3817498
| Question | Answer |
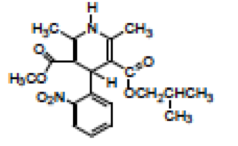
| NIFEDIPINE first ca blocker peripheral potent vasodilator 10 min onset used to be used in bolus 10-20mg TID (not anymore) Now used ER (like most ccb) Can cause ankle edema (sign of too high dose or Heart failure) can cause reflex tachycarrdia (can cause MI, but given with beta blockers reduces this) | |
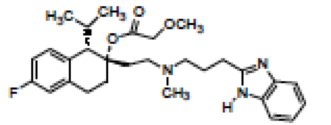
| NICARDIPINE Potent peripheral vasodilator not much effect on SA or AV nodes Major effect is vaso dialtor (no ionotropic effect) Can cause reflex tachycardia used to be the only IV CCB | |
| FELODIPINE Antihypertensive | |
| CLEVIDIPINE Only IV good for dose titration in 15 min effects will disappear 1/2 life of 1 min proprionates are rapidly hydrolyzed in humans and allows for rapid elimination | |
| ISRADIPINE Not ER Dihydydropyridol anti htn 2.5mg QD-10mg highest if you used 15-20mg you increase risk of peripheral edema 1/2 life of 8 hrs | |
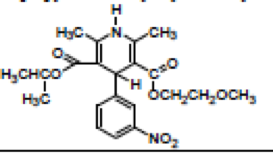
| NISOLDIPINE ER 1/2 life of 7-12 hours Peripheral Vasodilator | |
| AMLODIPINE 2nd gen dihydropyridol Slower onset peak plasma concentration in 6-12hrs 1/2 life of 35-48hrs no acute htn or reflex tach useful in combination with lipitor (called caduet) | |
| NIMODIPINE used for cerebral arterial spasms which are complications from subarachanoid hemmorages Need to treat within 96 hours take 60mg every 4 hours for 21 days (capsules) If they cannot swallow give via NG tube Vasodilators of arteries can help this conditon cannot give this drug parenterally not used for HTN or angina can cause birth defects 1/2 of patients of SAH die from birth defects | |
| MIBEFRADIL (WITHDRAWN) BMS marketed said it was like DHP lead to many deaths | |
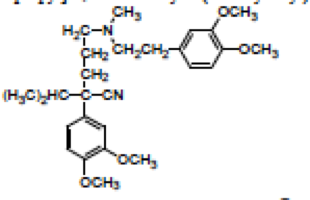
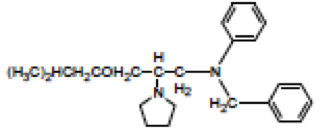
| VERAPAMIL 1/2 life of 5 hours affects myocardia not peripheral vasculature decrease in chrono and iono decrease in effect on vascular smooth muscle some blockage of Na channels can be used in cardiac arrythmias block tachycardia better than nifedipine AV node effect is greater Peroxisomal supraventricular tachycardia treatment 80-160 mg or 120-240 ER given IV Used for CHRONIC stable and unstable angina and HTN | |
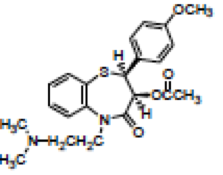
| DILITIAZAM Effect as coronary vasodilator (increase in O2) Reduces coronary Arterial spasms anti arrythmic (less than verapamil) Can have effect in peripheral vasculature (less than nefidipine but more than verapamil) effort associated angina or HTN Sustained release capsule 60-90mg can be IV for AFIB and PSVT (arrythmia) | |
| Bepridil HCL Antianginal | |
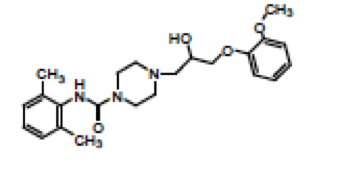
| RANOLAZINE Na channel blocker Angina ER (500mg - 1g) once daily doesnt alter HR or BP control CO at maximum exercise increases exercise tolerance Decrease in # of angina attacks No anti arrythmic properties Effects NA dependent Ca channels. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.