7273456
Description
Flashcards by ahmad MBook, updated more than 1 year ago
|
|
Created by ahmad MBook
about 9 years ago
|
|
| Question | Answer |
| spriomycin | |
| Erythromycin | |
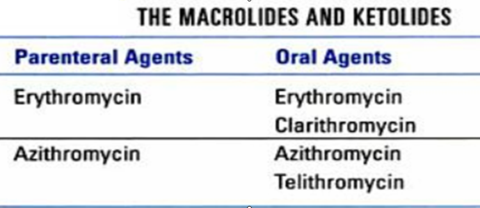
| classification of macrolides | older: Erythromycin Newer/ 2nd -Generation (semi-synthetic) : Roxithromycin, Clarithromycin & Azithromycin Newest one: (Ketolide) Teilthromycin |
| route of administration | |
| MOA: reversibly inhibit 50S subunit of bacterial ribosome by “dual MOA” | 1-Translocation movement of aminoacyl t-RNA from A-site to P-site on the mRNA 2-Transpeptidation by inhibiting peptide-transferase enzyme |
| Macrolide, Chloramphenicol, Clindamycin may competitively inhibit each other activity | Chloramphenicol &Clindamycin have the similar MOA & have closely related binding-site on the 50S ribosome combination should be avoided |
| Cidal/ Static: | usually -Static |
| Pharmacokinetics of Macrolides: | |
| Absorption: Erythromycin | orally is destroyed by gastric acid (acid-labile/acid-sensitive) It is activity is ↑ at the alkaline PH |
| Erythromycin is given as: | →Enteric-coated tablets → Add acid-stable salts Erythromycin (-stearate / -ethylsuccinate /-estolate) conjugates |
| The best absorption is obtained with | Erythromycin-estolate salt |
| absorption Azithromycin, Roxithromycin ,Clarithromycin &Telithromycin | are stable to gastric acid (acid-stable) & rapidly absorbed Food affects their absorption |
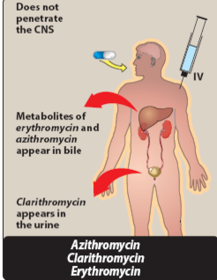
| Distribution | widely distributed to most body fluids & body tissues. CSF penetration is poor even when meninges are inflamed |
| Azithromycin > Clarithromycin → has unique pharmacokinetic properties | phagocytosed by macrophage→ travel to sites of infection → can enhance intracellular phagocyte killing of bacteria |
| Azithromycin is taken up extensively in high amounts by “tissues” | much greater concentration of the drug in the tissues as compared to its serum concentration Azithromycin → is slowly released from tissues over subsequent days (tissue half-life ~ 2–4 days) & has a prolonged T1/2 |
| unique properties of azithromycin permit once-daily dosing & shortening of the duration of treatment in many cases how?? | 3-5 day course of Azithromycin oral therapy may be adequate for most infections, instead of 7–10 days with other drugs |
| Metabolism & Excretion Macrolides | Mainly metabolized in the liver & excreted through bile dose adjustment is not needed in renal failure Except → Clarithromycin needs to be adjusted |
| Advantages of newer 2nd -Generation macrolides Azithromycin | -More acid-stablegood oral absorption) -Longer duration of action -Less frequent administration/once-a-day administration (better compliance) -Low side effect profile: +Less GI side effects (better tolerated) +Less effect on hepatic drug metabolizing enzymes→ less drug-drug interactions |
| (Azithromycin has no effect on hepatic metabolizing enzyme) | less drug-drug interactions |
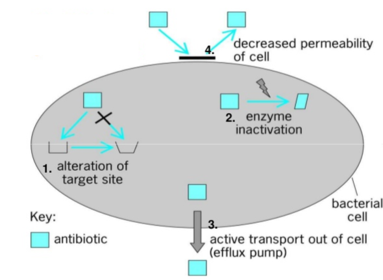
| Resistance is becoming increasingly common& occurs by one of several mechanisms | 1- Mutation that alter a 50S ribosomal binding-site 2- ↓Bacterial uptake of Macrolide→↓ Macrolide accumulation mediated by active efflux pump 3- Enzymatic inactivation of the Macrolides |
| Efflux & methylase production are the most important resistance mechanisms in | Gram+Ve organisms] |
| Resistance Macrolides | |
| - Complete cross-resistance between Erythromycin & the other Macrolides | Bacteria that have developed resistance to Erythromycin are usually resistant to the newer Macrolides |
| Partial cross-resistance | resistance to structurally unrelated Macrolides such as Clindamycin & StreptograminB →which share the same ribosomal binding site |
| Antibacterial spectrum of activity of Telithromycin,Clarithromycin & Azithromycin | 1- effective against aerobic Gram+ve organisms Gram+ve cocci: Streptococcus > Staph.aureus Gram +ve bacilli: C.diphtheriae, B.anthracis |
| Antibacterial spectrum of activity of Telithromycin,Clarithromycin & Azithromycin | 2- Atypical bacteria:As → Chlamydia, Mycoplasma, Rickettisae 3-few Gram -ve organisms: |
| Some/few Gram -ve organisms | Gram-ve cocci: as Moraxella catarrhalis Gram-ve bacilli: as → H.influenzae, B.pertussis , & Campylobacter jejuni causes → Traveler’s diarrhea treated by → Azithromycin H.Pylori causes →GI ulcer treated by→ Clarithromycin |
| Ketolides: As Telithromycin orally | -effective against many Macrolide -resistant Gram+ve organisms -it binds to 2 sites of contact instead of one on the 50S ribosome -poor substrate for bacterial efflux pumps |
| Telithromycin is active against many | strains of Strepto. pneumoniae, Strepto. pyogenes &Staph.aureus that are resistant to Macrolides |
| Teilthromycin is limited by | severe hepatotoxicity |
| antimicrobial spectrum of Teilthromycin | |
| Therapeutic uses of Erythromycin | MLCDPSS (mnemonics) |
| Therapeutic uses of Azithromycin | MLCDPSS + MAC + LGV + H.influenzae |
| Therapeutic uses of Clarithromycin | MLCDPSS + MAC + M. leprae + H.pylori |
| Therapeutic uses of Macrolide | |
| Older-generation (Erythromycin) | -has a similar spectrum of activity to PenicillinG -alternative drug to treat Penicillin-sensitive infections in Penicillin-allergic patients |
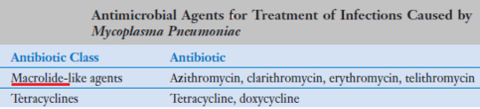
| MLCDPSS | Mycoplasma pneumoniae Legionnaire’s pneumonia Chlamydia pneumoniae Diphtheria Pertussis Staphylococcal & Streptococcal infections Syphilis |
| Mycoplasma pneumoniae | |
| Legionnaire’s pneumonia | Azithromycin is the DOC |
| Chlamydia pneumoniae | |
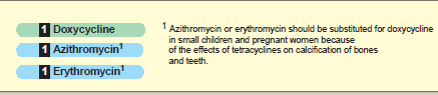
| : Macrolides in Chlamydia pneumoniae | preferred for 1- initial uncomplicated Chlamydial infections 2-for Chlamydial infections in children & pregnant women |
| Tetracyclines in Chlamydia pneumoniae | preferred for recurrent infections |
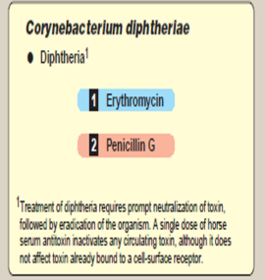
| Diphtheria Macrolide (Erythromycin) is very effective for eliminating the carrier state | |
| Pertussis (Whooping cough) caused by Bordetella pertussis | Macrolides (Erythromycin) is most effective treatment as well as for prophylaxis of close contacts |
| “alternative” in patient who are allergic to PenicillinG | -Staphylococcal infections in mild cases (but not MRSA strains) -Streptococcal infections:→ URTIs - Syphilis caused by Trepenoma pallidum |
| Macrolides good for!!! | 1-Atypical bacterial infection -- Upper & lower RTI Atypical-CAP 2-Traveler’s diarrhea (Azithromycin) 3- Clarithromycin is a key component in the treatment of H. pylori 4-Atypical mycobacterial infections |
| URTIs | |
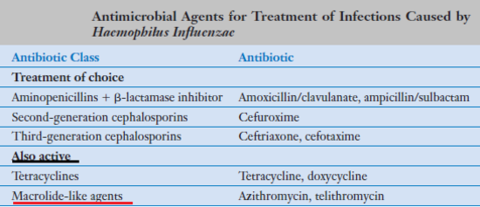
| TX of H. influenza | |
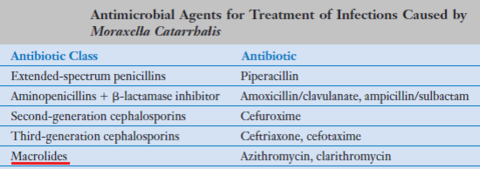
| TX of M. catarehalis | |
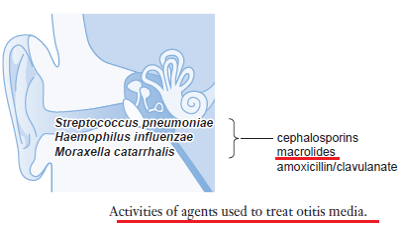
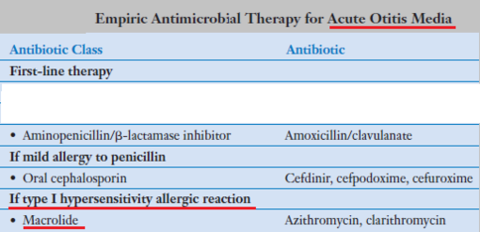
| Empiric Tx Acute otitis media | |
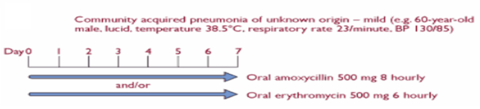
| Empiric Tx CAP | |
| Q- A 54- year-old man with no significant past medical history who presents with CAP of mild-moderate severity. He is probably allergic to Penicillin | |
| A 27-year-old pregnant patient with a history of pyelonephritis has developed a severe upper respiratory infection that appears to be due to a bacterial pathogen. The woman is hospitalized. Which Macrolide is to be selected for treatment! | ddd |
| Antimicrobial drugs that are eliminated via hepatic metabolism or biliary excretion include | erythromycin, cefoperazone, clindamycin, doxycycline, isoniazid, ketoconazole, and nafcillin |
| pseudomembranous colitis has been associated with the use of many agents including ؟؟ | ampicillin and clindamycin |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.