10388440
| Question | Answer |
| The Frank-Starling mechanism suggests that, within physiological limits, the more distension the heart experiences at end diastole, the ________ volume it is able to pump out. | More |
| Which factors will affect the Frank-starling mechanism? | 1. Venous return (input) 2. Peripheral resistance 3. Cardiac nutrition 4. Cardiac calcium |
| In a failing heart, the SV - end diastolic volume curve will be (higher/lower) than the normal heart. | Lower. |
| T/F: A failing heart does NOT adhere to the frank-starling law. | F. It still does. |
| Which conditions can increase preload of the heart? | 1. hypervolemia (too much blood) 2. regurgitation of cardiac valves 3. Heart failure |
| Which conditions can increase afterload? | 1. hypertension 2. vasoconstriction |
| Normal SV is about ________. If it falls below ______, it is problematic. | Normal: 70 ml. If below 55ml, problematic. |
| Normal EF is about ___%. If it is below ____, it is problematic. | Normal: 65%. If below 55%, problematic. |
| Normal CO range: | 4.0 - 8.0 L/min |
| Normal HR: | 60 -100 bpm |
| Systolic heart failure refers to when the EF is below _______%. It is also called a _______. | EF <50%. HFrEF (heart failure with reduced EF). |
| A diastolic heart failure is one that has a EF of about ___% or more. It is also called a __________. It is problematic because the total amount of blood ejected each time is _________. | EF > 60%. HFpEF (heart failure with preserved EF) Blood ejected each time is less. |
| List some major problems that could lead to heart failure. | 1. High blood pressure 2. lung problems 3. infections 4. heart problems 5. lifestyle 6. other medical conditions |
| Outline the big picture of HTN leading to HF. | HTN -- increased peripheral pressure -- heart needs to work against increased resistance -- prolonged remodeling -- thickening of cardiac walls -- unable to stretch as much |
| In endurance-trained athletes, the overload is (pressure/volume). This results in (concentric/eccentric) hypertrophy, which makes the cardiac wall ____, chambers ____, and the sarcomeres are organized in _______. | In endurance-trained athletes, the overload is [volume]. This results in [eccentric] hypertrophy, which makes the cardiac wall [thinner], chambers [larger], and the sarcomeres are organized in [series]. |
| Causes of pathophysiological eccentric hypertrophy include _____ and ______. | Valve disease (regurgitation) Heart failure |
| In strength-trained athletes, the overload is (pressure/volume). This results in (concentric/eccentric) hypertrophy, which makes the cardiac wall ____, chambers ____, and the sarcomeres are organized in _______. | In strength-trained athletes, the overload is [pressure]. This results in [concentric] hypertrophy, which makes the cardiac wall [thicker], chambers [smaller], and the sarcomeres are organized in [parallel]. |
| Causes of pathophysiological concentric hypertrophy are | 1. diabetes mellitus 2. Hypertension 3. obesity 4. Ageing |
| Aside from concentric hypertrophy, there are many other potential causes for HFpEF. List 5 of them. | 1. Extracellular matrix remodeling 2. oxidative stress (higher demand) 3. increased cardiomyocyte stiffness 4. energetic abnormalities 5. inflammation and endothelial dysfunctions |
| Aside from eccentric hypertrophy, what other factors may cause HFrEF? | 1. extracellular matrix remodelling 2. Tissue necrosis 3. Apoptosis 4. Autopagy 5. oxidative stress 6. Energetic abnormalities |
| Which factors from above may cause either HFpEF or HFrEF? | 1. Extracellular matrix remodeling 2. oxidative stress 3. energetic abnormalities |
| What are the downstream effects of SNS in the long term? | 1. increased heart rate and inotropy 2. myocardial toxicity 3. negative remodeling of heart 4. worsened LV function 5. symptoms of HF |
| What happens downstream after RAAS activation? | 1. increased angiotensin II -- vasoconstriction -- increases afterload 2. Increased aldosterone -- altered hemodynamics -- increased preload 3. negative remodeling -- worsened LV function 4. symptoms of HF |
| The SNS can be inhibited by _________ while the RAAS pathway can be inhibited by ____________. | SNS: inhibited by beta-blockers RAAS: inhibited by ACE inhibitors/angiotensin receptor blockers/aldosterone antagonists / ADH antagonists |
| What are some biomarkers that are released in proportion to severity of HF? | BNP ANP (natriuretic peptides) |
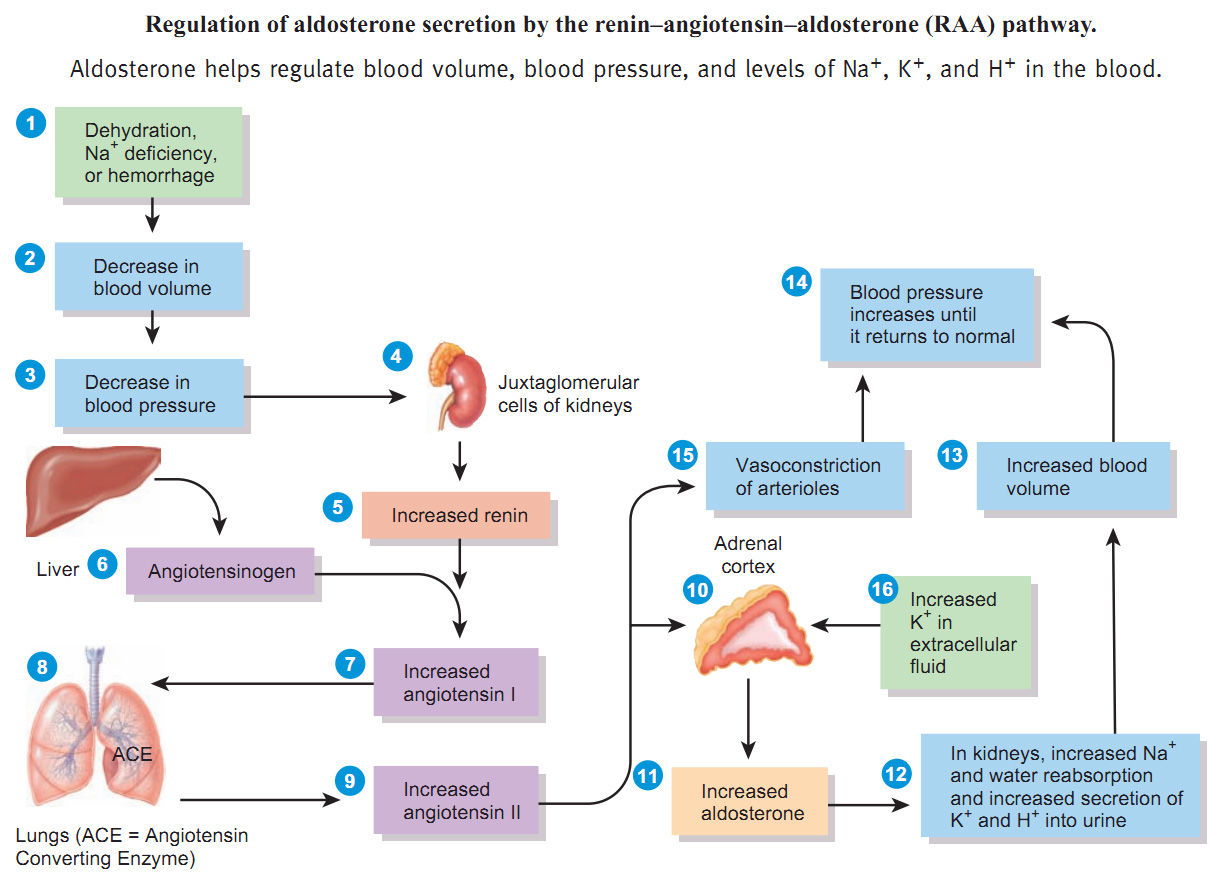
| Explain the RAAS pathway | |
| T/F: A patient without previous symptoms may experience a sudden, acute failure. | T. |
| T/F: The first episode is less likely to cause death as compared to additional episodes. | F. ANY episode may be the terminal event. |
| What is the most prominent manifestation of LV failure? | Dyspnea. (may escalate from DOE to resting dyspnea) |
| As HF advances, the patient may experience ______, and _______. | Orthopnea PND (paroxysmal nocturnal dyspnea) |
| Patient with LV failure may experience nocturnal cough and _________. | Hemoptysis |
| Why might the patient have dulled mental status and decreased urine output? | Poor CO and perfusion. |
| As compared to LV failure, RV failure is usually accompanied by _______ and _______. | Abdominal discomfort and peripheral edema |
| Why may a patient with RV failure have enorexia? | GI tract edema and liver enlargement |
| T/F: A patient with LV HF is more likely to have overnight weight gain. | F. (RV failure) |
| What are some other clinical findings that support heart failure? | 1. anxiety 2. falling O2 saturation 3. jugular vein distension (JVD) 4. tachycardia with weak pulse 5. hypotension 6. S3 or S4 |
| Match the symptoms with left-sided failure or right-sided failure. 1. Orthopnea 2. JVD 3. Fatigue 4. Restlessness 5. Tachycardia 6. Ascites 7. Paroxysmal nocturnal dyspnea 8. Elevated pulmonary capillary wedge pressure 9. Anorexia and GI distress 10. Weight gain 11. Cyanosis 12. Pulmonary congestion 13. increased peripheral venous pressure 14. dependent edema 15. exertional dyspnea | 1. Orthopnea (L) 2. JVD (R) 3. Fatigue (both) 4. Restlessness (L) 5. Tachycardia (L) 6. Ascites (R) 7. Paroxysmal nocturnal dyspnea (L) 8. Elevated pulmonary capillary wedge pressure (L) 9. Anorexia and GI distress (R) 10. Weight gain (R) 11. Cyanosis (L) 12. Pulmonary congestion (L) 13. increased peripheral venous pressure (R) 14. dependent edema (R) 15. exertional dyspnea (L) |
| What are some diagnostic tests for HF? | 1. Blood tests (pro-BNP, BNP, NT-proBNP) 2. Chest X-ray (cardiomegaly, pulmonary edema) 3. echocardiogram (look for hypo-, dys- or akinesis) |
| Treating congestive heart failure involves 'UNLOAD FAST', what are these treatments? | 1. Upright position 2. Nitrates 3. Lasix 4. Oxygen 5. ACE inhibitors 6. Digoxin 7. Fluids (Decrease) 8. Afterload (decrease) 9. Sodium restriction 10. Test |
| Outline the medical management for chronic heart failure. | 1. control risk factors (CAD, substance use, other conditions) 2. Treat symptoms (Medication and EXERCISE!) 3. Close follow-up (patient education, close monitoring, periodic check-ups) |
| The 5-year mortality rate following dx of HF is _______. | 45 - 60% |
| What are the patient presentations of Stage A HF? | 1. risk factors 2. no symptoms 'A for asymptomatic' |
| What are the patient presentations of Stage B HF? | 1. structural heart disease 2. still no symptom |
| What are the patient presentations of Stage C HF? | 1. structural disease 2. current/ prior symptoms C for '4 CLASS' |
| What are the patient presentations of Stage D HF? | 1. requires VAD (ventricular assistive device) 2. transfer to palliative care |
| Class I | Ordinary exercise OK |
| Class II | no resting symptom but reduced tolerance to exercise (5 - 10% annual mortality) |
| Class III | Mild activity cause symptoms |
| Class IV | Any physical activity is symptomatic. Resting symptoms. (30% - 70% annual mortality) |
| Make a table to differentiate CAD and HF. | see slide 25. |
| What is stenosis? | Hardening |
| What are some causes for aortic stenosis? | 1. calcification of previously normal valve 2. calcification of congenital bicuspid valve 3. rheumatic aortic valve disease (Strep infection) |
| Aortic stenosis causes ____ outflow obstruction, which increases ____ pressure, leading to ______ LV mass, and hence LV dysfunction. | Aortic stenosis causes [LV] outflow obstruction, which increases [LV systolic] pressure, leading to [increased] LV mass, and hence LV dysfunction. |
| LVET stands for ______. Increased LVET will increase the _______ of the heart, and reduce ___________. This together with increased LV mass result in ischemia of myocardial tissue, leading to heart failure. | LVET stands for [left ventricle ejection time]. Increased LVET will increase the [myocardial oxygen consumption] of the heart, and reduce [diastolic time]. This together with increased LV mass result in ischemia of myocardial tissue, leading to heart failure. |
| Why is decreased diastolic time result in decreased myocardial oxygen supply? | Because coronary arteries refill during cardiac diastole. |
| Which pressure is reduced by LV outflow obstruciton? | Aortic pressure (Ao pressure) |
| What type of hypertrophy in the LV is caused by aortic valve stenosis? | Concentric |
| ________ is the most common valvular defect. | Aortic stenosis |
| Mild, asymptomatic AS has (slow/fast) progression. About ____% of AS patients will end up having severe or symptomatic AS. | Slow progression, 20% |
| Clinical signs of AS. (SAD) | syncope angina dyspnea |
| Why might the patient experience exertional syncope when having AS? | Increased workload --> increased oxygen demand of body --> cardiac output restricted by stenosis of valve --> not enough CO to support body --> syncope |
| Why might the patient with AS have angina? | cardiac muscles increase in workload --> coronary artery unable to keep up with demand --> ischemia of cardiac muscles --> angina |
| T/F: Patient usually don't experience palpitations during AS. | F. Palpitation (especially a-fib) is a common symptom. |
| What might you here in heart sounds of a patient with AS? | 1. harsh, crescendo-decrescendo systolic murmur (heard best at aortic area) 2. a prominent S4 sound |
| S4 is associated with atrial contraction into a _______ left ventricle. | Stiffened |
| Upon palpation, an AS patient's carotid pulse may be ___________. | Parvus et tardus (low and slow) |
| What is the gold-standard of AS diagnosis? | 2-dimentional and doppler echocardiography. |
| What may happen to the patient's ECG if he/she has severe AS? | 1. enlarged R wave. 2. ST depression or inverted T wave |
| What are some possible treatments for AS? | 1. TAVR (thoracotomy and transcatheter aortic valve replacement) 2. Medication (diuretics, anti-arrhythmic, anti-hypertensives) |
| While tissue valve used for TAVR can last for ___ years, mechanical valves can last for _________. However, there is no medication required for _______ valve (other than ASA), but anticoagulation is always needed for _______ valve. | While tissue valve used for TAVR can last for [10 - 15] years, mechanical valves can last for [a lifetime]. However, there is no medication required for tissue valve (other than ASA), but anticoagulation is always needed for mechanical valve. |
| Aortic regurgitation usually happens in the ____ phase of cardiac cycle. | Diastolic |
| What effect does aortic regurgitation have on SV and LV volume? | 1. SV increases (due to increased afterload) 2. LV volume increases (due to increased work required) |
| Increased SV will also increase the _____ pressure, making the heart work harder and undergo _______. The cardiac oxygen consumption also ______, resulting in risk of __________. | Increased SV will also increase the [systolic] pressure, making the heart work harder and undergo [hypertrophic changes]. The cardiac oxygen consumption also [increases], resulting in risk of [myocardial ischemia]. |
| Increased SV also results in (increased/decreased) LVET, resulting in less time for _________ and hence _________. | Decrease LVET --> less time for coronary refill --> myocardial ischemia |
| The effective SV of patients with aortic regurgitation __________. | decreases |
| Other than age, radiation, and trauma, what are the possible etiologies of aortic regurgitation? (CREAM) | 1. Congenital heart defects (such as bicuspid aortic valve) - developed countries 2. Rheumatic fever - developing countries 3. Endocarditis 4. aortic dissection/ aortic root dilation 5. Marfan syndrome |
| List some symptoms of AR. | 1. dyspnea on exertion 2. Fatigue 3. decreased exercise tolerance 4. uncomfortable sensation of forceful heartbeat 5. chest pain or tightness that increases with exercise and subsides when at rest 6. orthopnea 7. weakness 8. syncope 9. swollen ankles and feet |
| What are some clinical signs of AR? | 1. collapsing pulse (Corrigan's pulse) 2. Hypertension with widened pulse pressure 3. Laterally displaced PMI (maximal impulse) 4. De Musset's sign (bobbing head) 5. Quincke's sign (capillary pulsation on light compression of nail beds) 6. early diastolic murmur |
| What are some medical tests that can be used to confirm AR? | 1. echocardiogram (look at competence of aortic valve and severity of regurgitant jet) 2. Cardiac x-ray (look for cardiomegaly and LV hypertrophy) |
| T/F: Aortic stenosis and aortic regurgitation have the same effective treatment. | T. (TAVR) |
| Which medications are useful in AR patients? | 1. beta agonists 2. nitrates 3. ACE inhibitors, ARBs, CCBs. |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.