
20000286
Description
Flashcards by Marissa Alvarez, updated more than 1 year ago

|
|
Created by Marissa Alvarez
over 5 years ago
|
|
| Question | Answer |
| The Endocrine Pancreas/Intermediary Metabolism Objectives | •Examine fuel metabolism, forms of stored fuels, and interconversion •Describe functional metabolic states •Define the role of the pancreas in glucose homeostasis •Examine the effects of pancreatic hormones on glucose, fatty acid, and amino acid levels •Examine glucose transport into cells •Describe the various types of diabetes and their impact on homeostasis and specific tissues •Examine the effects of hypo- and hyperglycemia •Examine the epidemiology of diabetes |
| Endocrine Control of Metabolism ____ = all chemical reactions that occur within the cells of the body the sum of the processes in the buildup and destruction of ____; specifically: the chemical changes in living cells by which energy is provided for vital processes and activities and new material is assimilated ___ (Fuel) Metabolism - reactions involving the degradation synthesis and transformation of proteins, carbohydrates, & fats. the intracellular process by which nutritive material is converted into ___ components | protoplasm Metabolism Intermediary cellular |
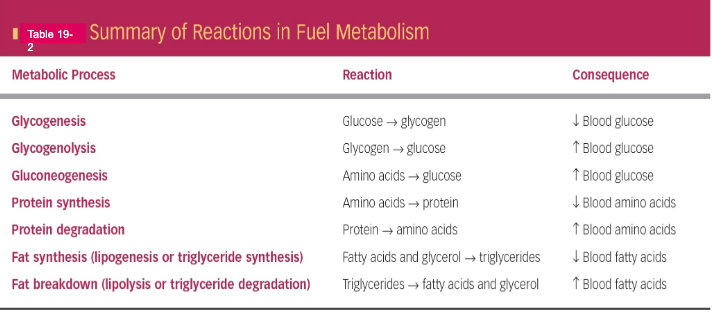
| Glycogenesis = glucose to ____ Glycogenolysis = glycogen to ___ Gluconeogenesis = Amino acids to ___ Protein synthesis = AA's to ____ Protein degradation = Protein to ___ Fat synthesis (lipogenesis/triglyceride synthesis) = Fatty acids & glycerol to ____ Fat breakdown (lipolysis/triglyceride degradation) = Triglycerides to ___ & ___ | |
| Anabolism: – Build-up of ___ organic molecules from smaller organic molecules | large |
| Catabolism - ___ of large, energy-rich organic molecules within cells | Breakdown |
| ->Excess glucose transformed to ___ and ___ to form triglycerides ->Excess a.a. transformed to glucose and fatty acids, eventually ending up as ____ | fatty acids & glycerol triglycerides |
| ADsorptive State (FED State) ->Carbs = ___ as major energy source (glycogen synthesis and storage) ->Excess converted and stored as ___ fat ->Fats = triglyceride ___ and storage ->Protein - protein synthesis ->Excess converted and stored as triglyceride ___ | glucose triglyceride synthesis fat |
| Postadsorptive State (FASTED State) ->Carbs = glycogen ___ & depletion glucose sparing for ___ use (New glucose through ____) ->Fats = triglyceride ___ energy for non-glucose using tissues ->Protein - protein catabolism (___ ___ for gluconeogenesis) | degradation brain gluconeogenesis catabolism amino acids |
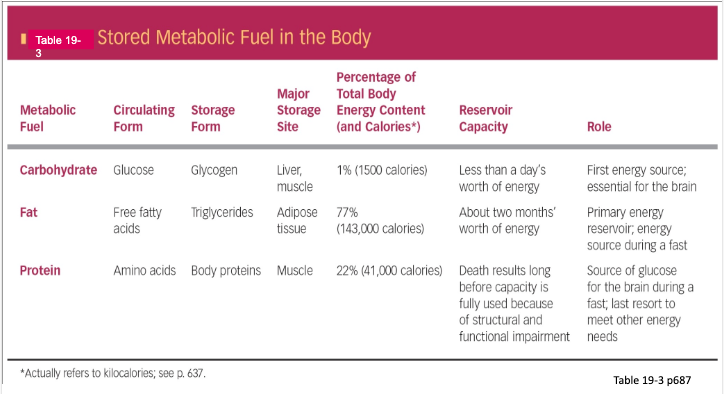
| Tissues involved in adsorptive and post-adsorptive metabolic states: –Liver •Primary role in [glucose]blood maintenance –Stores ___ –Site of _____ & other metabolic interconversions –Adipose tissue •Primary site of energy ___ •Regulates [fatty acid]blood –Muscle •Site of amino acid ___ •Major energy user –Brain •Can only use ___ •Cannot __ glucose (NEED for [glucose]blood maintenance) | glycogen gluconeogenesis storage storage glucose store |
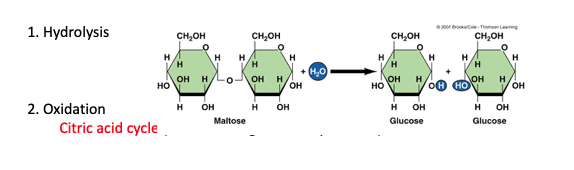
| Other Organic Intermediaries Are Energy Sources •Glycerol –Backbone of triglyceride (1 glyceride + 3 Fatty acids) –Converted to glucose by __ •Lactate –Result of ___ glucose metabolism in muscle –Converted to glucose by ___ •Ketone bodies (acetate acetoacidic acid β-hydroxybutyric acid) –Produced by liver during glucose ___ •Liver cannot completely catabolize fatty acids –Oxidation of fatty acids in liver yields ___ –Released to blood where other body cells use ketones for energy production via ___ ___ ___ •In long-term starvation: –Brain shifts fuel metabolism to use ___ »Prevents gluconeogenesis from depleting protein •Death due to starvation usually due to protein ___, not hypoglycemia •High levels of ketones lead to brain use and directly inhibit protein ____ | liver incomplete liver sparing ketones citric acid cycle ketones wasting degradation |
| Endocrine Pancreas (Insulin and Glucagon) | |
| ______ = Released in response to glucose and amino acids ___ digestion of nutrients, preventing excess in plasma ____ secretion of insulin, glucagon & SS itself (i.e. paracrine and autocrine actions) | Somatostatin Inhibits Decreases |
| INSULIN Insulin ___ blood glucose, amino acids, and fatty acids by –Altering transport of nutrients into cells –Altering activity of enzymes involved in specific pathways •Ex: ↑ glycogen synthase -> ↑ glucose to glycogen rate •Ex: ↓ hormone-sensitive lipase -> ↓ lipolysis (conversion of triglycerides to FFA+glycerol) Control of carbohydrates: •Circulating glucose concentration based on balance of: –Glucose absorption from GI tract –Glucose transport into cells (Only these two are subject to control) –___ glucose production (Only these two are subject to control) –Urinary excretion of glucose | lowers Hepatic |
| Glucose Transporters 1.) ___ facilitated diffusion into cell (through ___) 2.) Glucose -> glucose-6-phosphate –Phosphorylation »Traps glucose inside cell »Keeps intracellular glucose concentration __ | Passive GLUT low |
| Glucose transporters GLUT-1 Blood-brain barrier GLUT-2 ->Kidney and intestinal cells ->Na-glucose cotransporter GLUT-3 ____ GLUT-4 ->Most cells of body ->ONLY transporter that is sensitive to ___ ->Normally cells are relatively impermeable to glucose ->Abundant in resting ___ muscle & ___ ___ ->Recruitment triggered by insulin | Kidney Neurons insulin skeletal & adipose tissues |
| Insulin lowers blood glucose levels and promotes carbohydrate storage Insulin facilitates glucose transport into cells by insertion of __ at the cell membrane. ***Brain, exercising muscle, liver are NOT dependent on ___ for glucose uptake*** -Brain = GLUT 1 and GLUT3 -Exercising = contraction-induced glut-4 insertion -Liver = Not Glut4 dependent | glut4 insulin |
| Insulin actions on Fat 1. Insulin increases the transport of __ ___ and glucose (via GLUT4) into ___ cells 2. Insulin promotes reactions that use fatty acids and glucose for ___ synthesis 3. Insulin ___ lipolysis | fatty acids adipose triglyceride inhibits |
| Insulin actions on protein 1. Insulin promotes the active transport of ___ ___ from the blood into muscles and other tissues 2. Insulin increases the rate of amino acid incorporation into protein by stimulating the cell's protein-___ machinery 3. Insulin ___ protein degradation | amino acids synthesizing inhibits |
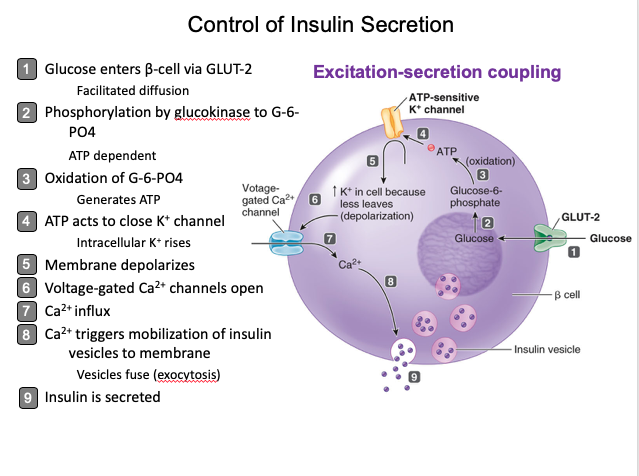
| CONTROL OF INSULIN SECRETION | |
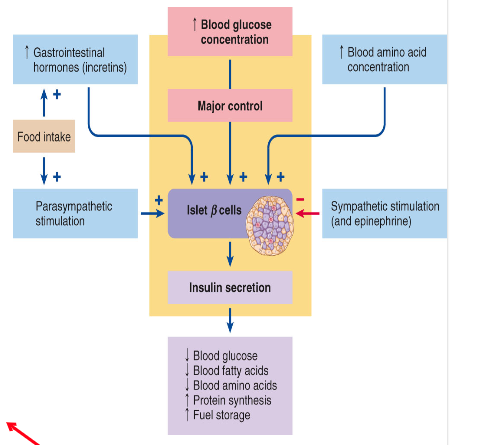
| Blood glucose is primary stimulus of insulin secretion, but also by: ↑ blood amino acids Amino acid uptake enhanced ↑ protein synthesis Stimulates insulin via excitation-secretion coupling Food intake: ____: glucose-dependent insulinotropic peptide (GIP), glucagon-like peptide (GLP) Feed-__ notification of impending rise in blood nutrients (Stimulates insulin via cAMP -> Ca2+) Nervous input to _-islets: ->Parasympathetic (vagal) stimulation (ACh stimulates via IP3/Ca2+) (Also feed-forward) ->Sympathetc inhibition & Epinephrine -> ↓cAMP | Incretins forward b |
| REVIEW | |
| Abnormalities in insulin secretion ->Diabetes - “siphon” or “running through” reference to the large volume of urine output characteristic of diabetes 1.) Diabetes Mellitus Mellitus = ____ ___glycemia - reduced cellular glucose uptake, liberation of glucose into the circulation from the liver 2. Diabetes insipidus Insipidus = ___ ->Due to lack of ___ | sweet Hyper tasteless vasopressin |
| 1. Diabetes mellitus - hyperglycemia A. Type 1 (insulin-___ or juvenile-onset) Lack of insulin ____ ~5% of all diabetes mellitus cases Autoimmune process involving the erroneous destruction of pancreatic -> cells by activated T lymphocytes Individuals require ___ insulin for survival | dependent secretion exogenous |
| 1. Diabetes mellitus - hyperglycemia B. Type 2 (non-insulin-dependent or ___ onset) Lack of ___ to insulin ~__ of all diabetes mellitus cases ____ is a major risk factor and can lead to inadequate insulin secretion & down-regulation of cellular insulin receptors. 90% of T2 Diabetics are overweight to obese | mature sensitivity 95% Obesity |
| Gestational Diabetes - abnormally elevated glucose levels during pregnancy as a result of decreased insulin ___ that occurs in approximately 4% of pregnancies similar to Type _ Cause unknown, but goes ___ following delivery. Associated with greater incidence of Type 2 diabetes ___ in life | sensitivity 2 away later |
| Obesity and Type 2 Diabetes Metabolic Syndrome (Syndrome X) – obesity, high triglycerides, low HDL, high blood glucose, high blood pressure Adipokines: ->___ – interferes with insulin actions, increased in obesity ->____ – enhances insulin sensitivity, decreased in obesity Inflammation – obesity is an “inflammatory state” and increases in things such as TNFα can decrease ___ to insulin ___ fatty acid levels - accumulation in muscle can interfere with actions of insulin - accumulation in liver can lead to increased hepatic glucose production - can trigger apoptosis of ___ cells | resistin adiponectin sensitivity High β cells |
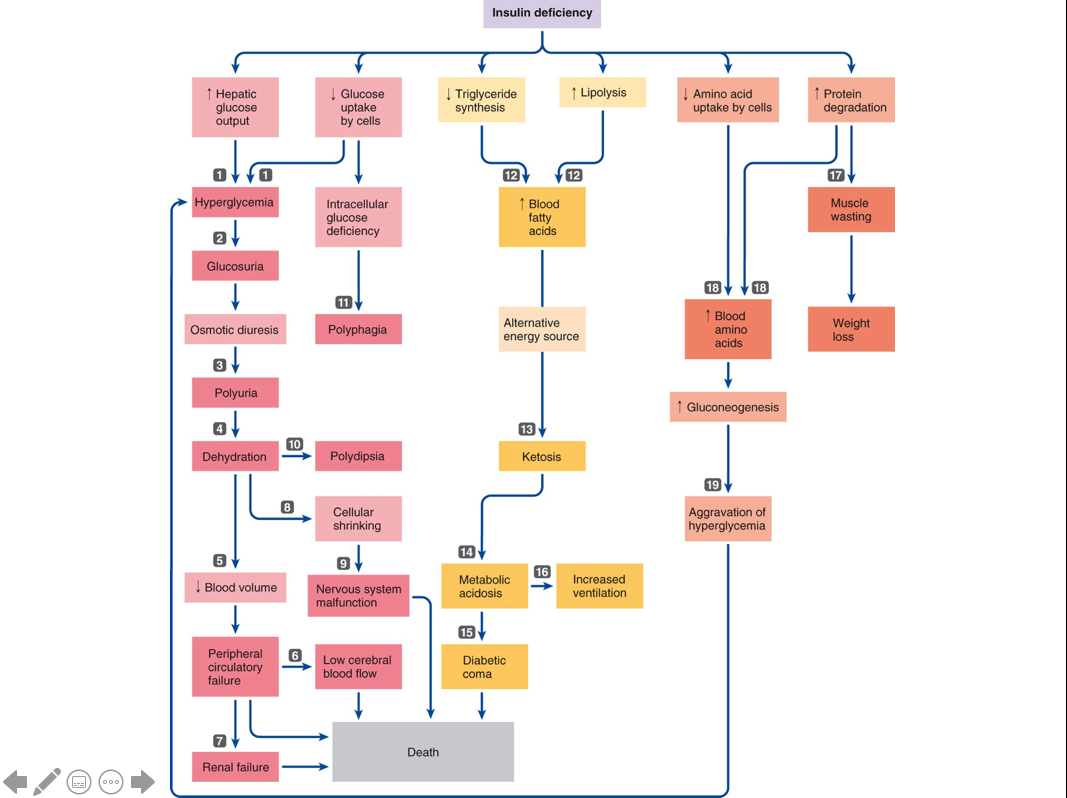
| Insulin Deficiency | |
| Long-term Consequences Diabetic Retinopathy: Vision ___ A.) Nonproliferative (most common) Pouch formation of capillaries in the back of the eye, leaking fluid and causing the eye to be unable to focus (__ __). B.) Proliferative (less common) Damaged vessels completely close off and new ones form, but are weak and leak blood (__ ___). ->Scar tissue can also form causing more damage to eyesight | Loss macula edema vitreous hemorrhage |
| Neuropathy: Sensorimotor and Autonomic Neuropathy Sensorimotor Neuropathy: Malfunction in nerves fibers that supply sensory input, leading to ___ and/or pain occurring typically at the extremities. Due to damage of blood supply to these nerves in a ___ environment. Autonomic Neuropathy: Malfunction in nerve fibers that control the heart, ___ tract, and urinary function. Common problem in diabetics is the inability to control ___ ___ and pressure to keep blood flowing normally to the brain when they stand up and as a result ___. Also due to damaged blood vessels around the nerves. | numbness hyperglycemic gastrointestinal heart rate faint |
| 3. Diabetic Nephropathy: Kidney Failure Destruction of the glomerular capillaries in the kidney which eventually leads to kidney failure and death; characterized by increased plasma ___ in the ___. | proteins urine |
| Treatment of Diabetes Type 1: Very controlled regimen of insulin ____ timed around meals Management of the types and amounts of foods consumed Exercise (remember that glucose uptake in exercising muscle is NOT insulin-____) | injections dependent |
| Treatment of Diabetes Type 2: Dietary control and exercise may be all that’s necessary ->10% weight __ can improve sensitivity to insulin significantly Pharmacological Intervention: Stimulation of insulin secretion by β cells (____) Suppressing liver output of glucose (__) Blocking enzymes that digest carbohydrates (α glycosidase inhibitors) Increasing sensitivity to insulin (thiazolidinediones) Mimicking the ____ (GIP, GLP) Increasing endogenous GLP-1 (Dipeptidyl peptidase or DPP-4 inhibitors) **If Type 2 persists, it can become __ _ due to depletion of β-cells | loss sulfonylureas metformin incretins Type 1 |
| Insulin Excess Consequences are primarily manifestations of the effects of ___ on the brain Insulin Shock: Can occur in a diabetic patient when too ___ insulin is injected Symptoms: largely due to effects at brain Treatment: ___ at first signs Reactive Hypoglycemia: beta-cell ___ or over-responsive beta-cells Insulin secretion ___ in response to elevated blood glucose and thus too much glucose is driven into cells Symptoms: tremor, sleepiness, inability to concentrate Treatment: limited ___ diet | hypoglycemia much sugar tumor overshoots carbohydrate |
| Glucose maintenance also involves α-cells of the islets Glucagon promotes ↑ blood glucose during ____ state | postabsorptive |
| Amino acid paradox (i.e. high protein meal) ↑ amino acids stimulate both α and β-cells If ONLY insulin is stimulated -> ___ Would promote further storage of already limited carbohydrate Parallel simulation of glucagon ensures glucose availability via hepatic glucose production Ultimately, glucose remains normal | hypoglycemia |
| Abnormalities of Glucagon Secretion There are __ __ clinical abnormalities associated with oversecretion or under secretion of glucagon Glucagon is usually elevated during diabetes and exaggerates the issue Insulin is necessary for glucose to enter ___ cells Thus, glucose ___ inhibit glucagon secretion For this reason, some Type 1 diabetics respond better to insulin in combination with ___, which inhibits ___ secretion | no known alpha cannot somatostatin glucagon |
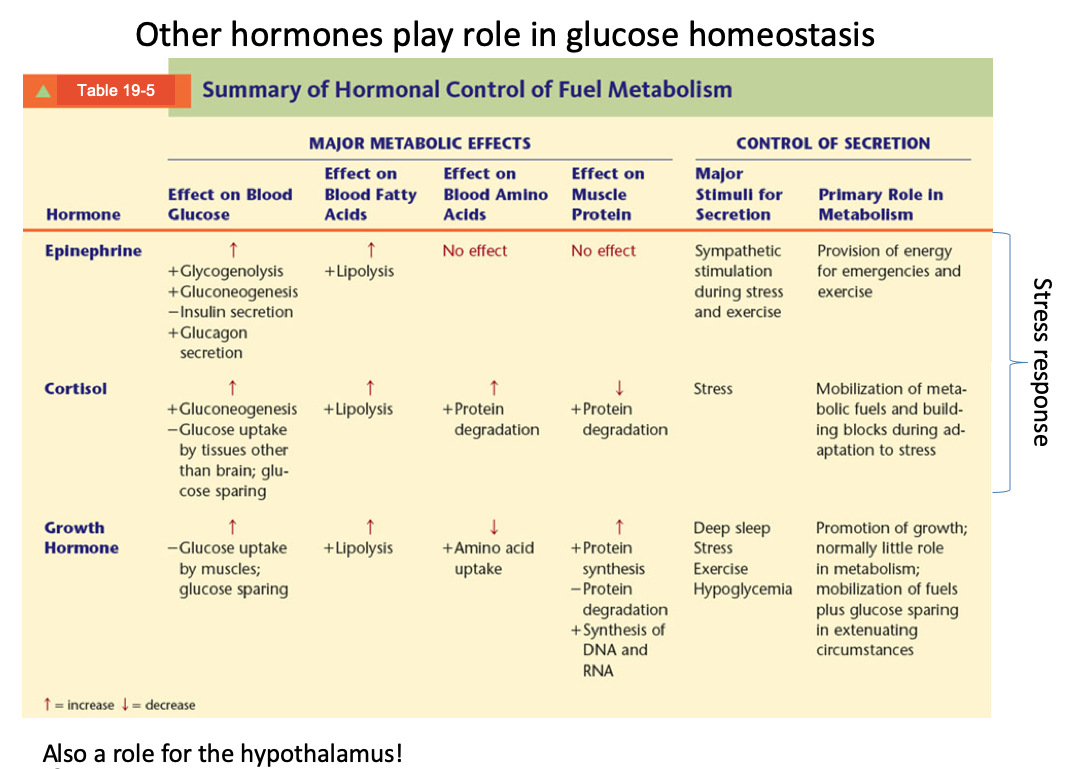
| Other Hormones play role in glucose homeostasis | |
| REVIEW |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
0 comments
Want to create your own Flashcards for free with GoConqr? Learn more.