation at the 15-position |
|
Image:
6 (binary/octet-stream)
|
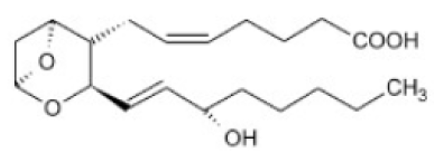
TXA2 (Thromboxane) • Promotes clotting • Promotes platelet aggregation • Constricts smooth muscles |
|
Image:
7 (binary/octet-stream)
|
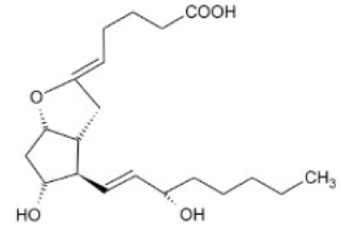
PGI2 (prostacyclin) • Decreases clotting • Decreases platelet aggregation • Relaxes smooth muscles • Increases renal blood flow (slight risk of kidney damage when inhibited) • Inhibit gastric acid production |
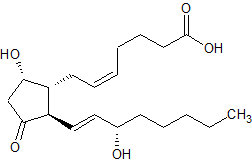
| PGD2 • Increases renal blood flow • Inhibits gastric acid production | |
|
Image:
9 (binary/octet-stream)
|
Misoprostol (Cytotec) • Prostaglandin prodrug analog. • Methyl ester ameliorates oral activity (improves absorption through gut membrane). • Oxidation of the 15-hydroxy group was overcome by: * Moving the hydroxyl group to C-16. * Introducing a methyl group at C-16 • Mixture of stereoisomers at the C-16 position • Use: prevention of NSAID- induced gastric ulcers. • Can be misused for abortion. |
|
Image:
10 (binary/octet-stream)
|
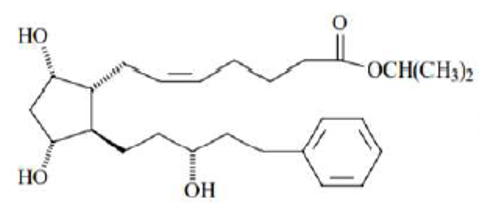
Latanoprost • F2α analog • Exists as eye drops. • For the treatment of open angle glaucoma by lowering the intraocular pressure. • Prodrug: ester functionality facilitates the penetration to ocular tissues • Aromatic ring protects from omega-oxidation (instead of methyl) |
|
Image:
12 (binary/octet-stream)
|
Alprostadil (PGE1) • Induces vasodilation, inhibits platelet aggregation and stimulates intestinal and uterine smooth muscle contraction. • Indicated for the treatment of erectile dysfunction. |
| What do NSAIDs do? | • They inhibit prostaglandin synthesis at the COX step ? profound effect on the reduction of inflammation. • COX-1: produces prostaglandins involved in the protection of the gastric mucosa and the maintenance of platelet and kidney function. • COX-2: produces prostaglandins at inflammatory sites (decrease pain, fever and inflammation). • Selective COX-2 inhibitors can eliminate side effects associated with COX-1 inhibition, such as gastric and renal effects. |
| What are the side effects of NSAIDs? | • GI toxicity • Renal disorders • Gastric damage caused by a dual insult mechanism: o Most NSAIDs are acidic substances that cause direct acid damage and a back diffusion of hydrogen ions. o ON TOP OF THAT they inhibit prostaglandin biosynthesis in the GIT, where prostaglandins exert a cytoprotective effect. |
| Which NSAIDs are p-aminophenols and what do they serve as? | Acetanilide, phenacetin and acetaminophen; they are analgesics and antipyretics • Acetanilide and phenacetin are metabolized to acetaminophen in vivo (by hydroxylation and deethylation respectively) • Both discontinued due to toxicity. • Aminophenols are less toxic than the corresponding aniline but remain toxic. • Acetaminophen has analgesic and antipyretic activity but very little anti-inflammatory effects. It is rapidly absorbed and has a half-life of 2-3 hrs. |
|
Image:
13 (binary/octet-stream)
|
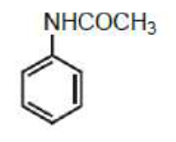
Acetanilide NSAID |
|
Image:
14 (binary/octet-stream)
|
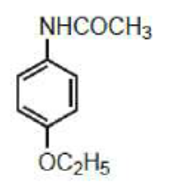
Phenacetin NSAID |
|
Image:
15 (binary/octet-stream)
|
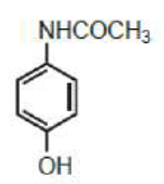
Acetaminophen NSAID |
| What is the SAR of acetaminophen? | - Esterification of the phenolic function with methyl or propyl groups produces derivates with greater side effects than with ethyl groups. (e.g., phenacetin) - Substituents on the nitrogen atom that reduce basicity reduce activity unless that substituent is metabolically labile (e.g., acetyl) |
| How are p-aminophenols metabolized? | - Acetanilide and Phenactine are metabolized into aniline by N-deacetylation to give aniline which is toxic and causes methemoglobinemia and hemolytic anemia. - Acetaminophen and Phenacetin are metabolized to hydroxyl amines by CYP2E1 and CYP3A4, which is then metabolized to N-acetylimido quinone (NAPQI) which is hepatotoxic, reacts with hepatic proteins and leads to hepatic necrosis and renal failure. BUT in the body, Glutathione naturally detoxifies NAPQI by binding to it and promoting its excretion as mercapturic acid or cysteine conjugates. - When overdoses, there is not enough glutathione for detoxification which leads to hepatic necrosis and renal failure. |
| Does alcohol affect the metabolism of p-aminophenols? If yes how? | - CYP2E1 and CYP3A4 play a role in the metabolism of p-aminophenols. - They are induced by the ingestion of alcohol. - Toxicity is observed upon the concomitant consumption of alcoholic beverages with acetaminophen (more NAPQI). |
| What is an antidote for p-aminophenol overdose? | N-acetylcysteine - It acts as a substitute for the depleted glutathione. |
| What are the classes of NSAIDs? | 1. Salicylates: acetylsalicylic acid, salicylamide, diflunisal, salsalate. 2. Pyrazolidinediones: phenylbutazone, oxyphenbutazone. 3. Aryl/heteroaryl acetic acids: diclofenac, indomethacin, sulindac, etodolac, tolmetin, ketorolac. 4. Aryl propionic acids (profens): ibuprofen, fenoprofen, carprofen, flurbiprofen, ketoprofen, naproxen, oxaprozin. 5. Anthranilic acid derivatives: mefenamic acid, meclofenamate. 6. Oxicams: piroxicam, meloxicam. 7. Napthylalkanones: nabumetone. |
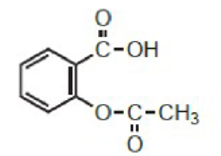
| What is the MOA of salicylates? | • Aspirin covalently (irreversibly) modifies COX by acetylating COX-1 and COX-2. It is hydrolyzed to salicylic acid in vivo. • Aspirin is more potent against COX-1 than COX-2 |
| What is the SAR of acetylsalicylic acid? | - Salicylate anion is the active moiety. The GI effects of aspirin are associated with the carboxylic acid function. - Acetyl group at position 2 is required for activity. - Removal of hydroxyl group to give benzoic acid (salicylate) results in a weak anti-inflammatory activity. - Placing the phenolic hydroxyl group meta or para to the carboxylic group leads to inactivation. |
|
Image:
16 (binary/octet-stream)
|
Acetylsalicylic acid (Aspirin) |
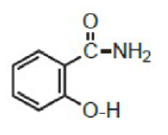
| What is the SAR of salicylamide? | - Amide maintains the analgesic actions of salicylic acid derivatives but eliminates the anti-inflammatory properties. (because lacks carboxyl group) - Salicylamide lacks gastric irritation of aspirin; it is used in individuals hypersensitive to aspirin. |
|
Image:
17 (binary/octet-stream)
|
salicylamide |
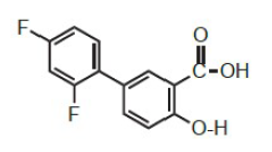
| What is the SAR of diflunisal? | - Substitution of aromatic rings at the 5-position of salicylic acid increases the anti-inflammatory activity. - Hint in naming: di - flunisal (2 Fs) |
|
Image:
18 (binary/octet-stream)
|
Diflunisal |
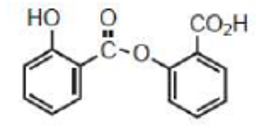
| What is the SAR of salsalate | - Also known as salicylsalicylic acid. - Dimer of salicylic acid. - Partially hydrolyzed to two molecules of salicylic acid. - Not active as is and has to undergo hydrolysis. |
|
Image:
19 (binary/octet-stream)
|
Salsalate |
| What role do salicylates have? | - They have antipyretic, analgesic and anti-inflammatory properties. - They inhibit platelet aggregation by blocking COX-1 in platelet membranes ? irreversibly blocking the formation of the TXA2, which is a potent platelet aggregation factor. |
| What are the side effects of salicylates? | • GI toxicity • Increased tendency towards bleeding (inhibit platelet aggregation) • Aspirin hypersensitivity (block PG synthesis ? more leukotrienes synthesis and more activation of the immune system) • Associated with Reye’s syndrome • Acidic group responsible for their high binding to plasma proteins ? DDIs |
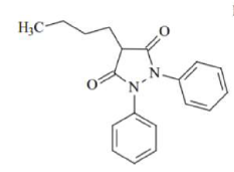
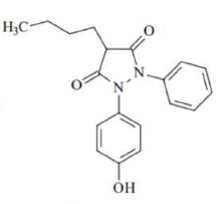
| What is the SAR of Pyrazolidinediones and which drugs belong to this class? | • Acidic H at position 4 is essential for anti-inflammatory activity. • Alkyl group at position 4 enhances anti-inflammatory activity, n-butyl is most active. Drugs: Phenylbutazone, oxyphenbutazone |
|
Image:
20 (binary/octet-stream)
|
- Used in the treatment of painful symptoms of gout and rheumatoid arthritis. - Contraindicated in children under 14 due to Na+ retention. - Discontinued due to agranulocytosis. - γ-ketophenylbutazone (kebuzone) is oxidized, active and commercialized on its own. |
|
Image:
21 (binary/octet-stream)
|
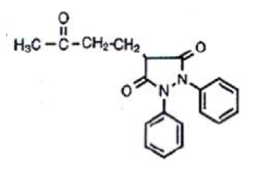
γ-ketophenylbutazone (kebuzone) - Active metabolite of phenylbutazone (by oxidation) - Commercialized on its own |
|
Image:
22 (binary/octet-stream)
|
Oxyphenbutazone - Hydroxylated active metabolite of phenylbutazone - T1/2 = 50-65 hrs |
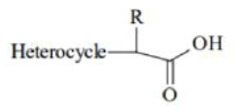
| What are aryl and heteroaryl alkanoic acids and how are they subclassified? | - They are derivatives of acetic acid - They are subclassified as 1. Aryl acetic acids: diclofenac 2. Indene/indoles: indomethacin, sulindac 3. Tetrahydropyranocarboxylic acid: etodolac 4. Pyrroles: tolmetin, keterolac |
|
Image:
23 (binary/octet-stream)
|
General structure for heterocyclic Acetic Acids. |
|
Image:
24 (binary/octet-stream)
|
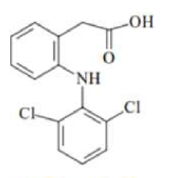
Diclofenac - Aryl acetic acid - Has structural characteristics of both aryl alkanoic acid and anthranilic acid classes. - 2 o-chloro groups force the anilino-phenyl ring out of the plane of the phenylacetic acid portion (rings not coplanar) - One of the most potent inhibitors of COX enzyme - Associated with a high risk of heart attack and stroke. - Inhibits both COX and lipoxygenase (acts on many levels that is why potent) - Inhibits arachidonic acid release and stimulates its uptake ? decreases arachidonic acid availability. - Metabolism: hydroxylation. All hydroxylated metabolites are inactive except the 4’-hydroxy metabolite which is the major metabolite and has weak activity. |
|
Image:
25 (binary/octet-stream)
|
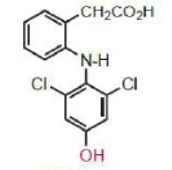
4'-hydroxy metabolite of diclofenac - Obtained by hydroxylation - Major and active |
|
Image:
26 (binary/octet-stream)
|
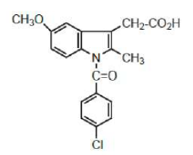
Indomethacin - Benzoylated indole nitrogen. - The methyl group at position 2 of the indole ring keeps the two aromatic ring noncoplanar. - One of the most potent inhibitors of COX but severe adverse effects limit its usefulness (high cardiovascular risk, significant GI toxicity). - Highly bound to plasma proteins. - Inactive metabolites by hydroxylation, N-deacetylation and glucuronidation |
|
Image:
29 (binary/octet-stream)
|
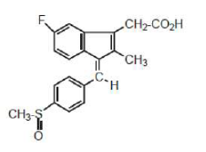
o Benzylidene replaces p-chlorobenzoyl ? decreased water solubility compensated by sulfinyl group. - N is not needed for activity. - Carbon-carbon double bond in sulindac restricts rotation and keeps the two aromatic rings noncoplanar. - Inactive prodrug. Active metabolite is obtained by reduction to the sulfide. - Not as high cardiovascular risk as indomethacin. - Z isomer is more potent than the E isomer. - Inactive metabolites by hydroxylation, oxidation and glucuronidation. Only the sulfide metabolite is active. |
|
Image:
28 (binary/octet-stream)
|
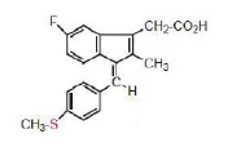
Sulfide metabolite of Sulindac Active |
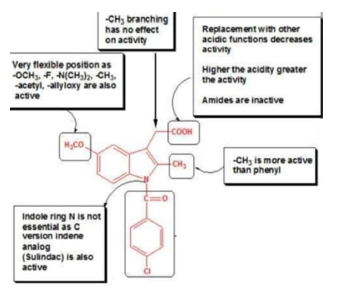
| What is the SAR of Indene and Indole Acetic Acids? |
Image:
30 (binary/octet-stream)
|
|
Image:
31 (binary/octet-stream)
|
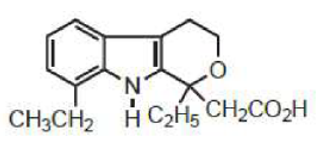
Etodolac - Tetrahydropyranocarboxylic acid - Lengthening the acid chain or ester or amide derivatives gave inactive compounds. - Preferentially inhibits COX-2. Low risk of GI side effects. - Has uricosuric activity. - Highly bound to plasma proteins. - Metabolites are hydroxylated and all are inactive. |
|
Image:
1 (binary/octet-stream)
|
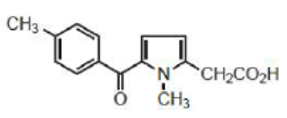
Tolmetin - Pyrrole acetic acid - Pyrrole ring contains a non-coplanar benzoyl group and an acetic acid function. - Short half-life (1 hr.) due to rapid phase 1 oxidation of the para-methyl group to a benzylic alcohol initially and then to the acid (both are inactive). - More potent than phenylbutazone and less than indomethacin. - Developed ketorolac as an improved tolmetin. |
|
Image:
2 (binary/octet-stream)
|
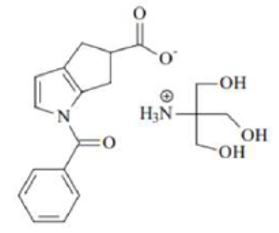
Ketorolac - Has a longer half-life (4-6 hrs) and lacks benzylic methyl group. - Most potent and most effective NSAID analgesic, only moderate anti-inflammatory activity. - Very selective COX-1 inhibitor ? highest incidence of side effects, five times more gastrotoxic than other NSAIDs. |
|
Image:
3 (binary/octet-stream)
|
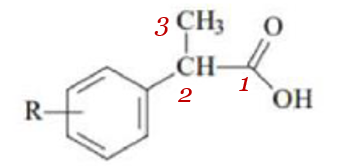
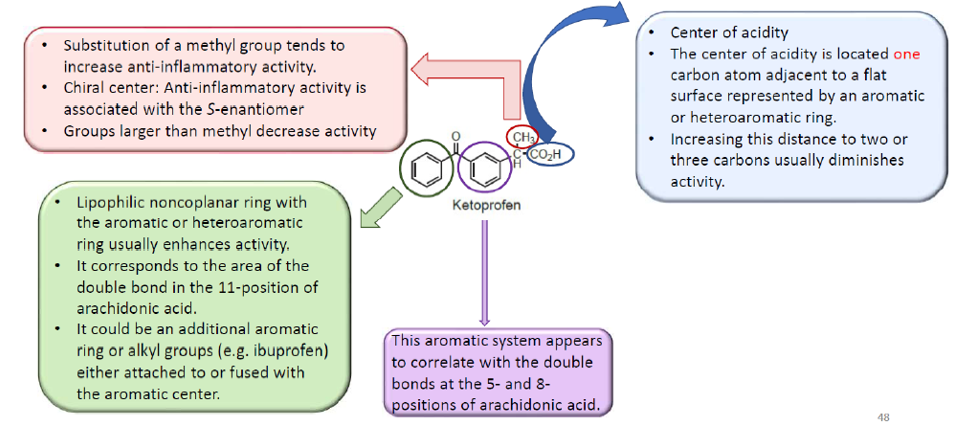
General Structure of aryl propionic acids • The α-CH3 substituent present in the profens (branching) increases cyclooxygenase inhibitory activity and reduces toxicity. • The α-carbon is chiral, and S-enantiomer is the more potent COX inhibitor. • Most profen products, except naproxen, are marketed as racemates. |
| What is the SAR of aryl propionic acids? |
Image:
4 (binary/octet-stream)
|
| What are the characteristics of aryl propionic acid drugs? | - Anti-inflammatory agents with analgesic and antipyretic activity. - Naproxen is considered to be the preferred non-selective NSAID for patients with high risk of cardiovascular disease. - All metabolites of ibuprofen are inactive. - Exception: oxaprozin ? The substitution of the propionic moiety is at position 3 rather than position 2 as in other agents. ? Prolonged DOA. ? Has uricosuric properties + used in the treatment of gout |
|
Image:
5 (binary/octet-stream)
|
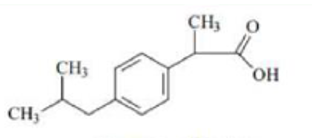
Ibuprofen - Aryl propionic acid derivative - All metabolites are inactive |
|
Image:
6 (binary/octet-stream)
|
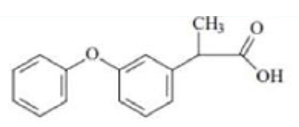
Fenoprofen - Aryl propionic acid derivative - Hint in naming: (how to differentiate between fenoprofen and ketoprofen ? ketoprofen has a ketone between the 2 rings; fenoprofen is an ETHER (only O between the 2 rings)) |
|
Image:
7 (binary/octet-stream)
|
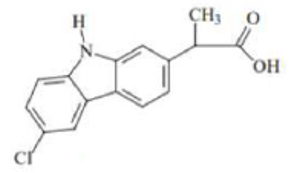
Carprofen Aryl propionic acid derivative |
|
Image:
8 (binary/octet-stream)
|
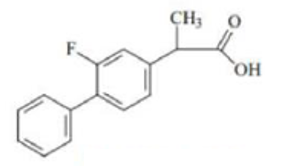
Furbiprofen Aryl propionic acid derivative |
|
Image:
9 (binary/octet-stream)
|
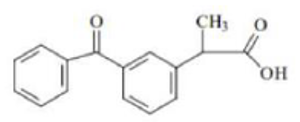
Ketoprofen Aryl propionic acid derivative |
|
Image:
10 (binary/octet-stream)
|
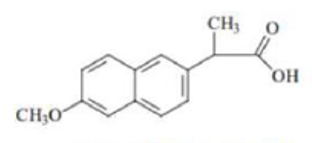
Naproxen - Aryl propionic acid derivative - Hint in naming: has a substituted naphthalene moiety - Preferred non-selective NSAID for patients with high risk of cardiovascular disease |
|
Image:
11 (binary/octet-stream)
|
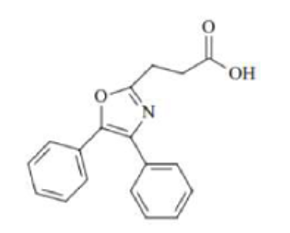
Oxaprozin - Aryl propionic acid derivative - Exception - Substitution of the propionic moiety is at position 3 rather than position 2 as in - Prolonged DOA - Has uricosuric properties + used in the treatment of gout |
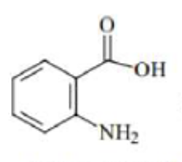
| What are Anthranilic acid derivatives? What drugs belong to this class of NSAIDs? | - N-aryl substituted derivatives of anthranilic acid, a bio-isostere of salicylic acid. - Retain the acidic properties characteristic of this class of agents. - Particularly, Fenamates are derivatives of N-phenyl anthranilic acid (Fen ~ phenyl) - REMINDER: Diclofenac (Voltaren) has structural characteristics of both aryl acetic acids AND anthranilic acids) - Drugs: meclofenamate, mefenamic acid |
|
Image:
12 (binary/octet-stream)
|
Anthranilic Acid |
|
Image:
13 (binary/octet-stream)
|
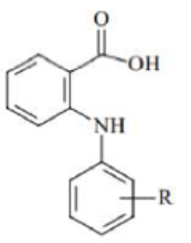
General Structure of Fenamates (N-phenyl Anthranilic Acids) |
| What is the SAR of Anthranilic acid derivatives? | - Small alkyl or halogen substituents at the 2’, 3’ and/or 6’ position of the N-aryl moiety increase activity. - E.g., meclofenamate is 25 times more potent than mefenamate. - 2’,3’ positions force the N-aryl ring out of coplanarity with the anthranilic acid. |
|
Image:
14 (binary/octet-stream)
|
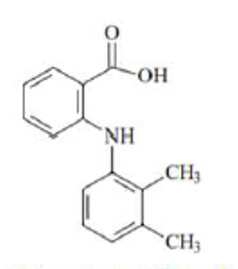
Mefenamic acid Anthranilic acid derivative |
|
Image:
15 (binary/octet-stream)
|
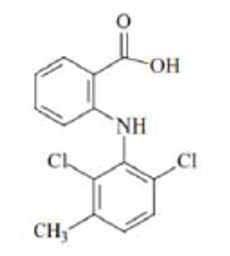
Meclofenamate - Anthranilic acid - 25 times more potent than mefenamate |
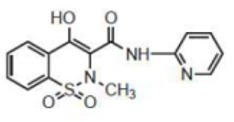
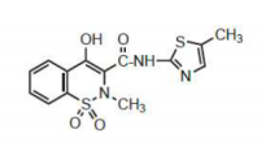
| What are the properties of Oxicams and what drugs belong to this class of NSAIDs? | - Drugs: Piroxicam and meloxicam; 4-hydroxy-1,2-benzothiazine carboxamide. (carboxamide = amide) - Their acidity is attributed to the 4-OH. - Optimal activity is obtained with methylamino and 2-pyridinyl groups. - Selectivity towards COX-2 over COX-1 is obtained with thiazole (as in meloxicam). - These compounds (pKa=6.3) are less acidic than carboxylic acid NSAIDs ? less GI side effects. - Long half-life - All piroxicam metabolites are inactive |
|
Image:
16 (binary/octet-stream)
|
Piroxicam - Oxicam derivative - All metabolites are inactive |
|
Image:
77 (binary/octet-stream)
|
Meloxicam Oxicam derivative |
|
Image:
18 (binary/octet-stream)
|
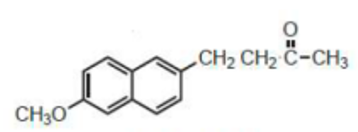
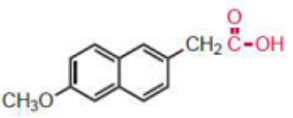
Nabumetone - Napthylalkanone derivative - Represents a new class of non-acidic prodrugs ? low incidence of GI side effects. - Prodrug, rapidly metabolized after absorption to form a major active metabolite, 6-methoxynaphthalene acetic acid. - Cl, CH3S, CHF2O at position 6 ? retains activity - Replacement of carbonyl group by CHO, CH2OH, COOCH3 ? retains activity |
|
Image:
19 (binary/octet-stream)
|
6-Methoxynaphtalene acetic acid - Napthylalkanone derivative - Active metabolite of Nabumetone |
| When is COX-2 expressed? | • COX-2 expression is induced by inflammatory cytokines, e.g., interleukins and tumor necrosis factor α (TNF- α). • Selective inhibition of COX-2 reduces the inflammation but does not interfere with the GI protective functions of COX-1. |
| Which classes of drugs are selective COX-2 inhibitors? | - Sulids - Coxibs |
|
Image:
20 (binary/octet-stream)
|
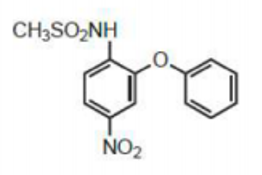
Nimesulide - Sulids derivative - Has a nitrobenzene, phenoxy and methyl sulfonamide group. - The methyl sulfonamide group is responsible for the greater selectivity towards COX-2 than COX-1. - No room for the methyl sulfonamide group in the active side pocket of COX-1, but it fits well in the active site of COX-2. - Metabolized to 4’-hydroxynimesulide which is biologically active. |
|
Image:
21 (binary/octet-stream)
|
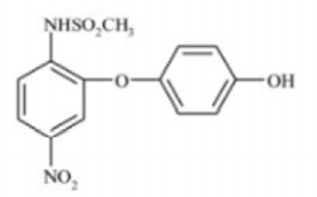
4’-hydroxynimesulide - Biologically active metabolite of Nimesulide |
|
Image:
23 (binary/octet-stream)
|
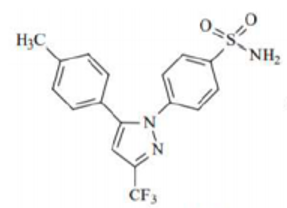
Celecoxib - Coxib derivative - Has a central pyrazole ring and two adjacent phenyl substituents, one containing a methyl group and the other a polar sulfonamide moiety; the sulfonamide binds to a distinct hydrophilic region on COX-2 but not on COX-1. - All metabolites are inactive. |
|
Image:
24 (binary/octet-stream)
|
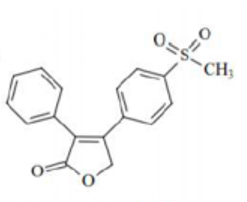
Rofecoxib - Coxib derivative - Has a central furanone ring and two adjacent phenyl substituents, one containing a methyl sulfone group, unlike celecoxib. |
|
Image:
25 (binary/octet-stream)
|
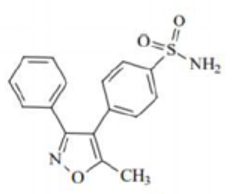
Valdecoxib - Coxib derivative - Has a central isoxazole ring and one phenyl ring with a polar sulfonamide like celecoxib. |
| What are the side effects of Coxib derivatives? | • Compared to nonselective NSAIDs, celecoxib is gastroprotective in the short term (6 months) but not in the long term (at 12 months) and causes clinically significant upper GI events. • Potential for severe cardiovascular effects: they suppress the formation of PGI2, which can result in elevated blood pressure and accelerated atherogenesis and predispose patients on coxib therapy to a heightened thrombotic response on the rupture of an atherosclerotic plaque. Valdecoxib and Rofecoxib were withdrawn from the market because of that. |
| What is the pathogenesis of Rheumatoid Arthritis? | • RA is an autoimmune disease. • Proteins containing citrulline are identified as foreign antigens by the immune system ? activation of T cells and B cells ? anti-citrulline inflammatory response that affects the joints ? swelling and degradation of both cartilage and bone. • Inflammatory cytokines TNF-α and IL-1 and 6 drive the destructive process in RA. |
| How can we treat RA? | • Anti-inflammatory drugs such as NSAIDs and glucocorticoids are used as adjunct therapy (NSAIDs show no sign in preventing or inhibiting the underlying pathogenic chronic inflammatory process) • Disease-modifying antirheumatic drugs (DMARDs) are used in the early stages of treatment to preserve joint integrity and function. - They limit joint damage and the progression of early rheumatoid arthritis but have no anti-inflammatory or analgesic effects. - Taken for as along as 3 months for clinical benefits. - Can be biologic or synthetic ? Biologic DMARDs target and inactivate cell proteins (cytokines) and T-lymphocytes (T cells), preventing them from causing inflammation. |
| What do synthetic DMARDs include? | 1. Gold salts: Aurothioglucose, sodium aurothiomalate, auranofin 2. Aminoquinolines: chloroquine and hydroxychloroquine 3. Immunosuppressants: methotrexate, leflunomide, sulfasalazine and Tofacitinib (Kinase inhibitor) |
| What are the properties of Gold compounds and which drugs belong to this class? | • Synthetic DMARDs • Examples: Auranofin, Aurothioglucose, Sodium Aurothiomalate • MOA: gold alters the morphology and functional capabilities of human macrophages, inhibiting the production of some interleukins. • High risk of side effects (55% of patients): dermatitis and mouth sores. • In case of toxicity, excretion of gold can be enhanced by chelating agents e.g., dimercaprol (also called British anti-Lewisite or BAL) and penicillamine. • High levels of gold persist for at least 20 days after the injection. |
|
Image:
1 (binary/octet-stream)
|
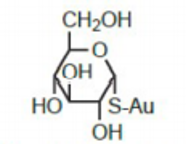
Aurothioglucose • Gold compound • Decomposes in aqueous solution after longstanding • Administered IM as a suspension in sesame oil. • Highly bound to plasma proteins. |
|
Image:
2 (binary/octet-stream)
|
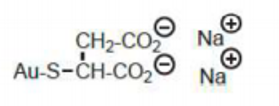
Sodium aurothiomalate • Gold compound • Is effective in slowing the development of progressive joint diseases. • Not active orally, administered by IM injection. • Water soluble. • Highly bound to plasma proteins. |
|
Image:
3 (binary/octet-stream)
|
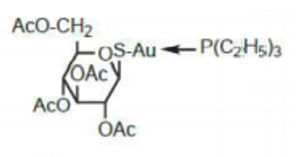
Auranofin • Gold compound • First orally effective gold compound for arthritis. • Complexation with triethylphospine enhances oral bioavailability. • Repurposed as a potential antimicrobial agent mainly against many Gram +ve bacteria, including multidrug resistant strains. |
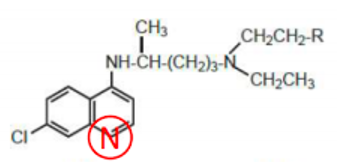
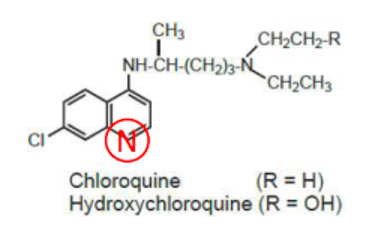
| What are the characteristics of Aminoquinolines and which 2 drugs belong to this class of drugs? | • Synthetic DMARDs • 4-aminoquinolines are originally known as anti-malarial drugs but they also showed efficacy in the treatment of RA. • Chloroquine: renal and corneal toxicity limits its use. • Hydroxychloroquine is less toxic but less effective as antirheumatic. • Hydroxychloroquine sulfate: oral and water soluble. |
|
Image:
5 (binary/octet-stream)
|
Image:
4 (binary/octet-stream)
|
|
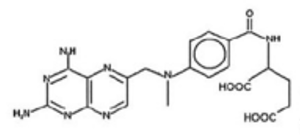
Image:
6 (binary/octet-stream)
|
Methotrexate • Synthetic DMARD: Immunosuppressant • MOA: causes in increase in adenosine ? adenosine causes potent anti-inflammatory effects, including a reduction in the number of activated T-cells and TNF-α levels. • Oral, food can delay absorption. • Metabolized to active metabolites, methotrexate polyglutamates and 7-hydroxy methotrexate. |
|
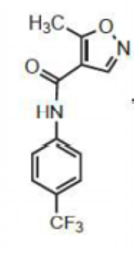
Image:
7 (binary/octet-stream)
|
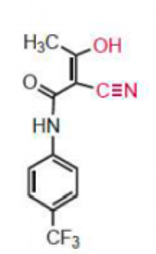
Leflunomide • Synthetic DMARD: Immunosuppressant • Oral administration • Prodrug: rapidly metabolized to teriflunomide, an active α-cyanoenol metabolite. • The C3-H of the isoxazole ring is required for ring opening. • Teriflunomide inhibits pyrimidine de novo synthesis by inhibiting dihydroorotate dehydrogenase ? decrease B-cell and T-cell proliferation, blocking the synthesis of immunosuppressive cytokines. • Undergoes primarily enterohepatic circulation, extending its DOA. |
|
Image:
8 (binary/octet-stream)
|
Teriflunomide Active metabolite of Leflunomide |
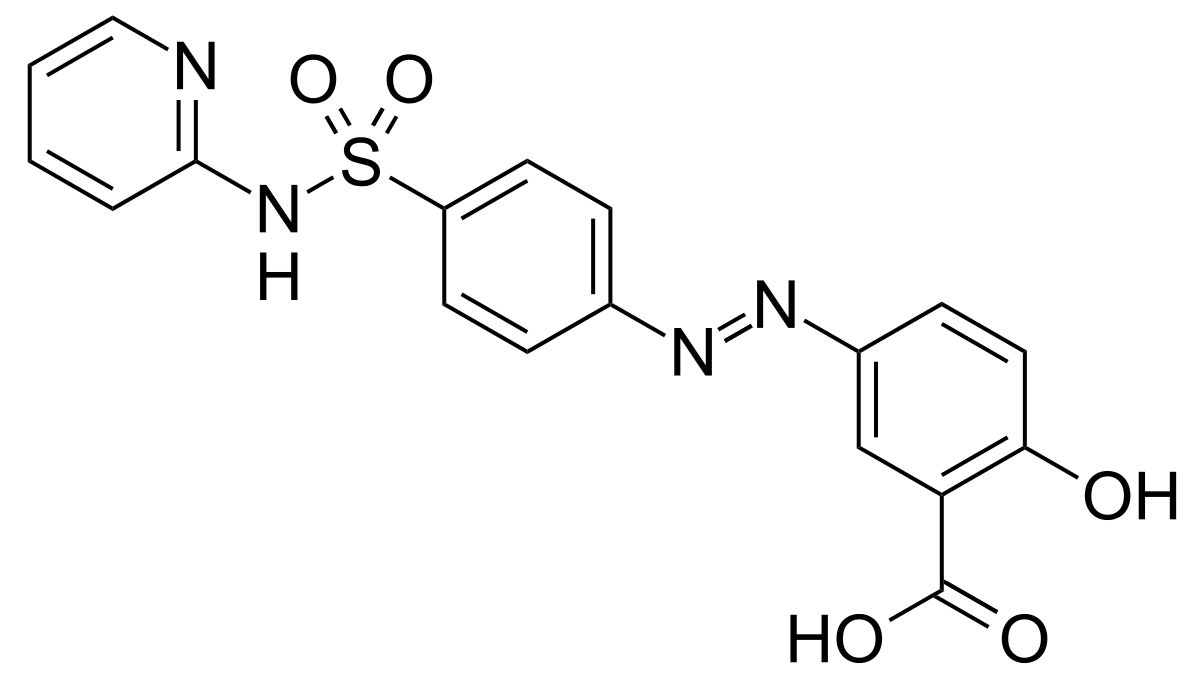
| Sulfasalazine • Synthetic DMARD: Immunosuppressant • Prodrug: hydrolyzed by colonic bacteria to 5-aminosalicylic acid (5-ASA; mesalamine) and sulfapyridine. • 5-aminosalicylic acid is an inhibitor of PG biosynthesis and also inhibits the release of inflammatory cytokines and TNF-α. • Inhibits lipoxygenase. • Used to treat colon inflammation as in Crohn’s disease. | |
|
Image:
9 (binary/octet-stream)
|
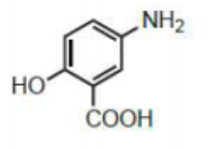
5-amino salicylic acid (mesalamine) Active metabolite of sulfasalazine |
|
Image:
10 (binary/octet-stream)
|
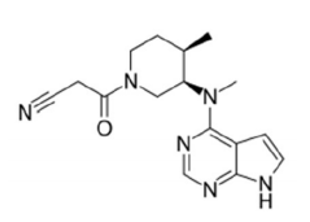
Tofacitinib • Synthetic DMARD: Immunosuppressant • Orally active • Specifically inhibits JAK3, blocking proinflammatory cytokine signaling which prevents the expression of both B and T cells. • For the treatment of adults with active RA who had inadequate response to, or who are intolerant to methotrexate. |
| What are the different types of biologic DMARDs? | • Cytokine inhibitors • Rituximab: monoclonal antibody that targets B-lymphocytes • Interleukin-1 receptor antagonist • IL-6 antagonist • Stimulation modulators Biologic DMARDs are associated with high risks of infections |
| What are the two different approaches used to decrease TNF activity? | 1. Administration of soluble TNF receptors (TNFRs; etanercept) 2. Treatment with anti TNF-α antibodies (e.g., infliximab, adalimumab, certolizumab); they neutralize the effects of TNF ? reduce the symptoms of RA within 1 or 2 weeks and slow the progression of the disease. Synergistic with methotrexate and are often taken with it. |
| Rituximab | • Monoclonal antibody that targets B-lymphocytes. • Originally used to treat non-Hodgkin lymphoma. • Also used in chronic lymphocytic leukemia. • Increasingly prescribed for the ttt of autoimmune diseases, including RA. |
| Interleukin-1 receptor antagonist | • IL-1 production is triggered by inflammatory stimuli. • Its binding to IL-1 type 1 receptor (IL-1R1) increases the formation of nitric oxide (PGE2) and collagenase in synovial cells, resulting in cartilage degradation and bone resorption. • The levels of the naturally occurring IL-1 receptor antagonist (IL-1Rα) in the synovium and synovial fluid from RA patients are insufficient to compete with the elevated amount of locally produced IL-1. • Anakinra is a recombinant form of IL-1Rα that prevents the binding of IL-1 to its IL-1R1, decreasing the inflammatory process. |
| Anakinra | Recombinant form of IL-1Rα that prevents the binding of IL-1 to its IL-1R1, decreasing the inflammatory process. |
| IL-6 antagonist | Tocilizumab • Recombinant anti-human IL-6 receptor monoclonal antibody that bonds to both soluble and membrane-bound IL-6 receptors, inhibiting IL-6 mediated signaling. • Shown to have slightly higher efficacy than methotrexate, but a slightly higher incidence of side effects. |
| Tocilizumab | IL-6 antagonist |
| T-cell Co-stimulation blockers | Abatacept • It is the first in a new class of immunosuppressants. • Prevents the generation of positive co-stimulation signals and stimulation of T-cell activation ? suppresses the proliferation of reactive T-cells and the release of more cytokines that destroy tissue ? reduce the symptoms of arthritis. |
| Abatacept | T-cell Co-stimulation blockers |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.