33216743
Description
| Question | Answer |
| Identify the Autoimmune Disease: Steroid hormones produced by the adrenal cortex are low or absent | Addison's Disease |
| Which steroid hormone impaired by Addison's Disease is responsible for regulating blood volume and pressure by maintaining sodium and water balance | Aldosterone (mineralocorticoid) |
| What is the role of the cortisol (glucocorticoid) hormone produced by the adrenal cortex | Maintaining BGL, reducing inflammation, and regulating water balance |
| One or both steroid hormones are produced but the body is unable to use them Does the above statement describe primary or secondary adrenal insufficiency? | Secondary |
| Which of the following is an example of "breath malodour?" a) Morning breath b) Bad breath caused by garlic c) Bad breath caused by smoking d) Bad breath caused by medication e) None of the above | e) None of the above By definition, breath malodour is both persistent and caused by some pathology |
| What might a patient suffering pseudo-halitosis experience? | The belief that they have oral malodour despite no malodour being present |
| Which of the following is NOT a source of halitosis a) Tonsils b) Microbial activity/high bacterial loads c) Tumours d) Blood-gas exchange e) Saliva f) Ulcerations g) Gingival Crevicular Fluid h) Plaque i) Granulomas j) Sinusitis | i) Granulomas |
| Complete the following A possible source of intra-oral halitosis can be the direct result of ________ activity attributed to gram ______ a________ flora producing volatile ________ compounds (VSCs) | A possible source of intra-oral halitosis can be the direct result of MICROBIAL activity attributed to gram NEGATIVE aNAEROBIC flora producing volatile SULPHUR compounds (VSCs) |
| Name the two primary halitosis-associated VSCs and the odour they produce | 1. Hydrogen Sulphide (H2S) - Rotten egg odour 2. Methyl Mercaptan (CH3SH) - Faeces odour |
| Name a systemic disease associated with malodour and the compound that these patients may exhale | Example from Lecture: Diabetes (when uncontrolled) can result in the release of ketones during blood-gas exchange and may produce a sweet smell |
| Which surface of the tongue is a primary source for bacteria accumulation? | Dorsum, especially posterior region |
| What role do VSCs play in the progression of periodontitis? | - Increases permeability of the mucosa and allows addition bacteria and endotoxins to invade - Assist lipopolysaccharides in penetrating healthy epithelium - Impedes wound healing by interfering with collagen, protein, and DNA synthesis |
| Complete the following: Research suggests an increase in perio disease severity when the ratio of ____ ______ exceeds that of hydrogen sulphide | Methyl mercaptan |
| True or False Hepatic conditions are associated with the production of methyl mercaptan (rotten egg) odours | False Hepatic conditions produce sulphur (rotten egg) odours |
| Which of the following is NOT a respiratory condition associated with halitosis? a) Lung abscesses b) Lung resection c) Lodged foreign bodies d) Pneumonia e) Pulmonary cancer f) Tuberculosis | b) Lung resection |
| What is the name given to the spread of bacteria to the tongue from the sinus during a sinus infection? | Postnasal drip |
| How can nasal-originating halitosis be distinguished from oral-originating halitosis? | If halitosis is produced by a nasal source, the odour will emanate from the nose when the mouth is closed |
| Which systemic disease can produce an ammonia odour which emanates from the oral cavity? | Renal failure |
| Name three examination/detection devices used in the diagnosis of halitosis | 1. The nose 2. Organoleptic judges (specialised individuals) 3. Gas chromatography (lab-based procedure that assesses VSC presence) 4. Microbiological assay (evaluates specific sites for VSC/bacterial byproducts) 5. Sulphide-detection devices (portable monitors to detect VSCs, more sensitive to hydrogen sulphide) |
| Which of the following is a disadvantage of gas chromatography? 1. Inaccuracy 2. Cost 3. Patient compliance 4. Inability to detect more complex causes of halitosis (e.g. nasal, respiratory) | 2. Cost |
| In the categorisation of halitosis, which category is described below? Odour is detectable, although the examiner could not recognise it as halitosis | 1. Questionable Halitosis |
| Name the rapid chair-side detection tool used to detect halitosis through samples of plaque from the dorsum of the tongue | BANA-zyme Benzoyl-DL-arginine-naphthylamide (BANA) |
| Which ingredients may aid in the management of halitosis when incorporated in chewing gum? | - Zinc citrate - Sodium bicarbonate - Eucalyptus - Probiotics Xylitol may also help to increase salivary flow |
| True or False Regular tongue cleaning with a tongue scraper has proven to be more effective at halitosis reduction than CHx and mechanical oral hygiene | False CHx and mechanical oral hygiene reduce bad breath for longer periods than tongue cleaning alone |
| In the following list of halitosis-managing chemotherapeutics, which has been REMOVED for being a possible carcinogen? 1. Chloride dioxide 2. Zinc 3. Chlorhexidine 4. Triclosan 5. Essential oils 6. Cetylpyridinium chloride (CPC) | 4. Triclosan |
| Explain the role of zinc in neutralising VSCs | Zinc ions have a strong affinity to thiol groups present in VSCs, converting them to non-volatile sulphides |
| True or False Acidic saliva is associated with halitosis | False Alkaline saliva is associated with halitosis |
| Which metal is most commonly used in the implant bodies? | Titanium |
| What is the name given to the part of the implant which acts as an interface between the crown and implant body? | Abutment (Can be made from aesthetic materials or titanium) |
| Name three implant abutments which may be used to support full dentures | 1. Ball anchor abutment 2. Magnetic abutments 3. Bar retainers (attaches to retaining clips on denture) |
| Which tool is used to deliver sterile solution to the bone during implant preparation surgery? | Fisiodispenser This tool functions to cool down the bur and the bone. Care must be taken not to overheat the bone as it may become necrotic |
| Pictured is a handpiece connector, used in implant surgery. What is it used for? | Transportation of the implant from sterile casing to the implant site |
| A patient presents to the clinic requiring an implant. After assessing the patient you notice that their bone quality is poor and the buccal bone is thin, and the bone height is sufficient. Which approach do you take? a) One-step implant (immediate placement) b) Two-step implant (delayed placement) c) Advise the patient that they are not suited for implants and invite them to consider dentures | b) Two-step implant (delayed placement) The quality and amount of bone is an important factor in deciding between one and two step implant placement |
| Roughly how long does healing take following implant placement in a delayed placement procedure? | 6 months It should occur in an environment where bacteria cannot penetrate i.e. the soft tissue is healed |
| Which material may be chosen for an implant abutment as an aesthetic alternative to titanium? | Zirconia |
| True or False When a patient surpasses roughly 60 years of age, osteoblast activity diminishes so significantly that the osseointegration required for implant placement becomes unattainable | False There is no cut-off age for implants, however the poor dexterity and higher rates of comorbidities associated with ageing results in a higher rate of implant failure |
| True or False Unresolved caries is considered a risk factor for implant failure | True |
| What are the advantages of selecting delayed (12-16 weeks) implant placement | - Substantial bone fill of the socket facilitates implant placement - Mature soft tissues facilitate flap management |
| In early implant placement, how long after extraction is the implant placed? What are the advantages and disadvantages of this? | 4-8 weeks Advantages: - Increased soft tissue area and volume - Resolution of local pathology can be assessed Disadvantages: - Site morphology may complicate optimal placement and anchorage - Treatment time increased - Socket walls exhibit varying amounts of resorption - Adjunctive surgical procedures may be required - Procedure is technique-sensitive |
| If a clinically healed ridge is required, how long should the tissue be left to heal before the implant is placed? | 16+ weeks (Late placement) |
| What are the major histological differences between implant and natural-tooth attachment? | - Implants have no PDL-cementum interface for attachment and require ankylotic attachment - Soft tissue surrounding implants is more fibrous and contains less cells (scar tissue) - Gingival fibres surrounding implant are oriented parallel to the implant and do not attach to the implant body |
| Identify two biocompatible materials implant bodies can be made of | - Ceramic - Titanium or titanium alloys |
| Implant surfaces are moderately rough (1um-2um usually) with additional micro-roughness created for retention How is this "micro-roughness" created? | Acid etched, sand blasted, or nano-modified |
| Which feature of the implant creates primary stabilisation before osseointegration is achieved? | The threads Overtime the gap between the implant and the bone is filled by bone remodelling until the bone comes into contact with the implant |
| Which of the following is NOT a risk factor for implant failure? 1. Autoimmune diseases (e.g. HIV) 2. Uncontrolled diabetes 3. Eccentric loading 4. Unresolved caries 5. Fixed partial denture with more than two implants | 5. Fixed partial denture with more than two implants |
| Which of the following does NOT affect the success of osseointegration? a) Implant material b) Micro-surface topography c) Soft tissue integrity d) Systemic diseases | c) Soft tissue integrity |
| Which of the following statements are FALSE regarding dental implants? a) A "biological seal" unites two objects with no gaps for the entry of foreign materials b) The mucosal tunnel should usually be shallow c) The junctional epithelium is incapable of attaching to the abutment as it would on a natural tooth d) Connective tissue fibres cannot encircle the implant, however they can encircle a natural tooth e) The implant should not be probed until 6-8 weeks after placement | c) The junctional epithelium is incapable of attaching to the abutment as it would on a natural tooth The junctional epithelium (JE) CAN attach to the abutment, this is how/where the biological seal is formed. While the JE can attach to the abutment, the gingival fibres cannot |
| Name the 3 gingival fibres not present around an implant | 1. Circular (encircles tooth) 2. Dentogingival (tooth to gingiva) 3. Transeptal (tooth to tooth) Only the gingival fibres which attach bone to gingiva and are oriented parallel to the implant remain (i.e. dentoperiosteal, alveologingival) |
| True or False Osseointegration can be deemed unsuccessful if that patient experiences soft tissue inflammation around the implant site | True Successful osseointegration relies on the absence of mobility, pain, discomfort, increased radiographic radiolucency, and inflammation of the peri-implant tissues. |
| True or False Following implant placement, patients should ensure they select a chlorhexidine rinse with NO alcohol | True |
| Following implant placement, when should sutures be removed? | After 2-3 weeks and with topical anaesthetic |
| When should the healing of an implant be assessed after surgery? | After 3 weeks Changes to monitor include tissue condition/colour, presence of suppuration, inflammation, bleeding, plaque, calculus etc |
| Which of the following statements correctly describe the probing of an implant? a) Use plastic or teflon-coated instruments and a probing force of 0.25N b) Use rubber or teflon-coated instruments and a probing force of 0.75N c) Use plastic or teflon-coated instruments and a probing force of 0.05N | a) Use plastic or teflon-coated instruments and a probing force of 0.25N |
| Which implant material is known for being soft and susceptible to scratches? | Titanium |
| True or False The use of metal probes around an implant are known to scratch the implant body | False The use of plastic probes is a priori, and no existing studies confirm that regular probes can compromise the implant integrity |
| During the "initial bone remodelling" phase occurring in the first year after implant placement, how can pathological bone loss be distinguished from naturally occurring bone loss? | Bone loss which reaches or exceeds 2mm is considered pathological. The threads may also be seen detached from the bone. Bone loss of <2mm within the initial bone remodelling phase, however, is considered normal. |
| When should a baseline PA be taken of an implant to identify future pathological bone loss? | 1 year after placement (after the initial bone remodelling period) |
| Which part of a dental implant may be negatively affected by mouthwash? | The abutment surface |
| Identify the main disadvantage of plastic scalers for implant debridement when compared to titanium scalers | Particles of plastic curettes may break off and remain on the implant surface where it can impede healing. Additionally they are bulky, and the tips, while replaceable, are single use |
| Either prophylaxis or air-powder polishers are used up to 1mm into the sulcus to maintain peri-implant health. Identify the powder described below - Natural sugar substitute present in some fruits and fermented food - Contains 0.3% CHX - Suitable for patients on low salt diet (no salt) - Grain size ~14um | Erythritol Alternatively, Glycine may be used subgingivally with a grain size ~25um, a sweet taste (no sugar), and low abrasiveness. |
| True or False Peri-Implant Mucositis may be associated with an increased PPD | True Despite not involving ANY bone loss, peri-implant mucositis can still increase pocket depth due to the swelling and reduced resistance of soft tissue |
| True or False Probing depths around implants a bit deeper than that of a natural tooth are to be expected, however, patients presenting with measurements ≥6mm can be diagnosed with peri-implantitis | False PPD ≥6mm are considered in the diagnosis of peri-implantitis, however these readings can still be found in healthy implants and are not reliable on their own. |
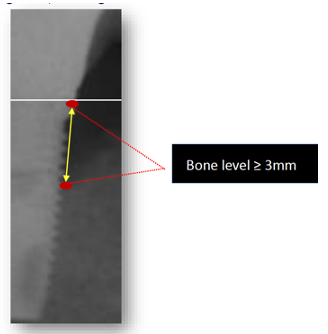
| Explain how peri-implantitis is diagnosed radiographically | Diagnosis can be achieved if 3 or more threads are outside the bone, OR the bone level presents ≥3mm apical to the most coronal part of the intraosseous part of the implant (see image) |
| True or False Active peri-implantitis often lacks clinical signs of inflammation and does not become apparent until examined radiographically | False Active peri-implantitis always presents with BOP, increased PPD, and suppuration |
| Which statement regarding the histopathology of peri-implantitis is FALSE? 1. Peri-implantitis lesions exhibit higher infiltrations of PMNs, macrophages, plasma cells, and lymphocytes 2. Peri-implantitis is self limiting due to the host immune response 3. Peri-implantitis lesions are more than twice as large as periodontitis lesions 4. Peri-implantitis lesions are circumferential | 2. Peri-implantitis is self limiting due to the host immune response While this IS the case for periodontitis, peri-implantitis do not have the same "self-limiting" feature and thus extend rapidly apically |
| True or False Implants are naturally more susceptible to infection than natural teeth, and thus require less microbially-complex biofilms to result in peri-implantitis | False Peri-implantitis is a poly-microbial anaerobic infection, more complex than periodontitis and more difficult to treat |
| Which bacteria are associated with implant health? | Coccoid gram positive bacteria |
| Name two bacteria associated with peri-implantitis | 1. Prevotelaceas 2. P.gingivalis 3. F.nucleatum 4. T.forsythia 5. T.denticola |
| Define Peri-Apical Peri-Implantitis (aka Retrograde Peri-Implantitis) and identify its common cause | Peri-apical radiolucency surrounding the implant without clinical signs of inflammation Usually caused by an existing peri-apical condition at the site either from the tooth extracted for the implant or from a neighbouring tooth |
| Which system of the body is affected by Guillain-Barre syndrome? | The nervous system |
| Which autoimmune condition may be associated with a melanin-pigmentation of or "bronzing" of the skin and mucosa? (pictured) | Addison's Disease |
| Name the gland responsible for metabolic processes e.g. growth, energy expenditure | The Thyroid Gland |
| True or False Graves' Disease is characterised by a chronically under-active thyroid gland | False Graves' Disease involves antibodies intended to interfere with thyroid cell receptors activating the cell instead. The receptors targeted by antibodies in Graves' Disease are TSH receptors. |
| Name 5 symptoms of hyperthyroidism | - Goitre - Trouble sleeping - Irritability/nervousness - Heat sensitivity, increased sweating - Hand tremors - Rapid heartbeat - Thinning of skin or brittle hair - Frequent bowel movements - Weight loss without dieting - Fatigue or muscle weakness - Lighter menstrual flow and less frequent periods - Problems getting pregnant - Swelling and inflammation of the eyes |
| Identify the autoimmune condition most commonly associated with hypothyroidism | Hashimoto's Thyroiditis aka chronic lymphocytic thyroiditis OR autoimmune thyroiditis |
| Name 5 symptoms of hypothyroidism | - Fatigue/muscle weakness - Increased cold sensitivity, pale, dry skin - Retained fluid, unexplained weight gain, puffy face - Constipation - Hoarse voice - Muscle aches, tenderness, and stiffness - Pain and stiffness in joints - Swelling in knees or the small joints of the hands and feet - Excessive or prolonged menstrual bleeding (menorrhagia) - Depression - Delayed dental eruption - Macroglossia, glossitis |
| What challenges do anti-thyroid drugs such as propylthiouracil (PTU) pose in a dental setting? | The anti vitamin-K properties of these medications can cause hypoprothrombinaemia and bleeding that poses a risk for haemorrhage. Hyperthyroid patients in general can be expected to exhibit longer bleeding times, especially if their arteriolar blood pressure is high |
| True or False Due to the impairment of wound healing from decreased metabolic activity in fibroblasts, hypothyroid patients are considered immunocompromised | False Hypothyroid patients may have delayed wound healing for these reasons, but are NOT considered immunocompromised |
| Which of the following is associated with longer bleeding times? a) Hyperthyroidism b) Hypothyroidism c) Both | c) Both Hypothyroid patients may bleed longer due to accumulation of subcutaneous mucopolysaccharides which impairs blood vessel constriction. This can also cause haemostasis and other cardiovascular diseases due to arteriosclerosis. Hyperthyroid patients, however, experience increased bleeding due to their elevated blood pressure and medications |
| Match each of the following descriptions to either HYPERTHYROIDISM or HYPOTHYROIDISM a) Salivary gland enlargement b) Maxillary and mandibular osteoporosis c) Increased susceptibility to caries d) Accelerated dental eruption e) Glossitis | a) HYPOthyroidism b) HYPERthyroidism c) HYPERthyroidism d) HYPERthyroidism e) HYPOthyroidism |
| Identify the Autoimmune Disease Considered to be a T-cell mediated disease that affects the central nervous system (CNS) | Multiple Sclerosis (MS) |
| Which part of the nerve is affected by multiple sclerosis, often by deteriorating, being lost (MS plaques), and being replaced with scar tissue (sclerosis). | The myelin sheath |
| How long does a multiple sclerosis "attack" usually last for? | Days to weeks These attacks can be several years apart, usually worsening in physical impairment each time |
| Identify the autoimmune disease Chronically inflamed synovium, densely crowded with lymphocytes, resulting in destruction of cartilage and bone. Characterised by periods of exacerbations and remissions. Pain is symmetrical and migratory and may present alongside anaemia or a low grade fever. | Rheumatoid Arthritis |
| Identify the Autoimmune Disease Neuromuscular disease wherein antibodies activate the acetylcholine receptor which blocks the reception of nerve impulses. | Myasthenia Gravis |
| Identify the Autoimmune Disease Characterised by weakness of symmetrical voluntary muscles, eye movement weakness with diplopia and ptosis (drooping eyelids), and in severe cases, total paralysis or serious breathing problems | Myasthenia Gravis |
| What occurs during a Myasthenic Crisis? How might it be managed? | A Myasthenic Crisis involves a deficiency of acetylcholine so great that it causes a sudden inability to swallow, speak, or maintain airway clearance. These attacks can be managed by suctioning, opening the airway, and calling for help |
| What oral manifestations may be seen in patients suffering myasthenia gravis? | - Increased salivation (anticholinesterase) - Gingival enlargement (cyclosporin) - Infection (immunosuppressive drugs) |
| Which of the following is NOT needed in the dental management of patients with myasthenia gravis? a) Antibiotic prophylaxis b) Short, frequent, early morning appointments c) Toothbrush modifications d) Stress reduction protocol e) Instructions to caregiver | a) Antibiotic prophylaxis |
| Identify the Autoimmune Disease Autoimmune disease complex in which lymphocytes attack and replace functional epithelium, primarily affecting exocrine glands | Sjogren's Syndrome |
| Which autoimmune disease is associated with ALL of the following - Keratoconjunctivitis - Xerostomia - Connective tissue disease | Sjogren's Syndrome |
| True or False Sjogren's Syndrome is characterised by a slow onset, and often goes undetected for years | True |
| Which viral infection is thought to cause Sjogren's Syndrome? Explain the mechanism for this | Exposure to or reactivation of Epstein-Barr virus (EBV) This triggers the activation of human lymphocyte antigen (HLA) complex, resulting in the release of cytokines (TNF, IL-2, interferon, IFN-y, etc) and in turn is followed by the infiltration of lymphocytes and destruction of the exocrine gland tissue. |
| Name 4 oral manifestations of Sjogren's Syndrome | 1. Hyposalivation 2. Glossitis 3. Mucositis 4. Partoid gland hypertrophy 5. Candidiasis 6. Angular cheilosis 7. Taste dysfunction 8. Secondary infection 9. Periodontitis 10. Increased caries rate |
| Describe the treatment of Sjogren's Syndrome | Treatment is palliative (treating pain without curing) and should focus primarily on the relief of dryness (oral and ocular) and burning/discomfort. This can be done by the stimulation or simulation of saliva, treatment of secondary mucosal conditions (e.g. mucositis), and prevention of oral disease. |
| Identify the Autoimmune Disease Autoimmune disease of connective tissue affecting the skin, intestine, kidneys, and sometimes lungs, caused by the accumulation of excessive collagen | Scleroderma |
| Identify the dental considerations for treating a patient with scleroderma | Clinicians should be wary of restricted mouth opening due to lip and skin rigidity, lack of dexterity, and greater sensitivity to cold, dampness, stress, and fatigue Extra-orally, the patient may also experience skin ulcers, immobility, and stiff joints |
| Identify the Autoimmune Disease Skin cells grow at abnormally fast rates causing lesions which appear as raised, red, scaly patches on the skin | Psoriasis |
| Identify the 5 types of Psoriasis | 1. Plaque psoriasis 2. Guttate 3. Inverse 4. Pustular 5. Erythrodermic (rare) |
| Name 3 symptoms of oral psoriasis | 1. Patches of red skin with yellow or white edges 2. Sores 3. Peeling of the gingiva 4. Pustules 5. Pain or burning, especially when eating spicy foods 6. Changes in how things taste 7. May be associated with other conditions e.g. fissured tongue, geographic tongue, inflamed gingiva |
| Identify the Autoimmune Disease Dangerous levels of anti-DNA antibodies are produced, attacking many organs and causing fever, joint pain, and damage to the CNS, heart and kidneys. | Systemic Lupus Erythematous (SLE) |
| How might systemic lupus erythematous (SLE) affect the kidneys? | Damage to the kidneys by SLE may lead to the leakage of protein (proteinuria) and haemorrhage (hematuria) |
| Systemic lupus erythematous (SLE) is linked to a genetic predisposition but exacerbated by environmental factors. Name 3 environmental factors which may exacerbate SLE | 1. Ultraviolet light 2. Hormones (10 times more frequent in women) 3. Drugs (may induce SLE-like symptoms) |
| A patient presents to the clinic with an unknown condition. During examination you notice they experience chest pain when taking deep breaths, swollen lymph nodes, fever, hair loss, and exhibit a "butterfly" rash across the cheeks Assuming these are all caused by the same condition, what is the most likely diagnosis for this patient? | Systemic Lupus Erythematous (SLE) |
| Name two autoimmune diseases which can be treated by non-steroidal anti-inflammatory medications (NSAIDS) | 1. Systemic Lupus Erythematous (SLE) (treats arthritis and pleurisy symptoms) 2. Rheumatoid Arthritis |
| How might a patient suffering SLE relieve symptoms of arthritis and skin rashes? | Hydroxychloroquine and low-dose corticosteroids can treat BOTH rashes and arthritis Additionally, NSAIDS can treat arthritis symptoms exclusively, and corticosteroid creams can be used on skin rashes |
| In more severe cases of SLE where corticosteroids prove ineffective, what medical alternatives may be used to block cell growth | Cytotoxic drugs |
| True or False In more severe cases of SLE, high doses of corticosteroids may be utilised to decrease immune response | True |
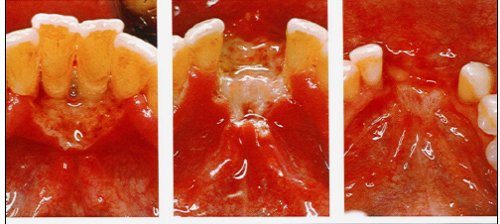
| Which autoimmune disease may be associated with keratotic, rough-surfaced plaque oral manifestations such as the one pictured? | Systemic Lupus Erythematous (SLE) Specifically, this image depicts a patient with discoid lupus erythematous |
| Identify the Autoimmune Disease based on the following oral manifestations - Delayed dental eruption - Reduced salivary flow - Recurrent aphthous stomatitis - Angular cheilitis - Dental enamel defects in both dentitions (poor enamel formation, pitting or banding of teeth, mottled or translucent-looking teeth) | Celiac Sprue Disease |
| True or False Crohn's Disease and Ulcerative Colitis involve BOTH autoimmune and immune-mediated phenomena in the small intestine | True |
| A patient presents to the clinic with an inflammatory bowel disease, but is unsure of whether they have Crohn's Disease or Ulcerative Colitis. You note that they exhibit a cobblestone appearance on the buccal mucosa, mucosal tags, and swollen lips. Which condition are they more likely to have? | Crohn's Disease Ulcerative colitis is characterised by apthous ulcers, dry mouth, and pyostamtitis vegetans |
| True or False Non-steroidal anti-inflammatory drugs (NSAIDS) can be prescribed to treat inflammatory bowel diseases | False NSAIDS can trigger flare-ups. Paracetamol is recommended instead, although this may have adverse effects |
| Which organ becomes inflamed in viral hepatitis? | The liver |
| In viral hepatitis, what action triggers the host immune response? | Replication of the virus in the liver The host immune response is also what causes most of the liver damage (cirrhosis) |
| Which form of Hepatitis is described below? Defective virus which requires Hepatitis B infection to exist, and can be prevented by the Hepatitis B vaccine | Hepatitis D |
| Name the types of Hepatitis transmitted through the faecal-oral route | Hepatitis A Hepatitis E All others are blood-blood transmission |
| Which type of Hepatitis is known for providing lifelong immunity and usually a fully recovery within months? | Hepatitis A However, symptoms may be quite debilitating while present |
| Which type of Hepatitis is known for symptomatically mimicking Hepatitis A but is found more commonly in Asia, Africa, and Central America, and does not have a vaccine available? | Hepatitis E |
| Which type of Hepatitis can be transmitted by bodily fluids, including saliva-blood? | Hepatitis B Hep B also includes blood-blood contamination. As such, it is the most common liver infection around the world |
| List the types of Hepatitis with available vaccines | Hepatitis B Hepatitis D (same vaccine) Hepatitis A Hepatitis E, while without a vaccine, is generally less of a threat as it tends to be acute. This is not the case for Hepatitis C, however. |
| How many Hepatitis C genotypes are thought to be in Australia? | 6 The most common of the 6 is type 1, and, to a lesser extent, type 3 Infection with multiple Hep C genotypes is possible |
| Name the type of Hepatitis described below: Antibodies produced do NOT provide immunity against this form of hepatitis, and reinfection can always occur, even after recovery | Hepatitis C |
| How might you expect the oral condition of a Hepatitis C patient to appear? | Hepatitis C patients usually exhibit a low salivary flow, especially if on antidepressants, and as such most of the oral manifestations are a result of this. These include: - Dental caries at higher rates - Altered taste - Burning mouth - Candidiasis - Halitosis - Difficulty chewing, swallowing, and talking - Difficulty wearing dentures - Dry lips |
| What two medications are known for being previously used in combination to treat Hepatitis C? | Pegylated Interferon injection + oral ribavirin These medications have varying success rates depending on genotype, are known for causing significant side effects over time, and are dose-dependent on viral load and liver fibrosis |
| True or False A person who has recovered from Hepatitis C but retains Hep C antibodies is still considered "Hepatitis C positive" | False Hep C status is determined only with an RNA test |
| What factor should be accounted for when selecting Hepatitis C medications | Virus genotype, determined by blood testing. Genotype (as well as presence of cirrhosis of the liver) also determines treatment duration |
| Complete the following Modern Hepatitis C medications can achieve a __% clearance rate. Treatment time ranges from __ to __ weeks, with the average time for geno type 1 treatment being __ weeks. | Modern Hepatitis C medications can achieve a 95% clearance rate. Treatment time ranges from 12 to 24 weeks, with the average time for geno type 1 treatment being 12 weeks. |
| Outline the correct procedure following a needle-stick injury with a Hep C positive patient | 1. Wash the source of the wound with soap and water (or alcohol rub if not available) 2. See a doctor immediately |
| True or False The interaction between Hepatitis C medications and LA are unknown | True Anti-viral medications rarely interfere with local anaesthetic as a whole, but a GP should still be consulted before treatment |
| Name a side effect of a modern Hepatitis C medication | - Significant fatigue, disturbed sleep - Nausea - Headaches |
| Explain briefly the role of CD4 cells and the effect HIV infection has on them | CD4 cells are helper T-cells which are regulators and effectors of the normal immune response Over time, attack from the HIV virus causes the CD4 cell count to decline and the immune function to become compromised. |
| A HIV positive patient presents to the clinic. Before treating them you ask about their last blood test and are told they had an "undetectable" viral load. What can you assume about their blood test results? | No virus could be detected in more than 20 copies/ml3 of blood |
| A HIV positive patient presents to the clinic and informs you they are taking retro-0viral medications. When you ask about their last blood test, you are told their T-cell count was 550. Should this patient be concerned about their current T-cell count? | No HIV patients taking retro-viral medications should aim to have a T-cell count above 500 consistently, as well as an undetectable viral load. |
| What is the main drawback of saliva-based HIV tests as opposed to blood tests? | Cost |
| How many genotypes of HIV are known to exist? | 2 HIV 1 and HIV 2 (HIV 1 also has 9 subtypes labelled A, B, C,..., I) |
| True or False A HIV positive patient who develops an opportunistic infection is thought to have progressed to A.I.D.S | True A HIV positive patient diagnosed with one or more AIDS-defining conditions is considered to have AIDS. These conditions include opportunistic infections as well as malignancy, wasting, and neurological disorders |
| List the recognised modes of transmission for HIV | 1. Unprotected sex 2. Re-using needles 3. Vertical transmission from mother to child However, mother-child transmission, needle-stick, tattooing, or medical procedure related transmission is uncommon in Australia |
| True or False HIV can be transmitted through saliva | False HIV is present in the saliva but is not considered a notable risk factor due to its low levels the inhibition of transmission by antiviral factors in saliva |
| Which of the following can transmit HIV? a) Tears b) Sweat c) Faeces d) Urine e) None of the above | e) None of the above |
| Statement 1: The risk of hepatitis C transmission from a needle-stick injury is extremely low Statement 2: The risk risk of HIV transmission from a needle-stick injury is extremely low | Both statements are true The risk of HIV transmission after subcutaneous exposure to HIV-infected blood is very small (0.3%), and even smaller if the patient's viral load is undetectable |
| At what T-cell count and viral load are oral manifestations from HIV most likely? | T-cell count <200 VL >3000 copies/ml3 |
| What type of infection is angular cheilitis regarded as? a) Fungal b) Bacterial c) Viral d) Oral Neoplasm | a) Fungal Other fungal manifestations include erythematous candidiasis and pseudomembranous candidiasis |
| What type of infection is non-hodgkin's lymphoma (NHL) regarded as? a) Fungal b) Bacterial c) Viral d) Oral Neoplasm | d) Oral Neoplasm |
| What type of infection is Kaposi's sarcoma regarded as? a) Fungal b) Bacterial c) Viral d) Oral Neoplasm | d) Oral Neoplasm This is a cancer commonly occurring in AIDS patients |
| Identify the HIV-associated fungal oral manifestation A creamy white or yellow plaque which, when scraped, reveals an erythematous or bleeding mucosal surface | Pseudomembranous Candidiasis |
| What type of infection is linear gingival erythemia regarded as? a) Fungal b) Bacterial c) Viral d) Oral Neoplasm | b) Bacterial |
| What type of infection is herpes regarded as? a) Fungal b) Bacterial c) Viral d) Oral Neoplasm | c) Viral |
| Oral hairy leukoplakia (OHL) is induced and maintained by the direct infection of epithelial cells in the saliva by which virus? | The Epstein-Barr Virus (EBV) OHL is considered a marker of immunosuppression, and thus is considered a viral oral manifestation of HIV |
| Name the viral infection | Expansive Ulceration |
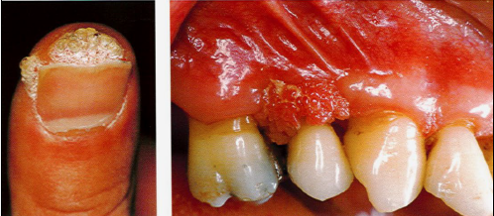
| Name the viral infection/lesion | Human Papilloma Virus (HPV) / Verrucae Wart |
| Which virus is known for causing Kaposi's sarcoma? | Kaposi sacroma-associated herpesvirus (KSHV) (HHV8) |
| While it may vary in appearance, describe generally the clinical presentation of non-hodgkin's lymphoma (NHL) | - Diffuse - Rapidly proliferating - Slightly purplish - Mass located on the floor of the mouth |
| List the 5 types of anti retro-viral therapy (aRT) medications | 1. Entry inhibitors 2. Non-nucleoside reverse transcriptase inhibitors 3. Nucleoside analogues 4. Integrase inhibitors 5. Protease inhibitors |
| What type of anti retro-viral therapy (aRT) medication is known for acting as a false substrate for reverse transcriptase, causing chain termination to create incomplete DNA and inhibit HIV replication? | Nucleoside Analogues |
| What type of anti retro-viral therapy (aRT) medication is known for blocking the integration of HIV and cell DNA to prevent HIV replication? | Integrase inhibitors |
| Which two drugs are combined to form an injectable HIV therapy? | Cabotegravir and Rilpivirine |
| On average, how long is survival time after HIV infection if left untreated? | 9 - 11 years depending on genotype |
| True or False Even with anti-retroviral therapy medications, A.I.D.S patients experience a reduced life span | False Patients rarely die of A.I.D.S in modern times and can have a normal life expectancy if on well managed anti-retroviral drugs |
| Which conditions can long-term aRT users expect to suffer later in life? | - Increased chance of cardiovascular disease - Osteoporosis - Minor neurocognitive disorders of the brain and dementia - Increased cancer risk (lung cancer, Kaposi sarcoma, hodgkin's lymphoma, etc) |
| How do non-nucleoside reverse transcriptase inhibitors prevent the formation of HIV DNA? | They inhibit the reverse transcriptase enzyme by binding to it. |
| How often should HIV patients ideally receive blood tests? | Every 3 months |
| How often should Hepatitis C patients ideally receive blood tests? | Annually (Not always observed post-therapy) |
| True or False If a HIV+ patient with a high viral load presents to the clinic and you feel uncomfortable treating them, you may refer them elsewhere | False You don't get a choice (illegal) |
| When, in a dental setting, is a HIV or Hepatitis C patient required by law to disclose their positive status? | Following a needle-stick injury and only if you have asked them directly. E.g. "do you have any reason to believe you may be carrying an infective blood-borne virus e.g., HIV or Hepatitis C?" Otherwise, the patient is not required to disclose anything |
| What is the correct procedure following a needle-stick injury with a HIV or Hepatitis C positive patient? | 1. Remove gloves and wash hands thoroughly 2. Inform the patient that it has taken place, ask if they have any reason to believe they are carrying a blood-borne virus e.g. HIV 3. If no, both you and the patient should be blood tested on the same day for HIV and Hep C 4. If the patient is a known HIV carrier, you should already be aware of what medications they are taking, the last blood test, and the results 5. For HIV seek medical advice and take "PeP" (not an option for Hep C) |
| True or False "PrEP" is a 28-day course of anti-retroviral medications taken to reduce the chances of significantly seroconverting to HIV | False This describes "PeP", or "Post Exposure Prophylaxis," a drug taken following potential HIV exposure PrEP, or "pre-exposure prophylaxis," is taken before potential exposure i.e. a safe sex tool |
| True or False "PrEP" functions doubly as an anti-HIV medication and anti STI medication | False PrEP does not protect the patient from STI's |
| True or False In molar-incisor hypomineralisation, defects are usually asymmetrical i.e. teeth can be clinically sound while the contralateral tooth presents with severe defects | True |
| List 2 potential aetiological/causative factors of MIH | 1. Genetics 2. Medical problems during pregnancy 3. Dental trauma 4. Postnatal problems/diseases during first year of life |
| Which of the following is NOT a difficulty associated with MIH-affected teeth? a) Hypersensitivity b) Anxiety c) Poor aesthetics d) Difficulties with anaesthesia e) Caries with fast progression f) Restoration failure g) Dysgeusia | g) Dysgeusia |
| In what phase of amelogenesis is MIH most likely to occur? | The maturation phase This is the second of the two main phases of amelogenesis, with secretion being the first |
| In what phase of amelogenesis is hypoplasia most likely to occur? | The secretory phase |
| Which phase of enamel formation is described below? A release of protons is neutralised by bicarbonate secretions from ameloblasts | The maturation phase Inhibition to the bicarbonate pH moderation system is considered a possible cause of hypomineralised enamel |
| True or False Decreased carbonate during enamel formation has been reported in MIH enamel | False However, INCREASED carbonate beyond levels usually found during amelogenesis is associated with MIH enamel |
| Which of the following is NOT considered a cause of MIH during amelogenesis 1. Excess proteinases 2. Apoptosis of ameloblasts 3. Inefficient bicarbonate production by ameloblasts 4. Excess carbonate 5. Failure of tight junctions between ameloblasts 6. Secretion of altered proteins by ameloblasts 7. Excess albumin in enamel matrix | 1. Excess proteinases However, deficient proteinases are |
| Name an environmental toxin found in polycarbonate plastics and epoxy resins implicated in MIH causation | Bisphenol A (BPA) |
| Name 3 birth complications linked to MIH | 1. Infant hypoxia 2. Maternal smoking in late pregnancy (hypomineralised second molars) 3. Caesarian section |
| Which of the following is linked to MIH? a) Amoxicillin b) Eryhtromycin c) Antibiotics d) Chemotherapeutic drugs e) None of the above | e) None of the above (Based on evidence so far) |
| Describe the clinical appearance of enamel disintegration | - Varying degree of porosity in hypomineralised areas - Masticatory forces may break down enamel - Unprotected dentine - Rapid caries development |
| Describe the clinical appearance of demarcated opacities | - At occlusal or buccal part of crown - Varied in colour (white, creamy, yellow to brownish) - Defects are >1mm in size |
| Would an MIH lesion with demarcated opacities, enamel breakdown, caries, and persistent/spontaneous hypersensitivity affecting function be described as: a) Mild b) Moderate c) Severe | c) Severe Moderate is not a classification used and Mild defects only exhibit occasional sensitivity to external stimuli and no caries |
| Which of the following is TRUE about Mild MIH? a) It's asymmetrical b) It includes caries presence c) It's symmetrical d) It can be a result of amelogenesis imperfecta | a) It's asymmetrical |
| Statement 1: Amelogenesis imperfecta often appears yellow with a slight roughness and heavy pitting Statement 2: Amelogenesis imperfecta is a form of MIH | Both statements are false Amelogeneis imperfecta DOES present as rough and yellow but does not involve pitting |
| True or False You can expect to find a healthy periodontium in a patient with a gingival abscess | True A gingival abscess is a localised acute inflammatory lesion of the gingival margin |
| What is the name given to an abscess in the soft tissue circled? | Pericoronal abscess (or pericoronitis) Most frequently seen in the operculum around mandibular third molars |
| True or false A periodontal abscess is considered a dental emergency | True |
| Which microflora are commonly associated with periodontal abscesses? | Anaerobes (anaerobic cocci, anaerobic gram-negative bacilli, and anaerobic gram-positive bacilli) |
| What challenges, other than pain, might arise when attempting to probe a tooth associated with a periodontal abscess | The swelling caused by the abscess may close the entrance to the periodontal pocket, making it near impossible to probe This occlusion of the pocket is how/why exudate accumulates in the area, as, until a fistula forms, it has nowhere to travel |
| Which of the following IS exhibited in a periodontal abscess which has become chronic? a) Extreme pain b) Sensitivity c) Elevation/extrusion of the tooth d) Exudate expressed from gingival margins e) Mobility | c) Elevation/extrusion of the tooth Every other symptom listed is associated with acute infection. Chronic abscesses are often asymptomatic with the exception of sinus tract formation, tooth elevation, and episodes of dull pain |
| What diagnostic methods/tools are used in the diagnosis of a periodontal abscess? | 1. Peri-apical radiographs 2. Vitality tests |
| True or false Both lymphadenopathy AND leukocytosis (high WBC count) is associated with periodontal abscesses | True |
| Should debridement and irrigation with chlorhexidine/saline fail to resolve a periodontal abscess, what measures might a dentist resort to? | 1. Draining the abscess through the sulcus by incision of overlying mucosa 2. Penicillin or other antibiotics are prescribed if abscess is associated with fever |
| Where does bacteria travel in periodontal-endodontic lesions? | From a periodontal pocket associated with LOA and root exposure through accessory canals to the pulp tissue where it may cause necrosis |
| Complete the following In an endodontic-periodontic lesion, ______ necrosis precedes periodontal changes | In an endodontic-periodontic lesion, PULPAL necrosis precedes periodontal changes |
| True or False Endodontic infections should always be controlled prior to treating a periodontal lesion (e.g. abscess) | True |
| Statement 1: In periodontal abscesses, intense pain is often felt by the patient before swelling has even begun Statement 2: In endodontic-periodontic lesions, infection from the pulp chamber travels apically until it leaves the tooth, then migrates cervically. | Statement 1 is False Statement 2 is True Pain before swelling is associated with endodontic abscesses. Periodontal abscesses usually aren't painful until they are already swollen |
| True or False It is possible to have an endodontic abscess with no pocket formation, however periodontal abscesses always involve some form of pocketing | True |
| True or False Teeth associated with peridontal abscesses may be tender to percussion | True However not often and usally very mild |
| Although occlusal trauma is a histological term, clinical diagnosis may be made in the presence of certain oral manifestations. Name 5 clinical signs of occlusal trauma | 1. Progressive tooth mobility 2. Adaptive tooth mobility (fremitus) 3. Thermal sensitivity 4. Radiographically widened PDL space 5. Tooth migration 6. Discomfort 7. Pain on chewing 8. Root resorption 9. Fractured teeth 10. Hypercementosis |
1 comment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
over 3 years ago
too many questions
Want to create your own Flashcards for free with GoConqr? Learn more.