7270859
Description
Flashcards by Liam Musselbrook, updated more than 1 year ago
|
|
Created by Liam Musselbrook
over 7 years ago
|
|
| Question | Answer |
| Key questions in history of acute loss of vision | Headache - giant cell arteritis Eye movements hurt - optic neuritis Lights or flashes preceding visual loss - retinal detachment Like a curtain descending - retinal artery occlusion/giant cell arteritis |
| What are the the two types of retinal vein occlusion and what is it associated with? What kind of visual loss does it give? | Central and branch retinal vein occlusion (CRVO and BRVO) Associations: age, diabetes, HTN, smoking, obesity, raised IOP, polycythaemia Unilateral visual loss |
| Non-ischaemic CRVO | 75% of CRVO Variable VA Dilated, tortuous retinal veins Widespread haemorrhages Good prognosis Progression to ischaemic in ~30% |
| Ischaemic CRVO | Sudden severe visual loss and more severe retinal signs Causes: glaucoma, polycythaemia, HTN Macular oedema Widespread cotton wool spots Deep haemorrhages Marked RAPD |
| Complications of ischaemic CRVO | Permanent visual loss Neo-vascularisation (VEGF): - Risk of vitreous haemorrhage - Rubeotic glaucoma (new vessels on iris, blocking aqueous drainage) - Treat with pan-retinal photocoagulation and anti-VEGF agents |
| BRVO and its presentation | 3x more common than CRVO Not an emergency (eg. OP appointment) Presentation: - Reduced VA (often central, worse on waking) - Visual field defects (often altitudinal) |
| What is seen on fundoscopy with BRVO? | Findings restricted to area drained by affected vein Haemorrhage Cotton wool spots Venous dilatation Oedema |
| Central renal artery occlusion: Presentation | Sudden unilateral severe decrease in VA (usually counting fingers or worse) May be complete loss of light perception RAPD (relative afferent pupillary defect) Cherry red spot on pale retina Intermittent prodrome phase common |
| What is seen on fundoscopy with CRAO? | Pale retina (oedema) Cherry red spot (fovea contains photoreceptors only, supplied by choroid - for 6 weeks) Possible signs of hypertensive retinopathy |
| Management of CRAO | Ocular massage, rebreathing into paper bag > hypercapnia and vasodilatation -> may dislodge embolus Acetazolamide, paracentesis (aspiration of aqeous from anterior chamber) - to lower IOP |
| What is Temporal Arteritis/Giant Cell Arteritis? | Causes AION Immune-mediated vasculitis of medium and large vessels Overlaps with polymyalgia rheumatica (PMR) |
| Clinical features of temporal arteritis | Typically patient > 60 years old Usually rapid onset (e.g. < 1 month) Headache (found in 85%) Jaw claudication (65%) Visual disturbances secondary to anterior ischemic optic neuropathy Tender, palpable temporal artery Features of PMR: aching, morning stiffness in proximal limb muscles (not weakness) Also lethargy, depression, low-grade fever, anorexia, night sweat |
| Management of temporal arteritis | High-dose prednisolone - there should be a dramatic response, if not the diagnosis should be reconsidered |
| What is Anterior Ischaemic Optic Neuropathy and how does it present? | Compromise of blood supply of optic nerve (posterior ciliary artery) Jaw claudication, tender scalp, temporal headache, abnormal temporal artery, decreased VA, RAPD, diplopia, optic disc swelling/atrophy |
| Investigations and management for AION | Investigations: - CRP/ESR raised - Temporal artery biopsy (but high false -ve due to skip lesions) Management: - Oral prednisolone - May take >1 year to settle |
| Posterior vitreous detachment | Degenerative changes in vitreous (liquefaction) leads to detachment from posterior retina Occurs earlier in myopia, trauma, inflammation, connective tissue disease Usually benign, leads to increased numbers of floaters |
| What are the complications of posterior vitreous detachment? | Vitreous haemorrhage Retinal tear Retinal detachment |
| Retinal detachment: what can cause it, what are they more common in and where do they happen more rapidly? | Causes: Vitreous detachment and retinal tear, trauma, surgery More common in myopes Detaches more rapidly in superior retina |
| How does retinal detachment present? | 4 F's: Floaters, Flashes, Field loss, Fall in acuity (if macula involvement) Abnormal red reflex Grey, ballooning retina |
| Management of retinal tears and detachment | Treat larger retinal tears with laser photocoagulation Surgical intervention for detachment |
| Optic neuritis | Optic disc swelling Unilateral decrease in visual acuity over hours or days Blurring of vision (blind spot enlargement/paracentral scotoma) RAPD Red desaturation Retrobulbar aching Eye movements painful |
| Papilloedema | Bilateral disc swelling due to increased ICP Headache Transient blurring of vision, enlarged blind spots May be splinter haemorrhages, exudates, cotton wool spots if severe Eventual atrophy |
| Causes of papilloedema | Space-occupying lesion: neoplastic or vascular Malignant hypertension Idiopathic intracranial hypertension Hydrocephalus Hypercapnia Rare: hypoparathyroidism and hypocalcaemia, vitamin A toxicity |
| Optic atrophy | Disc pallor from loss of axons, glial proliferation and decreased vascularity May occur without optic disc swelling, or following optic disc swelling |
| Causes of optic atrophy | Papilloedema, optic neuritis, ischaemic optic neuropathy, POAG, optic nerve compression Retinal V/A occlusion Retinitis pigmentosa |
| Most common causes of sudden painless loss of vision | Ischaemic optic neuropathy (e.g. temporal arteritis or atherosclerosis) Occlusion of central retinal vein Occlusion of central retinal artery Vitreous haemorrhage Retinal detachment |
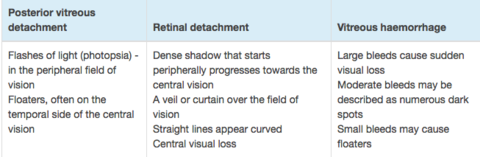
| Differentiating posterior vitreous detachment, retinal detachment and vitreous haemorrhage | |
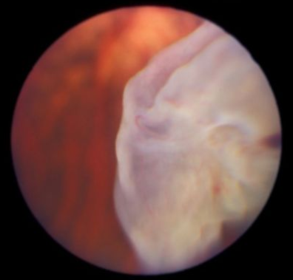
| What does this show? | Retinal detachment Features: - Dense shadow that starts peripherally progresses towards the central vision - A veil or curtain over the field of vision - Straight lines appear curved - Central visual loss |
| What does this show? | Papilloedema |
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.