12635845
Beschreibung
Mindmap von Natasha Sharp, aktualisiert more than 1 year ago
|
|
Erstellt von Natasha Sharp
vor etwa 6 Jahre
|
|
Acute Kidney
Injury (AKI)
- RIFLE Classification for Staging AKI
- Risk
- Serum creatinine increased x1.5 or
GFR decreased by 25%, with urine
output <0.5ml/kg/hr for 6hrs
(Beeman & Emerson, 2013).
- Serum creatinine increased x1.5 or
GFR decreased by 25%, with urine
output <0.5ml/kg/hr for 6hrs
(Beeman & Emerson, 2013).
- Injury
- Serum creatinine increased x2 or GFR decreased by
50%, with urine output <0.5ml/kg/hr for 12hrs
(Beeman & Emerson, 2013).
- Serum creatinine increased x2 or GFR decreased by
50%, with urine output <0.5ml/kg/hr for 12hrs
(Beeman & Emerson, 2013).
- Failure
- Serum creatinine increased x3 or GFR decreased
by 75% or serum creatinine >4mg/dl with acute
rise >0.5mg/dl, with urine output <0.3ml/kg/hr
or anuria for 12hrs (Beeman & Emerson, 2013).
- Serum creatinine increased x3 or GFR decreased
by 75% or serum creatinine >4mg/dl with acute
rise >0.5mg/dl, with urine output <0.3ml/kg/hr
or anuria for 12hrs (Beeman & Emerson, 2013).
- Loss
- Persistent acute kidney failure; complete loss of
kidney function>4 weeks (Beeman & Emerson, 2013).
- Persistent acute kidney failure; complete loss of
kidney function>4 weeks (Beeman & Emerson, 2013).
- End-stage kidney
disease
- Complete loss of kidney
function >3 months
(Beeman & Emerson,
2013).
- Complete loss of kidney
function >3 months
(Beeman & Emerson,
2013).
- Risk
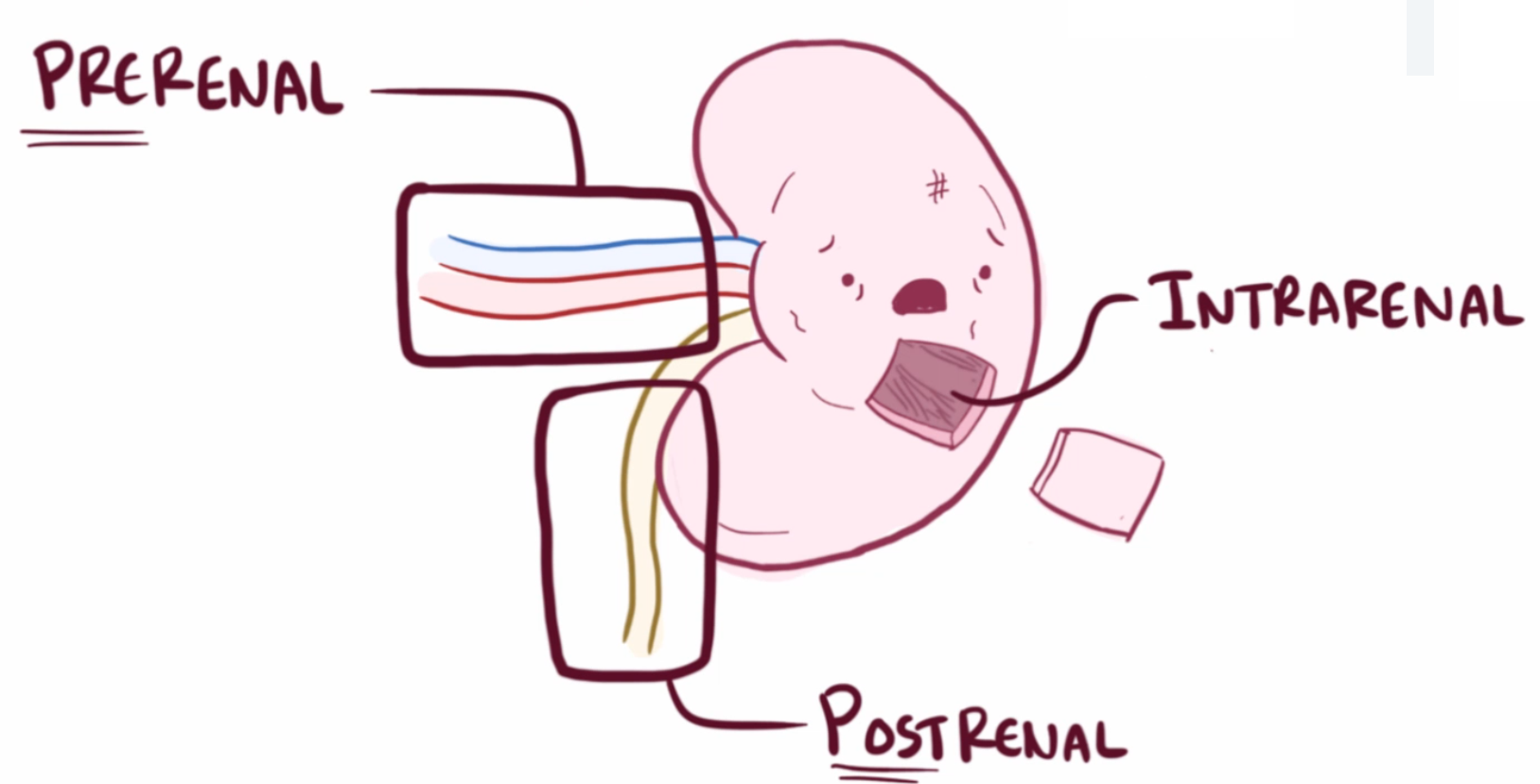
- Types of Acute Kidney
Injury
- Prerenal
- Absolute decrease in circulating
volume, which can be causes by
hemorrhage, dehydration or burns
(Beeman & Emerson, 2013).
- Relative decrease in circulating volume, which
can be caused by distributive shock,
third-spacing, deem, and decreased cardiac
output.
- Eventually leading to cariogenic shock, dysrhythmias, cardiac tamponde,
heart failure and myocardial infarction (Beeman & Emerson, 2013).
- Eventually leading to cariogenic shock, dysrhythmias, cardiac tamponde,
heart failure and myocardial infarction (Beeman & Emerson, 2013).
- Primary renal hemodynamic
abnormalities due to drug-induced
impairment of renal auto regulation or
occlusion or stenosis of the renal artery
(Beeman & Emerson, 2013).
- Absolute decrease in circulating
volume, which can be causes by
hemorrhage, dehydration or burns
(Beeman & Emerson, 2013).
- Postrenal
- Caused by kinked or obstructed
catheters, benign prostatic
hyperplasia, strictures, or
intraabdominal tumours
(Beeman & Emerson, 2013).
- Caused by kinked or obstructed
catheters, benign prostatic
hyperplasia, strictures, or
intraabdominal tumours
(Beeman & Emerson, 2013).
- Intrarenal/Intrinsic
- Tubular (acute tubular
necrosis)
- Ischemic
- Typically caused by prolonged prerenal failure,
transfusion reactions, and rhabdomyolysis
(Beeman & Emerson, 2013).
- Typically caused by prolonged prerenal failure,
transfusion reactions, and rhabdomyolysis
(Beeman & Emerson, 2013).
- Nephrotoxic
- Certain antimicrobials, prolonged post-renal failure,
radiographic contrast media, recreational drugs,
environmental agents, and snake/insect venom possess
neprotoxic affects (Beeman & Emerson, 2013).
- Certain antimicrobials, prolonged post-renal failure,
radiographic contrast media, recreational drugs,
environmental agents, and snake/insect venom possess
neprotoxic affects (Beeman & Emerson, 2013).
- Ischemic
- Glomerular
- Acute
glomerulonephritis
- Acute
glomerulonephritis
- Interstitial
- Acute pyelonephritis and/or acute allergic
interstitial nephritis affect the interstitial portion
of the kidney (Beeman & Emerson, 2013).
- Acute pyelonephritis and/or acute allergic
interstitial nephritis affect the interstitial portion
of the kidney (Beeman & Emerson, 2013).
- Vascular
- Caused by vasculitis or an emboli
(Beeman & Emerson, 2013).
- Caused by vasculitis or an emboli
(Beeman & Emerson, 2013).
- Tubular (acute tubular
necrosis)
- Prerenal
- Pathophysiology
- Haemodynamic
Instability
- Association between the time spent in relative
hypotension and the development of AKI in
patients with sepsis was shown in the FINNAKI
study (Ostermann & Liu, 2017).
- Asfar and colleagues discovered that
patients with chronic hypertension,
prevented the development of severe AKI
during sepsis (Ostermann & Liu, 2017).
- Many studies found that within the perioperative
setting, there is a link between intraoperative
hypotension and the development of
postoperative AKI (Ostermann & Liu, 2017).
- Association between the time spent in relative
hypotension and the development of AKI in
patients with sepsis was shown in the FINNAKI
study (Ostermann & Liu, 2017).
- Inflammation
- Inflammation and the need for leukocytes are key
mediators of all phases of endothelial and tubular
cell injury within the invitation and maintenance
phase of AKI (Ostermann & Liu, 2017).
- As soon as a endothelial or tubular epithelial cell injury
occurs, an immune response is triggered. It consists of
activation of inflammatory cells and recruitment and
invasion of WBCs (Ostermann & Liu, 2017).
- Basically all immune
cells are involved in
these pathophysiological
processes of AKI
(Ostermann & Liu, 2017).
- Basically all immune
cells are involved in
these pathophysiological
processes of AKI
(Ostermann & Liu, 2017).
- Systematic inflammation can contribute to the pathogenesis of AKI
- for example, elevated levels of interleukin 6 have been linked to
the development of AKI, cardiac surgery, and severely ill patients
with acute respiratory distress (Ostermann & Liu, 2017).
- Inflammation and the need for leukocytes are key
mediators of all phases of endothelial and tubular
cell injury within the invitation and maintenance
phase of AKI (Ostermann & Liu, 2017).
- Tubular Cell
Injury
- Microcirculatory dysfunction results in tubular cell injury as well as
direct exposure to substances in the filtrate (Ostermann & Liu, 2017).
- Structural changes such as: apical membrane blabbing,
opening of tight junctions, loss of polarity, cell
detachment from the basement membrane and cell
swelling are all manifestations of tubular cell injury
(Ostermann & Liu, 2017).
- Damage to the mitochondria may also occur, an increase in
mitochondrial fragmentation encourages the excess production of
ROS, release of cytokines and cellular death. All contributing to the
further progression of AKI, therefore, tubular cells have a diverse role
in AKI (Ostermann & Liu, 2017).
- Damage to the mitochondria may also occur, an increase in
mitochondrial fragmentation encourages the excess production of
ROS, release of cytokines and cellular death. All contributing to the
further progression of AKI, therefore, tubular cells have a diverse role
in AKI (Ostermann & Liu, 2017).
- Microcirculatory dysfunction results in tubular cell injury as well as
direct exposure to substances in the filtrate (Ostermann & Liu, 2017).
- Renal
Venous
Congestion
- Tubular
Obstruction
- Auto-Immune
Processes
- Hypersensitivity
Immune
Reaction
- Haemodynamic
Instability
- Collaborative
Care
- Diagnostic
- Requires treatment of the precipitating cause, fluid
restriction, nutritional therapy, calcium
supplements or phosphate-binding agents,
initiation of renal replacement therapy, and total
parenteral nutrition if indicated (Wood, 2014).
- Nutritional therapy involves potassium, phosphate,
and sodium restrictions with adequate amounts of
protein (Wood, 2014).
- Nutritional therapy involves potassium, phosphate,
and sodium restrictions with adequate amounts of
protein (Wood, 2014).
- Requires treatment of the precipitating cause, fluid
restriction, nutritional therapy, calcium
supplements or phosphate-binding agents,
initiation of renal replacement therapy, and total
parenteral nutrition if indicated (Wood, 2014).
- Collaborative
Therapy
- Involves a history and physical exam, identification of
precipitating causes, serum creatinine and BUN levels, serum
electrolytes, a urinalysis, renal ultrasound, renal scans, CT
scans, and retrograde pyelogram if indicated (Wood, 2014).
- Involves a history and physical exam, identification of
precipitating causes, serum creatinine and BUN levels, serum
electrolytes, a urinalysis, renal ultrasound, renal scans, CT
scans, and retrograde pyelogram if indicated (Wood, 2014).
- Diagnostic
- Etiology
- Risk factors
- Comorbidities such as, aging population, diabetes,
chronic kidney disease, COPD, heart failure
(Meersch, Volmering, & Zarbock, (2017).
- Acute medical conditions such as, sepsis,
major surgery, hemodynamic instability, and
mechanical ventilation (Meersch et al., 2017).
- Comorbidities such as, aging population, diabetes,
chronic kidney disease, COPD, heart failure
(Meersch, Volmering, & Zarbock, (2017).
- Most often nephrotoxic
drugs are the cause of
AKI (Meersch et al.,
2017).
- Surgical/interventional
measures related to AKI
development
- Inotropic support, vasopressors, aortic
cross-clamping, selective renal ischemia,
bleeding complications, and transfusion
of blood products (Meersch et al., 2017).
- Inotropic support, vasopressors, aortic
cross-clamping, selective renal ischemia,
bleeding complications, and transfusion
of blood products (Meersch et al., 2017).
- Risk factors
- By Natasha Sharp
Medienanhänge
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.