21818181
| Question | Answer |
| Diuretics | - diuretics are drugs that increase the excretion of salt (mainly Nacl) and water by the kidneys. - they do this by reducing reabsorption of Na+ and Cl- back into the nephron - this has an osmotic effect, meaning they also decrease reabsorption of water - even a small decrease in the volume of water not being reabsorbed greatly increases urine volume. |
| Clinical use of diuretics | - Oedematous conditions such as renal failiure, renal disease and hepatic disease are treated with loop diuretics. - Hypertension is treated using thiazide-type diuretics, reducing blood volume and therefore cardiac output. May also dilate arteries. |
| Mechanisms of the clinical uses of diuretics | - Oedematous conditions: loop diuretics, K+ sparing diuretics. Jv= net flux of water across the vascular wall; increased flux causes oedema - Hypertension: thiazide diuretics; reduce blood volume and cardiac output. Many diuretics also dilate arteries. |
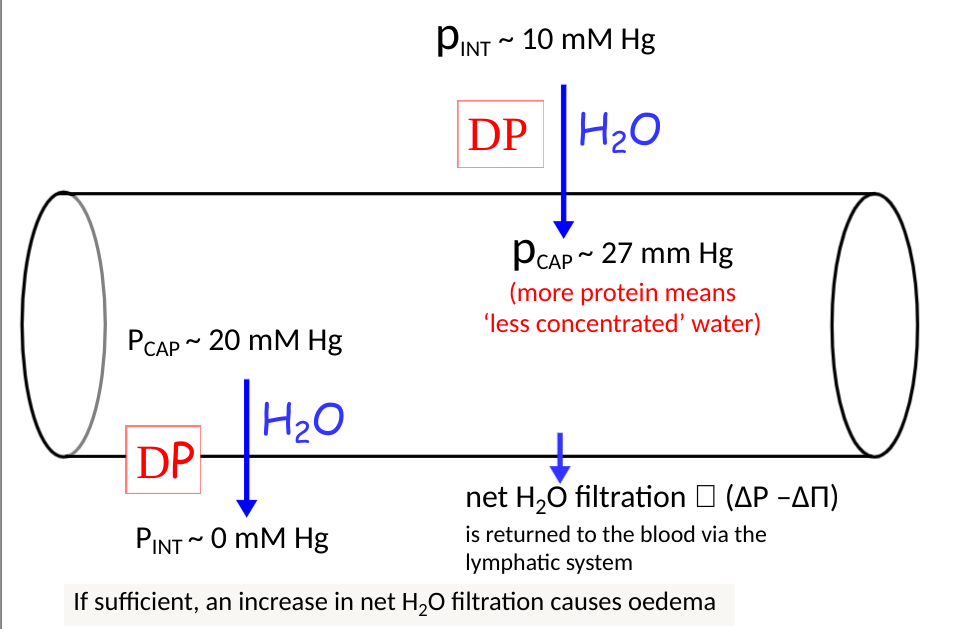
| Hydraulic and osmotic pressures in the microvasculature | |
| Normal mechanism in the kidney | - blood is filtered in the glomerulus, from the blood into the nephron - Na+ and H2O are reabsorbed back into the blood. Na+ reabsorption is regulated by aldosterone - that which isn't reabsorbed ends up in the urine, dragging water with it. This is regulated by ADH. |
| Effects of drugs on mechanisms in the kidney. | - Diuretics slightly inhibit the reabsorption of sodium, which can have a knock on effect to the amount of water reabsorbed into the blood, leading to a decrease in blood volume. |
| Sodium reabsorption and how diuretics effect it | - at the proximal tubule, 60-70% of Na+ is reabsorbed by H+ moving in - at he loop of Henle 20-30% of Na+ is reabsorbed by sodium-potassium pumps (this is inhibited by loop diuretics) - at the distal tubule, 5-7% of Na+ is reabsorbed via the sodium chloride cotransporter. - at the collecting tubule, ENAC channel, Na+ is reabsorbed (inhibited by K+ sparing diuretics) |
| 3 types of diuretics and their mechanisms: 1. Loop diuretics | Loop diuretics EG furosemide, torasemide, etacrynic acid Mechanism: - Block the Na+, K+ and 2Cl- co-transporters in the thick ascending loop of Henle. This causes a powerful diuresis because the kidneys lose their capacity to create a hypertonic medullary interstitium needed to drive ADH induced water reabsorption Main use: oedematous condition Adverse effects: Hypokalemia, metabolic alkalosis, depletion of plasma Ca2+ and Mg2+, hypovolaemia, ototoxicity (deafness,tinnatius dizzines); occurs if concurrent use w/ antibiotic aminoglycoside |
| 3 types of diuretics and their mechanism: 2. Thiazide-type diuretics | Thiazide-type diuretics eg Indapamine, bendroflumethazine, metolazone. Mechanism: Thiazide-type diuretics block Na+, Cl- co-transport in the distal convoluted tubule, reducing plasma volume, venous return and cardiac output. They also reduce total peripheral resistance (mechanism unknown). Adverse effects: Hypokalemia, hyperglycemia, hyperuricaemia |
| 3 types of diuretics and their mechanisms: 3. Potassium sparing diuretics | - inhibit Na+ uptake and K+ secretion in the collecting tubule, reducing the loss of K+ from the body. - can cause hyperkalemia if used alone, but using them in conjuction with other diuretics can help prevent this. - 2 types of K+ sparing diuretics: Aldosterone receptor antagonists and Blockers of the epithelial Na+ channel (ENaC) - main effect is via an active metabolite; 17a-thiomethyl-spironolactone |
| Why do loop diuretics and thiazide diuretics cause hypokalemia? | - they inhibit Na+ absorption and K+ secretion at the collecting tubule: ^sodium moving into the cell causes it to become negatively charged, causing K+ to move into the cell, pushing others out via the ROMK channel |
| Effects of aldosterone | - aldosterone is a 'mineralcorticoid' steroid hormone that increases Na+ reabsorption and K+ secretion in the collecting tubules. - It is released from the adrenal cortex by angiotensin II. - It acts on the cytoplasmic receptors in principle cells of the late distal tubule and collecting duct. - increases production of aldosterone-induced proteins which act to increase the expression and effect of the Na+ pump and Na+ and K+ channels |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.