7957366
Description
Mind Map by ladan kite, updated more than 1 year ago
|
|
Created by ladan kite
about 9 years ago
|
|
Primary Angle-Closure Glaucoma
- group of disorders characterized by high intracular
pressure
- GLAUCOMA
- Primary Open -Angled Glaucoma
- Primary Angle-Closure Glaucoma
- OCULAR EMERGENCY
- requires immediate management to avoid blindness
- (Weinreb, Aung, Medeiros, 2014)
- (Weinreb, Aung, Medeiros, 2014)
- requires immediate management to avoid blindness
- OCULAR EMERGENCY
- Primary Open -Angled Glaucoma
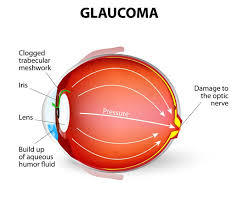
- consequences of elevated pressure
- optic nerve atrophy
- peripheral visual field
loss
- (Smith and Neely, 2014, p.520)
- (Smith and Neely, 2014, p.520)
- peripheral visual field
loss
- optic nerve atrophy
- GLAUCOMA
- EPIDEMIOLOGY
- In 2013, the number of
people of from agse 40-80
with PACG was 20.17 M
and is expected to
increase to 32.04 M in 2040
- Highest rates: Inuit, and other
Asian population
- (Marchini, Chemello, Berzaghi & Zampieri, 2015)
;Sun etal, 2016
- (Marchini, Chemello, Berzaghi & Zampieri, 2015)
;Sun etal, 2016
- Common in women,
female:male is 2:1
- Caucasians: 0.1-0.6%,
Inuits: 2.6-6.2%,
Asians: 0.3-3%
- In 2013, the number of
people of from agse 40-80
with PACG was 20.17 M
and is expected to
increase to 32.04 M in 2040
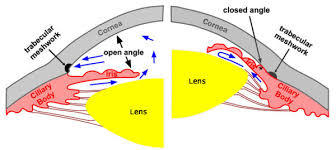
- PATHOPHYSIOLOGY
- Aqueous humor
- produced in posterior
chamber
- flows into anterior chamber through
pupil
- aqueous humor drains in
trabecular meshwork
- ( Marchini, Chemello, Berzaghi & Zampieri, 2015; Weinreb, Aung, Medeiros,
2014)
- ( Marchini, Chemello, Berzaghi & Zampieri, 2015; Weinreb, Aung, Medeiros,
2014)
- "Pupillary block"
- aqueous humor outflow
blocked
- increased intro-ocular
pressure
- SIGNS AND SYMPTOMS
- Red painful eyes
- Nausea and
vomiting
- Haloes around lights
- Haloes around lights
- Blurry
vision
- Headache
- Cornea edema
- Hazy
cornea
- Photophobia
- Pupil midilated and non-reactive
- (Marchini, Chemello, Berzaghi & Zampieri, 2015; Weinreb, Aung, Medeiros, 2014)
- (Marchini, Chemello, Berzaghi & Zampieri, 2015; Weinreb, Aung, Medeiros, 2014)
- Pupil midilated and non-reactive
- Photophobia
- Red painful eyes
- SIGNS AND SYMPTOMS
- Anterior chamber is narrow
- iris is pushed forward
- iris covers trabecular
meshwork
- iris covers trabecular
meshwork
- iris is pushed forward
- aqueous humor outflow
blocked
- aqueous humor drains in
trabecular meshwork
- flows into anterior chamber through
pupil
- produced in posterior
chamber
- Aqueous humor
- DIAGNOSTICS
- Gonioscopy
- most important diagnostic
method for assessing the
presence of angle closure
- most important diagnostic
method for assessing the
presence of angle closure
- The van Herick angle
- used to screen for the depth of the anterior
chamber angle prior to dilation
- used to screen for the depth of the anterior
chamber angle prior to dilation
- Penlight shadow test
- screening method for assessing anterior
chamber depth and iris convexity
- (Anwar & Turalba, 2017; Jackson et al,
1997)
- (Anwar & Turalba, 2017; Jackson et al,
1997)
- screening method for assessing anterior
chamber depth and iris convexity
- patient History
- family history of primary ACG.
- S/S of attacks
- family history of primary ACG.
- Normal IOP : 10-21 mmHG
- Angle closure IOP : >50 mmHG
- (Smith and Neely, 2014,)
- (Smith and Neely, 2014,)
- Angle closure IOP : >50 mmHG
- Gonioscopy
- Client- Centred-Care
- Use touch if appropriate to offer reassurance to the person
- Be reassuring when they
are expressing their fears
- (RNAO, 2015)
- (RNAO, 2015)
- Encourage the person to voice any questions
they may have about their health needs and
care.
- Use touch if appropriate to offer reassurance to the person
- PHARMOLOGICAL
- Drugs
- Indication
- will decrease formation of
aqueous humor, as well as
decrease the posterior–anterior
chamber pressure gradient
- works by constricting the
pupil and removing the iris
from the trabecular region.
- (Marchini, Chemello, Berzaghi & Zampieri, 2015; Anwar & Turalba,
2016)
- (Marchini, Chemello, Berzaghi & Zampieri, 2015; Anwar & Turalba,
2016)
- works by constricting the
pupil and removing the iris
from the trabecular region.
- will decrease formation of
aqueous humor, as well as
decrease the posterior–anterior
chamber pressure gradient
- Aqueous
suppressants
- Alpha Agonist, Carbonic
anhydrase inhibitors, and
Adrengeric antogonists,
- Micotics
- pilocarpine
dapriprazole
- pilocarpine
dapriprazole
- Micotics
- Alpha Agonist, Carbonic
anhydrase inhibitors, and
Adrengeric antogonists,
- Indication
- topical, oral, and intravenous agents
- GOALS
- Performance of laser peripheral iridotomy or
surgical iridectomy
- (Jackson et al,
1997)
- (Jackson et al,
1997)
- Evaluation of treatment
- Relief of the attack and avoiding vision loss using medical
therapy, laser therapy, or surgery
- Performance of laser peripheral iridotomy or
surgical iridectomy
- Drugs
- HEALTH PROMOTION
- eye exam every
3-5 years until
40 yrs and
every 2-4 years
until 65 yrs
- older adults should
have an eye exam
every two years
- eye exam yearly for
people of african
descent and those
with a history of
glaucoma
- (Smith and Neely, 2014, p.524)
- eye exam every
3-5 years until
40 yrs and
every 2-4 years
until 65 yrs
- NON PHARMOLOGICAL
- Patient may feel
uncomfortable
- providing a quiet and private
space
- applying cool compreses to the
patients forhead
- darkening the environment
- Reduce safety
hazards
- reducing clutter
- (Smith and Neely, 2014)
- providing a quiet and private
space
- Patient may feel
uncomfortable
- RISK FACTORS
- Older age
- female sex
- Asian ethnicities
- shorter axial length
- shorter axial length
- dense iris volume
- increase choroidal thickness
- (Marchini, Chemello, Berzaghi & Zampieri, 2015; Anwar & Turalba 2017)
- Older age
- SURGERY
- Laser Iridotomy
- heals pupil block
- for patients with narrow angles
- allows aqueous humor to flow in a new opening
- for patients with narrow angles
- preventative measure against an acute
attack
- if acute attack occurs,iridotomy must
be done immediately
- heals pupil block
- Laser Iridoplasty
- the iris is thick, so the laser will burn reduce
the thickness of it
- the iris becomes smaller and is detached from
the trabecular meshwork
- the angle is wide and the IOP
decreases
- (Sun et al, 2016; Anwar & Turalba 2017 ; Marchini, Chemello, Berzaghi & Zampieri, 2015
- (Sun et al, 2016; Anwar & Turalba 2017 ; Marchini, Chemello, Berzaghi & Zampieri, 2015
- the angle is wide and the IOP
decreases
- the iris becomes smaller and is detached from
the trabecular meshwork
- iridoplasty done when iridotomy fails
- the iris is thick, so the laser will burn reduce
the thickness of it
- Laser Iridotomy
- COLLABORATIVE CARE
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.