859369
Description
Flashcards by sophietevans, updated more than 1 year ago
|
|
Created by sophietevans
almost 10 years ago
|
|
| Question | Answer |
| The kidney maintains: volume of plasma concentrations of electrolytes pH within physiological range Achieved by varying amounts of water and salts excreted. Excretes waste products (e.g. urea, creatinine and urobilinogen) What proportion of the body's ATP does it use for all of these functions? | ~16% |
| What is the lifespan of an erythrocyte? | ~120 days |
| Which organs/tissues are included in the reticuloendothelial system (extravascular system in which macrophages phagocytose erythrocytes and recycle iron)? | Bone marrow, liver, and spleen. |
| Briefly describe the breakdown of haem from erythrocytes. | Haem → iron → protoporphyrin → bilirubin → conjugated bilirubin in the liver by UDP glucuronyl transferase → bilirubin glucuronides are transformed into stercobilinogen in the colon → majority of stercobilinogen is excreted in faeces, some is reabsorbed → that which is reabsorbed is converted to urobilinogen (solubilised) and excreted in the urine. |
| Intravascular haemolysis plays little role in normal erythrocyte destruction as erythrocyte metabolism and iron recycling occurs in the extravascular reticuloendothelial system. Which diseases is intravascular haemolysis associated with? | Haemolytic anaemias. |
| Macrophages are not really involved in intravascular haemolysis. Which blood components bind to erythrocytes and result in their lysis? | Complement and/or haptoglobin. |
| Haemolytic anaemias are characterised by an increased rate of erythrocyte destruction. What clinical feature might result if there is too much erythrocyte destruction (not anaemia...)? | Haematuria. |
| What is methaemalbumin? | Albumin with haemoglobin bound to it. |
| What is haemosiderinuria? | An accumulation of iron in the kidneys which causes damage. |
| In haemolytic anaemias, is erythrocyte destruction intravascular or extravascular? | It can be either, but tends to be intravascular. |
| How might anaemias be 'masked'? | Compensation by the bone marrow tends to occur - that which is not usually haemopoietically active is activated and haemopoiesis increases 6-8x. |
| Defects in erythrocytes which result in their premature destruction are usually inherited. List three conditions in which erythrocytes are defective and which may result in haemolytic anaemias. | Spherocytosis (membrane defect, or elliptocytosis), pyruvate kinase deficiency (metabolic defect), and thalassaemia (haemoglobin defect). |
| Why do erythrocytes only have the haemoglobin/enzymes that they start their lifespan with? | Because they don't have any organelles (they are not nucleated) so they cannot produce more. |
| List some acquired causes of haemolytic anaemias. | Immune e.g. antibodies (e.g. alloimmune blood transfusion resulting in antibody production) ◦ Red cell fragmentation syndromes e.g. cardiac valve ◦ Infections e.g. malaria ◦ Chemical e.g. drugs, exposure to chemicals ◦ Secondary due to liver or renal disease (which frequently have systemic effects) |
| Haemolytic transfusion reactions are reactions to 'foreign' blood with previously 'unseen' antigens in which there is increased haemolysis. This breakdown may be intravascular or extravascular - what does this depend on? | The antibodies/immune cells involved. For instance, if anti-ABO antibodies are involved, complement is activated via the classical pathway as immune complexes interact with the C1q complex, resulting in lysis/rupture of the erythrocytes within the vessels and release of haem into the plasma. Other blood systems (anti-Rh, anti-MNS, anti-Li, anti-KEL) only activate complement up to C3 or don't activate it at all, so MAC does not form. Instead, they are phagocytosed by macrophages in the extravascular reticuloendothelial system and extra bilirubin is released into the plasma rather than extra haem. |
| What are the signs of a haemolytic tranfusion reaction? What is the timescale? | There is a lot of haem or bilirubin in the plasma (depending on whether the haemolysis is intravascular or extravascular based on the antibodies involved) so the faeces will be red/black and there will likely be haematuria/haemosiderinuria. It is an immune response so there is an increase in heart rate and a fever, as well as vomiting. |
| In fatal cases of haemolytic transfusion reactions, death may result from disseminated intravascular coagulation (DIC) and associated hypotension, or from acute renal failure. What is the basic pathogenesis of DIC? | Lots of microthrombi form throughout the vessels, using up all the platelets so that none are available for wound healing - this can result in severe haemorrhage. The thrombi themselves can cause tissue ischaemia by blocking small blood vessels. |
| Which hormone does the kidney produce to regulate erythropoiesis? | Erythropoietin. |
| What about the bone marrow might affect erythropoiesis, resulting in anaemia? | Whether or not it has room and/or stem cells to produce erythrocytes. If the bone marrow is taken over by useless cells in leukaemia, for instance, there may not be room for myeloid progenitors to differentiate, whereas if haemopoietic stem cells are not being produced, myeloid progenitors will not even be produced. |
| Which nutrients are critical for erythrocyte formation? | Vitamin B12 and folate (as well as iron) - deficiencies in these can result in nutritional anaemias. |
| How can respiratory dysfunction result in anaemia even if Hb concentration is fine? | Anaemia refers to the oxygen carrying capacity of the blood - this IS reduced if there is less O2 available to be carried, even if the hypoxia detected by the kidneys results in the production of more erythropoietin and the formation of more erythrocytes. |
| Erythropoietin production increases in anaemia. Describe some other situations in which it will increase. | When atmospheric O2 is low (i.e. high altitudes); when Hb is unable to give up O2 (metabolic/structural region); or when defective cardiac or pulmonary function, or damage to renal circulation affects O2 delivery to the kidney. |
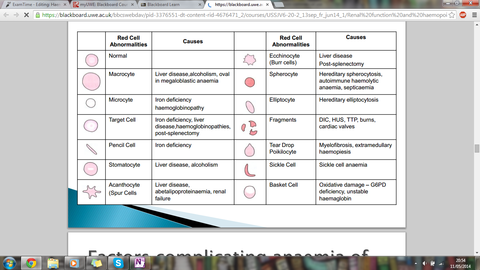
| Renal failure can affect EPO production, resulting in impaired erythrocyte production and a normochromic anaemia. What factor in the serum may result in the formation of 'spur' and 'burr' cells? Why? | Uraemia. Uraemic serum contains factors which inhibit proliferation of erythroid progenitors, so in severe uraemia erythrocytes show abnormalities, such as 'spur' and 'burr' cells. |
| What is a Burr cell technically called? And a spur cell? | Burr cell = ecchinocyte. Spur cell = acanthocyte. |
| Here are some erythrocyte structural abnormalities and their causes. | |
| There are other factors affecting the anaemia caused by dialysis in chronic renal failure. What do these include? | Iron deficiency from blood loss during dialysis Folate deficiency in some chronic dialysis patients (folate loss during dialysis) Aluminium excess in patients on chronic dialysis inhibits erythropoiesis (aluminium used to be in the phosphate binders used to treat bone disease associated with kidney disease but is seen less now as it suppresses marrow function) |
| What is the basic process by which thrombopoiesis is increased? | If you don't have many thrombocytes, the thrombopoietin produced by your kidneys and liver will not bind to many of them (they have receptors for it), and will return to the bone marrow, where it stimulates platelet production in the bone marrow. |
| As well as producing erythropoietin and a small proportion of thrombopoietin, what other hormone do they kidneys produce? | Renin. |
| Renin controls blood pressure through the renin-angiotensin system. How? | Juxtoglomerular cells detect decreased blood pressure via hypotension or decreased Na+ delivery to tissue, or are stimulated sympathetically, and they release renin which is then able to convert constitutive pro-enzyme angiotensinogen into angiotensin I. Angiotensin-converting enzyme then converts it to angiotensin II which acts on the adrenal medulla to cause more production and release of aldosterone. Aldosterone acts on the distal convoluted tubule to increase Na+ reabsorption and thus H2O reabsorption, and this water retention increases blood pressure. This increase in BP negatively feeds back to the kidneys to reduce renin production. |
| So kidney disease can cause haem problems (e.g. reduced EPO production) but haem can cause kidney problems too - namely disturbances in cell differentiation in the bone marrow, such as multiple myeloma. How does this result in kidney disease? | There is clonal proliferation of plasma cells and production of vast amounts of identical antibody which forms complexes which get stuck in the glomeruli - glomerulonephritis/type III hypersensitivity reaction. |
| Multiple myeloma (MM) is a neoplastic proliferation of plasma cells in the bone marrow, resulting in their accumulation as well as presence of monoclonal protein (antibody molecules and/or free light chains) in serum and urine as malignant plasma cells have clonally re-arranged Ig genes and secrete excess paraprotein. Why are IL-6 and osteoclast activating factor (OAF) significant in multiple myeloma? | IL-6 is a potent haematopoietic growth factor in multiple myeloma (probably via an autocrine mechanism), while OAF is secreted by MM cells and results in the painful bone lesions seen in MM. |
| What do multiple myeloma plasma cells and the Philosopher's stone have in common? | Immortality - the MM cells do not die so they accumulate in the bone marrow and replace normal cells, meaning that there is suppression of normal bone marrow function, including anaemia. |
| List some of the clinical features of multiple myeloma. | Hyperviscosity of the blood due to the large numbers of monoclonal antibodies. 'MYELOMA KIDNEY' - around 1/4 of people presenting with early multiple myeloma symptoms have severe renal damage and fibrosis, which can cause complete renal failure. There are proteinaceous deposits in the kidney, and the inflammatory damage from this results in hyperuricaemia and hypercalcaemia. Anaemia results from decreased erythroid production, both as a result of bone marrow impairment and renal damage resulting in less EPO produced. Cryoglobulinaemia: all the protein in the blood means that at low temperatures, these complexes can precipitate. Clotting and bleeding problems: antibodies 'get in the way of' platelets, which in turn are dysfunctional due to reduced TPO production and bone marrow impairment. |
| Why is there an increased infection risk in multiple myeloma? | Despite the fact that tonnes of antibody is being produced, it is all useless (irony). There is neutropenia (reduced innate response) and B cell class switching is not possible because only immature plasma cells are produced, resulting in monoclonal antibody production. This means neither the innate nor the acquired immune response is functioning fully, leaving patients with MM vulnerable to more infections. |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.