6394570
Description
Flashcards by Derek James, updated more than 1 year ago
|
|
Created by Derek James
over 7 years ago
|
|
| Question | Answer |
| Treatment Goals of Early CKD | • Slowing progression of disease • Increase survival time • Increase quality of life |
| Treatment Goals of Late CKD | • Only palliative effects • Control uremic symptoms • Improve quality of life |
| What stages of CKD are considered early? | IRIS I/II |
| What stages of CKD are consider late? | IRIS III/IV/V |
| Why do we encourage as much water intake as possible for cats with CKD? | -Maintains hydration status -Promotes osmotically driven polyuria and compensatory polydipsia |
| Does protein restriction help in early CKD? | We are “Less certain if protein restriciton alters progression of renal failure in dogs or cats” |
| What is Proteinuria and how does it relate to CKD? | -Elevated Urinary Protein Concentration -An independent risk factor for reduced survival in cats and dogs with naturally occurring renal disease. |
| Effects of protein restriction (early CKD)? | -The effects of protein restriction are not clear with natural disease. -High dietary protein corresponded to high UPC in lab-induced dz. -Logic: moderate protein may limit diet-related "hyper filtration" |
| So should we protein restrict in Early CKD? | Start low and adjust to effect based on BW, BCS, MCS, TP, albumin, etc... |
| Define Azotemia | From Wiki: a medical condition characterized by abnormally high levels of nitrogen-containing compounds (ex: urea, creatinine, etc) in the blood. |
| Define uremia | Urea in the blood. |
| Why do uremia and azotemia occur in CKD? | It is from the accumulation of protein metabolites that would normally be filtered by the kidneys. |
| What are the correlates of excess/high protein intake in late CKD? | Azotemia and morbidity. -Clin Signs decrease with lower BUN |
| What are the correlates protein malnutrition in late CKD? | Morbidity/mortality. Clin signs: hypoalbuminemia, anemia, weight loss, muscle wasting. |
| What is the goal of protein restriction in late stage CKD? | -Provide a HIGH QUALITY PROTEIN -Ensure essential AAs covered -Controlled reduction of non-essential AAs to reduce prod'n of nitrogenous waste products and therefore clin signs. |
| How do we determine the minimal protein requirements for late CKD patients? | We currently just assume the minimal needs are similar to healthy animals. |
| When should we restrict phosphorus in cats (with or without CKD)? | -In healthy cats and IRIS stage I cats, continue normal diet. -In IRIS stage II-IV, low phosphorus diet and maybe phosphate binders are indicated. |
| Hypertension with CKD | Common. Contributes to progression of disease. Risks target organ damage to kidneys, eyes, brain and heart. Treat with anti-hypertensives. |
| Should we restrict sodium in CKD? | The recommended target is .25-.65% on a DM basis. AVOID high sodium. However, we lack evidence of benefit. |
| Hypokalemia in CKD | -20-30% of CKD cats have hypokalemia likely d/t reduced intake (anorexia, vomiting) and excessive renal losses. -Potassium intake ↓ with ↓ protein intake & metabolic acidosis can cause loss of buffering capacity. -Combat with mod protein and sufficient K diet. |
| Buffering Capacity in CKD | -↓ Urinary acid excretion & metabolic acidosis -Feed mod protein with low sulpher containing AAs -Buffers include K citrate, K gluconate |
| Goal of supporting buffering capacity in CKD | -Urinary pH of 6.5-7.0 (alkaline) |
| What is the purpose of antioxidants in CKD? | Renal diet + additional vit E/C and beta-carotene promotes less oxidative DNA damage and lowers urea levels. |
| What if your feline CKD patient is anorexic? | MAKE SURE THE PATIENT EATS. Choose a highly palatable, high protein, high energy diet in small amounts in the short term. DO NOT FORCE FEED. Stimulate appetite. Tube feeding>forced. Once you get appetite back, gradual transition to renal diet. |
| Appetite Stimulation Suggestions (Cats)? | ▫ Warm up the food to body temperature ▫ Small, frequent meals (6-8 per day) ▫ Take the food away after 15 min and try again later, etc... |
| Purpose of soluble fibre in CKD? | Helps to increase faecal urea excretion and decrease blood urea and urinary urea excretion. (In small intestine: escapes enzymatic digestion. In large intestine: promotes anaerobic bacterial fermentation) |
| Define Urolithiasis | Condition where calculi form in the urinary tract |
| What type of stone(s) can hypercalcemia cause? | Calcium oxalate. Hypercalcemia is an example of a systemic disorder which may cause urolithiasis. |
| What type of stone(s) can Cushing's disease cause? | Calcium oxalate and struvite Cushing's dz is an example of a systemic disorder which may cause urolithiasis. |
| What type of stone(s) can defects in purine metabolism cause? Also, give an example of a purine metabolism defect. | Ammonium urate. Portal vascular abnormalities. Purine metabolism defects are examples of a systemic disorder which may cause urolithiasis. |
| What type of stones can urease-producing bacterial infections of the urinary tract cause? | Struvite |
| What type of stones can be caused by foreign material in the urinary tract cause? Give an example of foreign materials that may cause stones in the urinary tract. | Struvite stones mainly and sometimes calcium oxalate. Examples of foreign materials that may cause stones include suture material and catheters. |
| What type of stones can renal tubular acidosis cause? | Calcium oxalate. |
| How can we diagnose stones? | History, PE, CBC and chem profile, Urinalysis with culture and sensitivity, Imaging (rads +/- contrast, U/S), Stone analysis. |
| What factors influence crystal/urolith formation? | -Calculogenic ions, urine pH, and urine volume. -Urine is a complex medium with calculogenic ions |
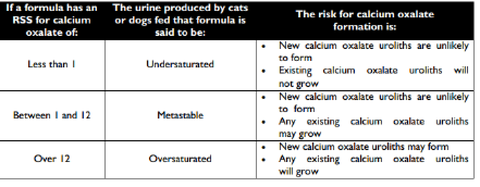
| What is RSS? | -RSS=Relative supersaturation -Used to assess the diet-specific risk of crystal/urolith formation in urine of dogs and cats. |
| UNDERSATURATED: ZONES/LEVELS OF URINARY SATURATION | No crystal nidus formation or growth. Dissolution is possible. |
| Metastable: ZONES/LEVELS OF URINARY SATURATION | Nucleation possible but minimal growth. Dissolution is no longer possible |
| Oversaturated: ZONES/LEVELS OF URINARY SATURATION | Spontaneous nucleation with MAXIMAL growth. Dissolution not possible. |
| Biologic behaviour of struvite stones | Fast growing, smooth, dissolvable, alkaline environment, high recurrence (d/t UTIs), RADIODENSE. |
| Struvite treatment plan | Urinalysis (triple phosphate returned) Dissolution possible. Removal only if needed. Treat underlying UTI. I.e. long-term treatment with amoxicillin +/- clavulenic acid. |
| Dietary consideration regarding struvite stones | Dissolution and prevention diets are available. Restrict Mg and P (cautiously) in diet. Restrict protein in dogs as it promotes polyuria. |
| What is the single most important factor in urolithiasis cases? | WATER INTAKE. Increase it. Aim for USG <1.020 in first morning urine. |
| Give example of diet acidifiers for struvite cases. | DL-Methionine Ammonium chloride. |
| RSS approach to struvite | Feed formulas with measured RSS less than one (undersaturated) to dissolve existing stones. Formulas w measured RSS 1-2.5 are metastable and will not dissolve or grow existing stones. Formulas w measured RSS >2.5 will grow stones and form new ones. |
| Biological behaviour of calcium oxalate | Slow growth; jagged or smooth; acidic-neutral urine?; recur >50% within 3 yrs of removal; RADIODENSE |
| Calcium oxalate Tx plan | -UA to find out type. UA could be negative. -Strong suspicion with radiodense uroliths, urine C&S negative, hypercalcemia, predisposed breed, advanced age, steroids etc. -REMOVAL: surgical, lithotripsy, voiding urohydropulsion -stone analysis |
| True or False: Dissolution of calcium oxalate stones is possible | FALSE. Removal is the only option. (surgical, lithotripsy, voiding urohydropulsion) |
| Should we restrict calcium for calcium oxalate stones? | The current suggestion is to moderately restrict. Ca is so tightly regulated that it might not do much since homestatic mechanisms (bone resorption, increased absorption) might counter what we do. |
| Should we restrict oxalates with calcium oxalate stones? | We want to avoid high oxalates and balance with moderate Ca restriction. Recall: Absorption affected by serum [Ca2+]: If ↓serum [Ca2+] oxalate hyper-absorption from GIT to accompany |
| Should we restrict Vit C for calcium oxalate stone cases? | YES. Restrict since Vit C is a precursor for oxalate. |
| How does excessive protein contribute to calcium oxalate stone formation? | -Excessive protein contributes to hypercalciuria and hypocitraturia. -Citrate (-vely charged) binds Ca2+ - Ca2+ is available to complex with oxalate -Also, it promotes oversaturated urine. |
| Why do we need to be careful with Phosphorus restriction with calcium oxalate stones? | If we restrict too low, we'll increase Ca2+ absorption from GIT and more resorption from bone --> hypercalciuria |
| How can magnesium help with calcium oxalate stones? | Can inhibit calcium oxalate formation by binding both Ca2+ and oxalates thereby preventing complexing. Caution: too much can promote hypercalciuria. |
| Calcium oxalate dietary options? | Reminder, dissolution is not possible but preventative diets are available. |
| Urine Alkalizing Agents for Calcium oxalate stones | Potassium Citrate -Use pH strips to monitor the urine. |
| RSS Approach to Calcium oxalate stones | |
| Ammonium Urate Biological behaviour | Smooth and round; can spontaneously dissolve, grow or stay static, radiolucent but hyperechoic; acidic urine; recur 33-50%. Rare compared to struvite and calcium oxalate. |
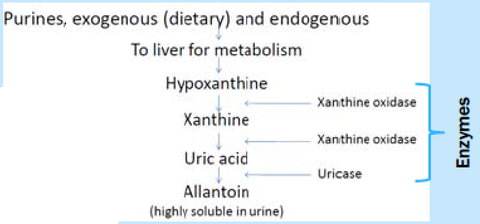
| Normal Physiological fate of purines: What are they excreted as? What enzyme is important for the final transformation? | |
| Dalmation pathogenesis of Ammonium nitrate stones | -Problem with uricase (plenty of enzyme but inefficient uric acid oxidation to allantoin), autosomal recessive trait -End result: Uric acid ↑ 2-4x in urine -Small % of dogs form stones |
| NON-Dalmation pathogenesis of Ammonium nitrate stones | -Liver dysfunctin: portal vascular anomalies or end-stage failure/cirrhosis. -Inadequate conversion of uric acid to allantoin and inability to convert ammonium-> urea -End result: uric acid and ammonia ↑ in blood and urine |
| Treatment Plan for Ammonium Urate | Dx on UA Dissolution may work Removal is an option Medical management: diuretics, xanthine oxidase inhibitor in dogs, urine alkalizing agents |
| What is allopurinol? | It is a xanthine oxidase inhibitor. It is needed in addition to a dietary change for ammonium urate. |
| Ammonium urate stones: nutrients of concern | -Restrict purines (shellfish, fish, goose, heart, kidney, liver, gravies) within at least first 3 ingredients. Restrict prot overall. Increase water (as always) -Sodium can help increase thirst and urine output but may cause hypercalciuria. -Avoid excess vit D |
| What urine pH should we aim for with ammonium urate stones? | Cats: 6.8-7.2 Dogs: 7.1-7.5 -pH >7.5 predisposes to calcium phosphate so try and avoid. |
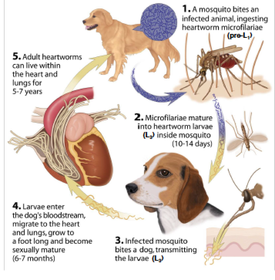
| Life cycle of Heartworm | |
| Where is the heartworm line? | ~80% of heartworm cases in Ontario are south of the 402/401/403. Caledon |
| How prevalent is clinical disease in heartworm dogs in Ontario? | Low (~12%) in 2010 |
| Is heartworm more or less prevalent in cats than in dogs? | Less prevalent. About 5-15% that of dogs. |
| How does the parasite burden required to cause disease vary in cats compared to dogs? | While cats typically have lesser numbers of parasites, ONE para can cause disease. |
| What is different about testing cats vs dogs for heartworm? | RUN Ag and Ab tests simultaneously |
| What other parasites do many heartworm preventative products also work against? | Roundworms, Hookworms +/- fleas |
| What is "reach back activity"? | Drugs with reach back activity will kill parasites that had been maturing in the duration of the reach back time. Many drugs licensed with 1 month reach back with an effective reachback of 2 months. |
| When should heartworm prevention start? | One month after the earliest start date of transmission season (Ontario ~June 1) |
| When should heartworm prevention stop? | Within 1 month of end date of transmission season. Unless the product is Trifexis. It needs 3 months post season end. |
| When is year-round preventatives indicated? | When the transmission season is greater than 6 months. |
| If a puppy/kitten is born during the heartworm-transmission season, by what age should it receive its first preventive treatment for heartworm ? | Puppies could be bitten on day one. However, with reach back activity, the products minimum age should be fine. MAKE sure they get a preventative within 8 weeks. |
| What method should be used to screen dogs for heartworm ? | Antigen tests. Antigen only appears seven months post-infection. THEREFORE, don't test a six month old dog... |
| When should we screen for heartworm? | 7 Months after end of transmission season. |
| When should dogs be tested for heartworm? | The first time you see the dog to establish a baseline. (>7mo old) After that, licensed usage requires annual testing. Can be done less frequently=OFF LABEL. Justification needed and informed consent. ALWAYS before prescribing diethylcarbamazine |
| Why is it difficult to justify annual heartworm testing in Canada? | - low risk of infection - preventives work extremely well - very low predictive value of positive test |
| What is a good strategy to determine if heartworm testing is justified? | Perform yearly risk evaluations. -Good compliance? -Travel history? Test if these answers aren't ideal. I.e. missed a dose or travelled. |
| What do we do if a dog tests positive without clinical signs? | 1. Repeat Ag test (new sample, new company with no knowledge of 1st test) 2. Microfilaria detection (smear): concentration method. 3. Consider travel/compliance history |
| What do we do if a dog tests positive with clinical signs? | 1. Repeat Ag test (new sample, new company with no knowledge of 1st test) 2. Microfilaria detection (smear): concentration method. 3. Consider travel/compliance history 4. Radiographs 5. Echocardiography |
| What is the treatment protocol for infected dogs? | (i) Pre-treat with HW preventive on days -60, -30 and 1 (if applicable). (ii) Pre-treat w doxycycline for 4 weeks within 3mo of starting melarsomine tx. (iii) On days 1, 30 and 31 treat w melarsomine. (iv) On days 1 & 30: prednisone at decreasing dosages for 4 weeks. |
| What about the "slow kill protocol? | Not endorsed by American HW Society (or Dr. Peregrine) |
| How to we manage heartworm positive cats? | -do not use melarsomine -Treat symptomatically (e.g. prednisone) -Sx? -Monitor w Ab and Ag tests. Thoracic rads every 6-12 mo. Ag is -ve 4-5 mo following elimination |
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.