7678221
Description
Flashcards by brittny beauford, updated more than 1 year ago
|
|
Created by brittny beauford
almost 9 years ago
|
|
| Question | Answer |
| The heart is the engine of the body, it is_________ and___________. | electrical mechanical |
| Cardiac cells are electrically negative at rest. ____IN and_____OUT | K+ Na++ |
| Movement of sodium and potassium in and out of the cells cause changes that can be picked up on the ______ by electrodes and translated to the ECG printout. | skin |
| When the cell is stimulated by an electrical impulse,________ rushes into the cell and____________ leaks out. This causes cell to become positively charged, this is referred to as_________! Contraction follows. | sodium potassium DEPOLARIZATION |
| During cell recovery, the sodium-potassium pump returns cell to it’s negative charge. This is____________! Muscle relaxation follows. | REPOLARIZATION |
| #1 SA Node=___-__ beats per minute | 60-80 |
| #2 _____=40-60 BMP | AV node |
| #3____,_____, & _______=20-40 BPM | HIS, Bundle Branches & Purkinje |
| Cardiac Intervals One small box=_____ seconds One large box=_____ seconds 5 large boxes=_____ seconds | 0.04 seconds .20 seconds 1 second |
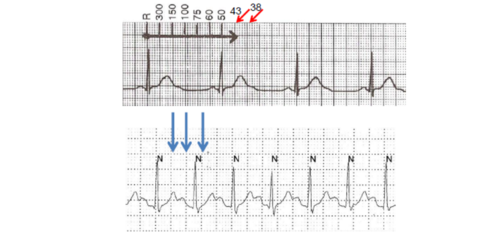
| reference for counting | |
| PR interval – time for electrical impulse to get from _______ to the _________, <0.20 seconds (5 small or 1 large boxes) | atria ventricles |
| _____ interval – measures the time it takes to depolarize the ventricles, < 0.12 seconds (3 small boxes) | QRS interval <0.12 seconds is mentioned twice in the powerpoint and .04-.10 seconds is mentioned once |
| QT interval – measures depolarization and repolarization time of the ventricles. Measured from the beginning of the QRS to the end of the T-wave. Should be less than one half the R – R interval. If prolonged can lead to ____________. Usually 0.36 - 0.44 seconds (9 – 11 little boxes) Lead 2 or V5 – 6 best place to measure. | lethal dysrhythmias |
| Indicates atrial depolarization, or contraction of the atrium. The P wave can have any shape, up, down, or biphasic, as long as it is consistent | P wave |
| Indicates AV node conduction time Duration time is 0.12 to 0.20 seconds | PR segment |
| Indicates ventricular depolarization, or contraction of the ventricles. Interval is .04-.10 seconds or <0.12 seconds | QRS interval <0.12 seconds is mentioned twice in the powerpoint and .04-.10 seconds is mentioned once |
| Indicated ventricular repolarization. Or the ventricles at rest Rounded and asymmetrical | T wave |
| Questions to consider with an EKG | Is it regular or irregular? Is there a P wave? Is there a P wave for every QRS? What is the rate ? Is the QRS wide or normal ? |
| Sinus tachycardia (100 and above) | |
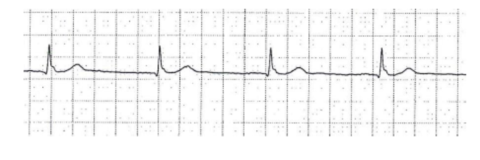
| Sinus rhythm (60-99) | |
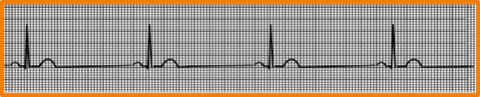
| Sinus brady (59 and below ) | |
| supraventricular tachycardia (don't need to know) *In class we pretend this is sinus tach even though there is no P wave and it breaks all there rules grrrrr | |
| Atrial fibrilaiton (irregularly irregular with no discernible P wave) If rate is irregular, must calculate by range Ex. this pt is 55-90 (shorts and longest range) | |
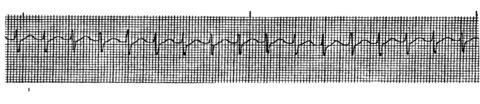
| atrial flutter (sawtooth or shark tooth) | |
| Rate control: just because its upside down doesn't mean it doesn't count *cool story bro | |
| 3 treatments of A-Fib | PREVENTINO OF BLOOD CLOTS: ASA, Warfarin. NOACS-Pradaxa, Xarelto, Eliquis HEART RATE CONTROL: Beta Blockers HEART RHYTHM CONTROL: Sodium Channel Blockers (Flecanide, Quinidine) Potassium Channel Blockers (Amiodarone, Sotalol) |
| Rest period before heart get ready to beat again | Depolarization |
| Premature atrial contraction (don't need to know) *in class we pretend this is sinus rhythm with a rate even though its not regular once again grrrr | |
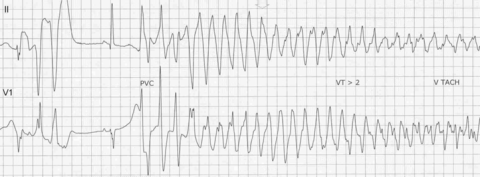
| PVC (an ecotype we don't need to know) | |
| PVC (an ecotype we don't need to know) | |
| A sinus rhythm must be/have what? | A QRS wave and regular |
| (lethal ventricular rhythms) | |
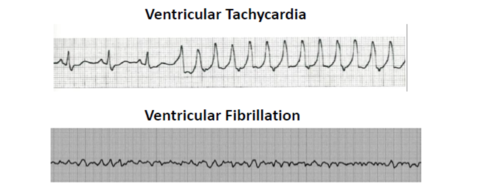
| Ventricular tachycardia (lethal ventricular rhythms) | |
| torsades de pointe | |
| ventricular fibrillation (lethal ventricular rhythms) | |
| Treatment of VT or V-Fib | Assess patient NOT monitor. Pulse? LOC? VS? CPR, O2, IV, defib/pacer pads Cardioversion: Stable Defibrillate: Symptomatic Rx: Epi, vasopressin, amiodarone, (Lidocaine, old school) |
| Torsades can occur when magnesium is depeleated | |
| Long QT syndrome Risk factors? | Torsades de Pointes Risk factors: Medications, women 2x > men, >65 y/o, Heart Dx, Diuretics, Renal or Hepatic dysfunction, Electrolytes abnorms, Bradycardia, |
| Treatment Collaborative Care for Torsades | STOP CAUSATIVE MEDS Synchronized Cardioversion IV Magnesium (for who?), Potassium, Amiodarone IAD |
| Education Collaborative Care for Torsades | Medications to avoid and those to take Seek care immediately for syncope BLS training for family, consider AED (enter defibrilatior) |
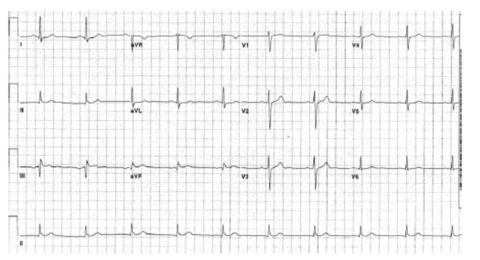
| Benefits of multiple leads | |
| What is this? | Point is sometimes you need more then one lead |
| What is this? | ? |
| TEST QUESITON Cardioversion and defribilation | BOTH SHOCK Defibrilaiton-push button pads go, it will go no matter what when you push button cardioversion synchronized- goes specifically when a pattern is recognized. *Used during Vtach if conscious and unsymtomatic |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.