6221900
Description
Flashcards by Ashutosh Kumar, updated more than 1 year ago
|
|
Created by Ashutosh Kumar
over 9 years ago
|
|
| Question | Answer |
| Clinical examination of Facial nerve (CN VII): | Motor function: Inspect carefully for any asymmetry of the face as a whole, or blinking or eye closure. Ask the patient to raise their eyebrows. Then ask the patient to show you their teeth (smile from ear to ear). Demonstrating yourself and then asking the patient to mimic. Look for any asymmetry. Test power by giving the instruction “close your eyes tightly shut and stop me from opening them”. “Blow out your cheeks with your mouth closed” (purse lips and puff out their cheeks). Taste Taste sensation is not tested routinely and we will not be doing this today, but it is done by applying cotton buds dipped in sweet, salty, sour and bitter solutions to the anterior two-thirds of the tongue. The patient is asked to identify which has been applied, and must rinse their mouth between applications. |
| Signs and symptoms of different levels of Facial nerve lesions (CN VII): | In a unilateral LMN lesion of the facial nerve there is weakness of both upper and lower facial muscles, therefore the forehead doesn’t wrinkle, the eye can’t close, and the corner of the mouth droops on the affected side. The mouth deviates to the unaffected side. The loss of eye closure is a serious threat to the cornea. In a unilateral UMN lesion such as a stroke, facial paresis is marked in the lower facial muscles with relative sparing of the upper face. This is because there is bilateral innervation of the upper facial muscles. This will be seen as the corner of the mouth drooping but eye closure is well preserved. |
| Clinical examination of the vestibulocochlear nerve (CN VIII): | Balance is tested by the patient standing upright with their feet together and eyes open. Once stable, ask them to close their eyes for up to a minute. Compare steadiness with their eyes open and closed. Be ready to support them if they become unsteady. The test is positive if there is considerable unsteadiness to the point where the patient needs to open their eyes or move in order not to fall. Hearing is test simply by occluding the opposite external meatus (by pushing of the tragus) and whispering a number at about 60 cm from the ear under test. Other ways of standardising the method include whispering towards the end of expiration, and using set numbers for different tones; 68 (high tone) 100 (low tone). If your voice is soft enough you will notice that your larynx doesn’t vibrate. If you suspect partial deafness as a result of the above testing, Rinne’s and Weber’s tests are used to determine whether this is nerve deafness (e.g acoustic neuroma) or conductive deafness (e.g middle |
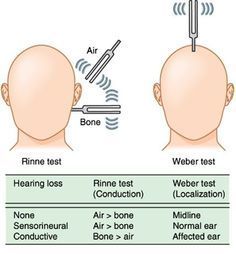
| Rinne's and Weber's tests: | Rinne’s test: Set a 256 Hz or 512 Hz tuning fork vibrating and place it on the mastoid process. Once vibration is no longer heard move the vibrating fork level with the external auditory meatus. Normally air conduction is better than bone conduction. In nerve deafness the tone will be audible once the fork is moved as both bone and air conduction are equally reduced. This is called Rinne positive. In conductive deafness the tone will not be audible once the fork is moved. This is called RInne negative. Weber’s test: Set the same 256 Hz or 512 Hz tuning fork vibrating and place it on the centre of the forehead. Normally the sound is heard in the centre. If there is nerve deafness, the sound will localize to the normal ear and be heard loudest there. If there is conductive deafness, the sound is heard loudest in the affected or abnormal ear. |
| Clinical examination of the glossopharyngeal and vagus nerves (CN IX and X): | Ask the patient to speak in order to assess hoarseness (which may occur in a unilateral recurrent laryngeal nerve lesion), and then to cough. Listen for the characteristic bovine cough that occurs with recurrent laryngeal nerve lesions. Assess the patient’s speech for dysarthria or dysphonia. While the patients says “Aaah” look at the movements of the palate and uvula using a torch. Test pharyngeal sensation by gently using a tongue depressor. Elicit the gag (pharyngeal) reflex by touching the posterior pharyngeal wall of faucial pillars with a tongue depressor. Apply the stimulus to both sides in turn. Ask the patient to puff out his or her cheeks with the lips tightly closed. Look and feel for air escaping from the nose. Test the patient’s ability to swallow a small amount of water and watch for regurgitation into the nose, or coughing. It is not routinely necessary to test taste on the posterior third of the tongue (CN IX). Testing pharyngeal sensation and the gag reflex are unpleas |
| Signs and symptoms of different levels of glossopharyngeal and vagus nerve lesions: | Normally both sides of the palate elevate symmetrically and the uvula remains in the midline. In order to puff out the cheeks, the palate must elevate and occlude the nasopharynx. If palatal movement is weak, air will escape audibly through the nose. The gag reflex produces elevation of the palate and the pharynx, very similar to the motions seen at the beginning of vomiting. Isolated unilateral IX lesions are rare. Damage to the vagus on one side leads to deviation of the uvula when the soft palate is elevated by saying ‘Aaah’. Damage to the recurrent laryngeal branch of X causes dysphonia and a ‘bovine’ cough. Causes include lung cancer, thyroid surgery, mediastinal tumours and aortic arch aneurysm. Bilateral X nerve lesions cause both bulbar and pseudobulbar palsies. They are associated with dysphagia, dysarthria and either lower or upper motor neuron lesions of the hypoglossal (XII) nerve. Less severe cases can result in nasal regurgitation of fluids and nasal air escape when the cheeks are puffed out. |
| Clinical examination of accessory nerve (CN XI): | Face the patient and inspect the sternocleidomastoid muscles for wasting or hypertrophy and palpate them to assess their bulk. To test power in the left sternocleidomastoid ask the patient to turn their head to the right while you provide resistance with your hand placed on the right side of the patient’s chin. Reverse the procedure to check the sternocleidomastoid. Stand behind the patient and inspect the trapezius muscle for wasting or asymmetry. Ask the patient the patient to shrug their shoulders as you apply forceful downward pressure with your hands. |
| Clinical examination of hypoglossal nerve (CN XII): | Ask the patient to open their mouth. Look at the tongue at rest for wasting, fasciculation or involuntary movement. Ask the patient to protrude their tongue. Look for deviation or involuntary movement. Ask the patient to move the tongue from side to side. Test power by asking the patient to press the tongue against the inside of each cheek in turn while you press from the outside with your finger. Assess speech by asking the patient to say ‘yellow lorry”. |
| Signs and symptoms of different levels of hypoglossal nerve lesions (CN XII): | Unilateral LMN lesions lead to wasting of the tongue on the affected side and deviation to that side on protrusion. Bilateral lower motor neuron damage results in global wasting-the tongue lies thin and shrunken like an autumn leaf. When associated with lesions of IX, X and XI, typically in motor neuron disease, these features are called bulbar palsy. Upper motor neuron lesions on one side are uncommon, while bilateral lesions lead to a spastic, bunched up, almost conical or acorn-like tongue. Bilateral supranuclear lesions of IX-XII are called pseudobulbar palsy and usually result from vascular disease, motor neuron disease or occasionally multiple sclerosis. In addition to dysarthria most cases of severe tongue weakness are associated with dysphagia. Tremor of the resting or protruded tongue is common in Parkinson’s disease. Other movements of the mouth and tongue (orolingual dyskinesia) are often drug induced (e.g antiparkinsonism drugs and neuroleptics). |
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.