3646985
Description

Flashcards by Natashia Reyes, updated more than 1 year ago
|
|
Created by Natashia Reyes
over 8 years ago
|
|
| Question | Answer |
| Juvenile Idiopathic Arthritis (aka Juvenile Rheumatoid Arthritis) What Is It Cause Leading Cause Of | An autoimmune inflammatory Disease No KNOWN cause, it is the Leading Cause of childhood disability and a more common chronic disease in children |
| DIAGNOSIS What Age How Many Joints Must Be Affected What Is Excluded Criteria | For JIA dx the child has to be UNDER 16 and have joint swelling in one joint for at least six weeks that is not a result of trauma, infection, or malignancy |
| Most Common Age Onset Most Common Sex Cause | 2-4 years old Girls 3x more likely No known cause |
| What Is Most Affected What initiates immune Complexes What Causes Chronic Inflamm & Joint Des Inflammation Causes | Synovial Structures usually clear and viscous for lubricating articular cart. Immune complexes in blood and synovial tissue init. Phagocytosis and accum of immune complexes. Excessive fluid unlike normal watery and thin so synovium swells and thickened villi and nodules protrude into joint cavity. |
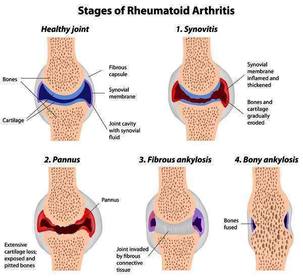
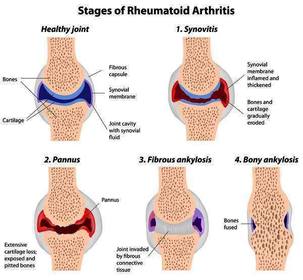
| Pannus Is | Pannus-inflamed granulating tiss, formation occurs over articular cartilage with further deterioration articular cartilage and contiguous bone become eroded and destroyed |
| AGE 1-4 Years Old | More females than males Subtype is Oligoarticular, early onset Four or Fewer joints some one joint ANA+ in 60% increased risk uveitis |
| 9-12 Years Old | Enthesitis-related arthritis (late onset Oligoarticular) More Males than Females, four or fewer can have polyarticular course, possible sacroilitis (bottom) May carry HLAB27 gene, enthsitis (where tendons or ligaments insert into bone) |
| RF - Polyarticular | More Females than Males, 1-4 years old 5 or more joints, small and large joints, RF-, symmetrical involvement |
| RF + (Positive) | More Females Than Males, onset 9-16 years old, 5 or more joints small and large joints, RH +, rheumatoid nodules, risk of bony erosion, symmetrical involvement |
| Systemic Onset JIA | Equal sexes, polyarticular movement, high daily or twice daily spiking fevers, rash, risk of pericarditis, lymphadenopathy, hepatosplenomegaly |
| Describe Joints Morning Description If Untreated | stiff, swollen, warm to touch, erythematous, limited rom Worse in morning called "gel phenomenon" because joints gel in place untreated uveitis (inflammation of eye structure) and uveal tract can lead to vision loss |
| STAGES OF RA | |
| Diagnostic Eval | Comprehensive Hx and Physical, characteristics, frequency, and severity of systemic and articular manifestations |
| LABS | Antinuclear antiody (ANA), Human Leukocyte antigen B27 (HLA-B27) nd anti-cyclic citullinated peptide (anti-CCP) antibody identify subtype CBC, ESR< CRP identify presence of inflammation |
| Slit Lamp Eye Exam More Frequently When | Should be done routinely to screen for Uveitis which occurs more frequently in the presence of ANA positive |
| Therapeutic Goals | There is no cure goal is for preserving joint function, controlling inflammatory process, minimizing deformity, and reducing impact of disease on chlid's development will entail physical and occupational therapy, family education, home care, encouragement of age appropriate activities |
| DRUG THERAPY: NSAID when DMARDs why Methotrexate when Biologics when Corticosteroids for what | NSAID-first line treatment DMARD if child's condition does not improve in 4-6 weeks started at dx (if mod to severe) Bio to completely control arthritis to reduce inflammation in selected joints |
| Active ROM vs. Passive ROM | Active-and rest during times of increased synovitis and pain gentle movement through ROM maintains joint mobility Passive ROM-NOT indicated for early stages of disease or times of active inflammation instead encourage play activities to increase active range Rest or frequent breaks throughout the day |
| When Can Gradual Strengthening Begin What Would Be Examples | After Synovitis is well controlled and functional ROM is obtained can be low impact strengthening by swimming and riding a bike. Parent should promote child's participation in age appropriate activities if no restrictions per therapy |
| What are Additional Modalities for Reducing Pain and Maintaining Range During Painful Episodes | Hot baths, whirlpools, moist hot packs, paraffin baths for heat at home or in conjunct with therapy reduces joint stiffness and increasing elasticity of tissues surrounding joints making stretching more effective |
| Why Splint | It rests the joint, decreases pain, aligns the joint in proper position, and is helpful as a support as the child becomes more active. Goal is to keep child active and able to keep up with peers activity should be encouraged though modification may be needed |
| Surgical Intervention | Rare but may be needed for contractures, micrognathia (jaw undersized), or unequal growth of the extremities |
| NURSING ASSESSMENT Assess Affected Joint For | Status of affected joints, child's physical limitations, level and intensity of pain, child and family response to disease -Swelling, warmth, tenderness, pain, and limited ROM |
| Be Alert For | Guarding of painful joints, refusal to bear weight, limping, facial expressions of discomfort |
| Parent May Describe Child As | Fussy and irritable in the morning reluctant to walk or be carried |
| Assess for Systemic Involvement by | history of temperature elevations, especially in late afternoon or evenings, determine whether rash occurs with fever, assess for anorexia, weight loss, and failure to grow |
| Managing Pain | Know/teach Verbal and Nonverbal indicators (nonv like restlessness, withdrawl, decreased attention span, increased crying, decreased sleep) |
| Most Effective Way to Assure Max Comfort NSAID Relevance Nonpharmacological Pain Relief | -Therapeutic Blood Level of pain med -NSAID give with food or milk to prevent GI irritation -diversion, splinting, heat or cold application, imagery, meditation some children |
| Interventions to Teach Parent for AM Routine | Child may need more time in AM, give plenty time to wake up, provide warm shower or bath, keep child's room or bed warm, administer NSAID in AM with snack allowing it to take affect before child rises |
| Live Virus Vaccination Held if On | DMARD or Biologic Medication such as varicella, measles, mumps, rubella (MMR) and flu-mist, must be held. Yearly flu is allowed in injectable form |
| How To Facilitate Emotional & Social Development How Will Anticipatory Guidance Help School Nurse Involvement | Expressive Therapy though doll play, painting boards, bean bags, clay, painting, story composing (safe mechanisms for reducing stress). will help child develop coping mechanism fostering optimism Communication necessary for rest periods allow to bring a friend for short period of quiet activity |
| Parent Involved? Teaching Good? | Yes, as many nursing activities as possible to reduce anxiety and increase sense of control. Provide verbal and written instructions and return demonstration needed |
| Diet? What To Do When Anorexia is Present or Pain When Eating | High fiber, protein, and calcium with adequate fluid intake. -consider more frequent high calorie foods. Don't forget emphasis for regular visits to the ophthalmologist |
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.