2434450
Description
Flashcards by Annie Nguyen, updated more than 1 year ago
|
|
Created by Annie Nguyen
about 9 years ago
|
|
| Question | Answer |
| GI symptoms: Abdominal pain, bloating, steatorrhea, abdominal distention and diarrhea Systemic symptoms: fatigue, weight loss, stunted growth, and muscle pain | Celiac DX |
| Definitive diagnosis is made with IgA transglutaminase antibody test Biospy performed by endoscopy or colonoscopy | Celiac Sprue |
| DDX: irritable bowel disease diverticulitis gastroenteritis, appendicitis infection food poisoning medications side effect metabolic disorders gastrointestinal obstruction | Celia Sprue |
| Iron deficiency anemia Early onset osteoporosis or osteopenia Lactose intolerance Vitamin and mineral deficiencies Central and peripheral nervous system disorders Pancreatic insufficiency GI cancers Gall bladder complications Neurological manifestations, including ataxia, epileptic seizures, dementia, migraine, neuropathy, myopathy | Non-Compliance to Strict Gluten-Free Diet |
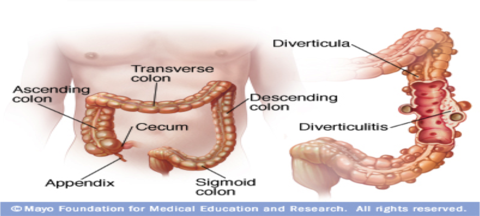
| A condition when undigested food causes pressure on the colon and forms a bulging pouch that pushes weak portion of colonic wall. Increased incidence with age. This condition occurs near the distal portion of left colon, which is referred as sigmoid colon | Diverticulosis |
| Sign and Symptoms Patient have localized mild to moderate pain in Left lower quadrant. Frequent nausea and vomiting Fever Abdominal tenderness Loose bowel movement or constipation | Diverticulitis |
| Complicated Diverticulitis Occurs when colonic obstruction, frank perforation, intestinal rupture, abscess, fistula, or peritonitis developed | Type of Diverticulitis |
| Uncomplicated Diverticulitis Occurs when microperforation is limited to mesentery wall and pericolic fat and usually developed in sigmoid colon | Type of Diverticulitis |
| Diagnosis is based upon the patient history and physical examination. Blood test and blood culture reveals leukocytosis. CT scan of abdomen is considered as best diagnostic test to confirm the diagnosis. Endoscopy and colonography is avoided to prevent risk of perforation. | Diagnosis of Diverticulitis |
| Conservative Therapy Patient are admitted to the hospital for about a week to receive treatment for uncomplicated diverticulitis Initial treatment includes bowel rest and maintain NPO status (nothing to eat or drink by mouth) once patient started feeling better and have no abdominal pain NPO change to clear liquid diet Advance to low fat and high fiber for 2 to 4 weeks | Treatment Plan For Diverticulitis |
| High fiber diet helps to firm the stool, regular bowel movement, resolve diarrhea and abdominal discomfort Intravenous nutrition and fluids are administered to maintain nutrition, hydration and electrolyte balance until patient is able to tolerate per oral Anticholinergic and antispasmodic agents are used during the course of treatment to relieve colon spasm | TX Plan for Diverticulitis |
| Demerol is used commonly for pain Morphine is avoided due to the side effect of increasing colonic pressure antibiotic therapy is very effective for outpatient treatment ciprofloxacin and metronidazole 500mg BID X 7-10 days, Bactrim DS 160/800mg BID X7-10 days are commonly used or until the patient is afebrile for 3-4 days. | Pharmacology for Diverticulitis |
| Surgical Intervention patient with bowel obstruction or perforation need temporary colostomy Typically laparoscopic surgery is done for colon resection, drainage of abscess, fistula repair or reversal of temporary colostomy Immune-compromised patient are more prone for postoperative complications like slow wound healing | Surgical option for DIverticulitis |
| Patient with diverticulitis are encouraged to make numerous lifestyle changes to avoid flare-ups symptoms Life style changes includes, avoid smoking, increase diet which are high fiber source, drink at least six to eight glasses of water, participate in regular exercise, avoid foods or medications that may causes constipation | Patient education for diveticulitis |
| Encourage patient to minimize fat in their diet and increase fiber rich diet like whole grains, legumes, high-fiber cereals, fruits, and green vegetables High fiber diet helps to bulk stool, which reduce the incidence of constipation and prevent the formation of further diverticula, reduce abdominal discomfort, bloating, and flatulence. Encourage patient to discuss their diet with their primary care provider so that provider can guide them correctly | Patient Education for Diverticulitis |
| Abdominal pain migrates to right lower quadrant and become more intense and localized. Appendicitis is the differential diagnosis of diverticulitis because in diverticulitis pain is in the lower abdomen but more intense and localized in the left lower quadrant, where sigmoid colon is located | Acute Appendicitis |
| Colorectal cancer also resembles the symptoms of the generalized lower abdominal pain, fatigue, weakness, weight loss, alternating diarrhea and constipation. Colorectal cancer is differential diagnosis of diverticulitis because colonoscopy will be positive, colonoscopy is necessary for biopsies, positron emission tomography (PET) scan is additional diagnostic test detect tumor origin and metastasis | Colorectal Cancer: |
| common disorder that affects the large intestine (colon). IBS commonly causes cramping, abdominal pain, bloating, gas, diarrhea and constipation. IBS is differential diagnosis of diverticulitis because IBS improved with defecation, onset change in stool frequency, form and appearance. | Irritable Bowel Syndrome |
| 1) Diverticulitis is an inflammatory response of obstructed diverticulum and increased pressure on diverticulum due to obstruction leads to perforation of diverticulum A) True B) False 2) Complicated diverticulitis is when micro perforation is limited to mesentery wall and peri colic fat. A) True B) False | TRUE and False |
| What is the recommendation for patient with diverticulitis to prevent flare-ups symptoms? A) Drink plenty of water B) Eat high fiber diet C) Quit smoking D) Only A & B D) All of the above | E. All of the above |
| Diverticulitis commonly occurs at long intestine in A) Ascending colon B) Descending colon c) Sigmoid Colon D) Transverse Colon | C. Sigmoid Colon |
| 5) Which pain medication is avoided due the side effect of increasing colonic pressure in diverticulitis? A) Morphine B) Demerol C) Dilaudid D) Tylenol | A. Morphine |
| the chronic GI functional disorder characterized by abdominal discomfort or pain with altered bowel habits in the absence of a specific and unique organic pathology Affects the large intestine (COLON). | IBS |
| abdominal pain or cramping, having a bloated feeling, gas, diarrhea/ constipation mucus in the stool visible distention and bloating in some cases | IBS |
| Abnormal Motility, Constipation-predominant irritable bowel syndrome (IBS-C) Diarrhea-predominant irritable bowel syndrome (IBS-D) Visceral Hypersensitivity, Enteric infection Psychosocial Abnormalities depression, anxiety, panic attacks and hypochondriasis | IBS |
| made by the physical examination and the presenting clinical signs and symptoms The Rome III diagnostic criteria recurrent abdominal pain or discomfort for at least 3 days/month in the last 3 months associated with at least one or more of the following symptoms improvement with defecation, onset associated with a change in frequency of stool, onset associated with a change in form or appearance of stool If the patient presenting with the signs and symptoms of IBS but has a positive family history intestinal cancer, inflammatory bowel disease, or celiac disease then he or she has to undergo further evaluation | DX of IBS |
| Adolescence : Incidence Increases Third and fourth decades it peaks Affects women more than men Symptoms after age 50 is unusual, and should consider obtaining a colonoscopy, if not already performed | IBS |
| rritable bowel syndrome is a chronic condition Managing the symptoms with pharmacologic treatment should be viewed as being adjunctive rather than curative making the symptoms diary, and knowing the stressors either medication, dietary or psychosocial as it helps manage the symptoms and increase adherence to treatment plan Stress may trigger Irritable Bowel Syndrome. | IBS |
| Causes : Irregular bowel habit from repeated inhibition of normal defecation reflexes. Overuse of laxatives for prolonged periods. Due to slow colonic transit (more in women) Defecatory disorders (more in women) | Constipation |
| Endocrine disorders Hypothyroidism Hyperparathyroidism Diabetes mellitus. Metabolic disorders Hypokalemia Hypercalcemia Neurologic conditions (causing gut dysfunction & myopathies) Parkinsons Multiple Sclerosis Sacral nerve damage (prior pelvic Sx, tumor) Paraplegia Autonomic neuropathy | Secondary Constipation |
| Structural abnormalities that can cause constipation Anorectal abnormalities-prolapse, stricture, fissure, ulcer Perineal descent Colonic mass with obstruction- adenocarcinoma Colonic stricture- radiation, ischemia, diverticulosis Hirschsprung disease Idiopathic megarectum | Secondary Constipation |
| Most commonly reported symptoms: Hard stools Excessive straining Fewer than 3 stools/week Feeling of not having a complete evacuation Associated symptoms include- bloating fullness, abdominal pain | Constipation |
| Symptoms r/t specific causes Rectal pain or bleeding- with hemorrhoids, fissures Decrease in diameter of stool- in intestinal obstruction Nausea, polyuria, fatigue- in hypercalcemia DRE- may identify stricture of anus, rectocele, rectal prolapse, perineal descent, abnormal pelvic floor motion Presence of Rome III criteria symptoms confirms constipation. | Constipation |
| Physical Examination Auscultate bowel sounds Assess tympani to evaluate stool in the colon Palpate abdomen for tenderness & masses Digital Rectal Exam (DRE ) to palpate hard stool, assess masses, hemorrhoids, anal fissures,sphincter tone, prostatic hypertrophy in men, push effort, posterior vaginal masses in women | DX for constipation |
| Common Radiologic Exam / Imaging Abdominal plain X-Ray (KUB) Helpful in detecting significant stool retention May suggest diagnosis of megacolon Barium enema To identify areas of colon dilatation & obstruction Endoscopic Examination - to r/o malignancy Colonoscopy / Flexible sigmoidoscopy Indicated in pts with alarm symptoms | DX constipation |
| Special Procedures Radiopaque marker methods Most commonly used – to measure colonic transit time Abdominal radiograph is performed 120 hrs after ingestion of 24 radiopaque markers If it shows retention of >20 %, prolonged colonic transit is indicated. | DX for constipation |
| Inadequate fluid intake & medications are the main causes for constipation Thorough H&PE–initial step in elderly assessment Digital rectal exam (DRE) – very significant in elderly presenting with loose stools Fecal impaction may result in overflow incontinence causing loose stool | Geriatrics constipation |
| Bulking agents can worsen constipation in elderly who do not consume adequate fluids Mineral oil can cause aspiration pneumonia Prophylactic treatment is beneficial for elderly at high risk for fecal impaction | Geriatric constipation |
| Dietary modification Increase dietary fiber in normal transit constipation Fiber rich foods and fiber supplements Decreases colonic transit time Increases stool bulk Sufficient fluid intake -daily 3L(thirteen 8oz )for men, 2.2L (nine 8oz)for women 30ml/kg bodywt daily for pts taking Bulking agentsDietary modification Low residue diet is recommended for patients with refractory slow transit constipation and with pelvic floor dyssynergy Fiber can worsen symptoms in pts with defecatory disorders, colonic inertia, opioid induced constipation , and Lifestyle modification Increasing physical activity and exercise Attempting defecation at particular times Colonic activity is stimulated during waking up in the mornings/meals Probiotics Promotes colonic mucosal health Lactobacillus may improve constipation | Non-pharmacologic Therapy for constipation |
| Bulking agents Stool softeners and emollients Osmotic laxatives Stimulants Chloride secretory agents Opioid-receptor antagonists | Pharmacologic therapy |
| First line agents for constipation Help to produce softer stool They expand with water->Increases bulk of stool ->Softens stool Ex- psyllium, calcium polycarbophil, methylcellulose C/I- patients with swallowing difficulty, possible rectal mass/bowel obstruction, those who do not consume adequate fluid. | Bulking agents |
| Have a detergent effect on the stool consistency Ex- docusate, mineral oil Use mineral oil with caution in elderly- can cause aspiration & lipoid pneumonia | Stool softeners & emollients |
| Used when bulking agents or stool softeners are not effective Increases secretion of water into the intestinal lumen--> softening of stools and stimulation of defecation Ex- polyethylene glycol(PEG)—>considered best. Lactulose, sorbitol, magnesium hydroxide | Osmotic laxatives |
| Increases peristaltic contraction, increases intestinal motility, Results in a BM 6-12 hrs after ingestion. Melanosis Coli-marker for chronic laxatie use seen on colonoscopy assoc. with stimulant laxatives. | Stimulant medications: Constipation |
| Chloride secretory agent. stimulates intestinal chloride secretion, increase intestinal fluid, and accelerates colonic transit. last line. ex. lubiprostone and linaclotide | Chloride secretory agent: constipation |
| Blocks peripheral opioid receptors of the GI tract, reverses opiod induced peristalsis inhibition, mostly used in pallative care. ex. methylnaltrexone, mu-opiod receptor antagonist. | Opioid- receptor antagonist |
| Teaching r/t drug therapies (contd) Fiber should be taken 1 hr before or 2 hr after other medication since fiber may inhibit drug absorption Onset of action varies with laxative types PEG (Miralax) and Magnesium hydroxide preparations are not recommended for those with CHF and Chronic renal disease – may cause electrolyte imbalance | Patient Education: constipation |
| Irritable Bowel Syndrome- less seen in >=50 yrs Recurrent abdominal pain / discomfort- improved upon defecation Intestinal Obstruction Progressive constipation associated with pain and nausea, marked abdominal distention, reduction in BM frequency, thin “pencil” stool, palpable mass, pain/tenderness Colon Cancer- more in > 40 yrs Unexplained constipation associated with abdominal distention, colicky pain, weight loss, anorexia, decrease in laxative effect, blood/pus/mucus in stool. | DDX for constipation |
| Which one of the following is included in Rome III criteria used by clinicians to define constipation? Straining during all defecations. Loose stools are rarely present without use of laxatives. Hard or lumpy stool in more than 20% of all defecations. Fewer than 4 defecations per week. | Loose stools are rarely present without use of laxative. |
| The estimated prevalence rate of constipation in individuals older than 65 years is: 25% 30% 40% 45% | 40% |
| Melanosis coli is associated with the use of: Stimulant laxatives Osmotic laxatives Bulking agents Stool softeners None of the above | stimulant laxatives |
| Which one of the following is linked with aspiration and lipoid pneumonia in older adults? Magnesium citrate Lactulose Sorbitol Mineral oil | mineral oil |
| A chronic inflammatory condition of the bowel One of the inflammatory bowel diseases (IBD) Affects the mucosal inner lining of the colon and rectum, resulting in inflammation and ulceration | Ulcerative Colitis |
| The appearance of inflamed colon is characterized by Edema Hyperemic Granular Mucopus Friability Erosion Wide range of ulcerations tend to Cause normal mucosal areas to look like polypoid, called psuedopolyp | Ulcerative Colitis |
| The disease can be Limited only to recto-sigmoid area, called proctosigmoiditis Expanded to the splenic flexure, called left sided colitis Expanded proximally, called extensive colitis | Ulcerative Colitis |
| The signs and symptoms of UC Diarrhea with blood or pus Abdominal pain and cramps Rectal pain and bleeding Urgency to defecate Loss of weight Severe tiredness Anemia Fever | SXS of UC |
| Most of the population experience sudden onset of symptoms and a period of remission (McPhee & Papadakis, 2014) In the United States About 2 million people are affected Ages 15 – 30 are more frequently affected Men and Women are equally affected UC is exacerbated by Use of NSAIDs Intake of less antioxidants (Vitamin A & E) Psychological stress Alcohol Smoking Intake of milk products | Risk Factors of UC |
| Proper and accurate history collection Physical Examination Abdominal and rectal examination Labs Stool tests Complete blood count (CBC) Erythrocyte sedimentation rate (ESR) C-reactive protein (CRP) Electrolytes Albumin and Liver function test (LFT) | DX of UC |
| Imaging- in severe colitis Abdominal plain X-rays - to look for colonic dilatation Barium enema studies are in limited use, induce toxic megacolon Endoscopy Sigmoidoscopy can be done in acute colitis – to look for abnormal changes in mucosal lining Colonoscopy should be avoided in severe colitis – risk of bowel perforation | DX of UC |
| Main Objectives - to decrease symptoms and to continue remission. Anti-inflammatory drugs- first line of treatment: Aminosalicylates (Sulfasalazine, Mesalamine, Balsalazide, Olsalazine) Help to decrease symptoms of UC Available in the form of suppository, enema, and oral Corticosteroids (Prednisone, Hydrocortisone) Used to treat moderate to severe UC, if other treatment is failed Available in the form of oral, intravenous, enema, and suppository Not advised for long term use- increased and dangerous side effectsImmune system suppressors To control immune system response, thereby reducing the inflammation Azathioprine (Azasan, Imuran) and Mercaptopurine (purinethol, Purixam) Broadly used by providers to treat IBD Regular follow-up and blood works are necessary to look for side effects Cyclosporine (Gengraf, Neoral, Sandimmune) Used if other treatments are failed Not for long term use due to serious side effectsInfliximab (Remicade), Adalimumab (Humira), and Golimumab (Simponi) Used for moderate to severe UC if other treatments are failed or not tolera | TX of UC |
| Antibiotics To prevent or control infection if fever presents Anti-diarrheal Used with caution due to risk for developing toxic megacolon Lopramide can be used for severe diarrhea Pain relievers Tylenol can be used for mild pain Avoid NSAIDS- exacerbate the disease Iron Supplements To prevent iron deficiency anemia due to chronic ble | Tx of UC |
| Maintenance therapy UC patients who are on remission period to prevent reoccurrence Oral aminosalicylates are commonly prescribed If patient treated with infliximab, need to be continued with infliximab or azathioprine. Indicated for patients who are unresponsive to medication therapy Unmanageable toxic megacolon Unmanageable intestinal bleeding Prolonged use of steroids Dysplasia or adenocarcinoma | Therapy of UC |
| Avoid alcohol and smoking - to prevent worsening of symptoms Take medications regularly as prescribed (CCFA, 2015) In active diarrhea, avoid dairy products, spicy and fatty foods, and high fiber foods – aggravate the symptom (Wedro, 2015c) Eat well balanced and nutritious diet - to prevent weight loss Frequent Colonoscopy studies - to detect signs of cancer Adequate exercise, calcium and vitamin D supplements To prevent osteoporosis due to prolonged corticosteroid therapy | Patient Education for UC |
| Which of the following is considered as an inflammatory bowel disease (IBD)? a. Celiac disease b. Diverticulitis c. Infectious colitis d. Ulcerative colitis 2. Which symptom is the hallmark in ulcerative colitis (UC)? a. Bloody diarrhea b. Constipation c. Dysuria d. Vomiting | 1. ulcerative colitis 2. bloody diarrhea |
| Which age group of people are more commonly affected by UC? a. 15 - 30 years b. 35 - 45 years c. 40 - 60 years d. 50 - 75 years 4. Which of the following drug class is the first line of treatment in UC? a. Analgesics b. Antibiotics c. Anti-inflammatory d. Immunosuppressant | 1. A 2. c |
| In severe UC, the following diagnostic tests are performed except a. Abdominal X-ray b. Colonoscopy c. Labs d. Physical examination | A. abdominal x-ray |
| Originates from a growth of non-cancerous tissue or tumor, usually a polyp on the inner lining . Adenomatous polyps are pre-cancerous cells. 85% of adenomas turns into cancer. Hyperplastic and inflammatory polyps are not pre-cancerous, but may increase the risk of adenomas. A family history in 20% of patients | Patho of Colon Cancer |
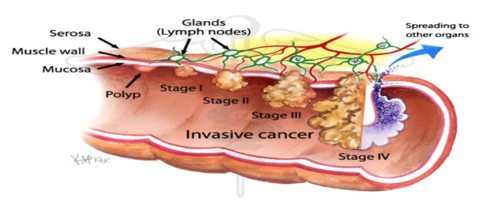
| When cancer cells are detached from their primary source, they invade into nearby blood or lymph vessels and can travel to distant parts of the body, a process called metastasis | |
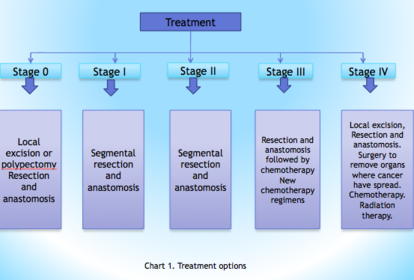
| Stage 0 (Carcinoma in situ) – Cancer has not grown beyond the inner layer (mucosa) of the colon. Stage I - Cancer has grown through the muscularis mucosa. Stage II - Cancer has grown into the outermost layers of the colon or rectum. Stage III – Cancer has outgrown the wall of the colon. Invasion into lymph vessels. Beginning of metastasis. Stage IV – Cancer has spread to peritoneum and distant parts of body. | Stage of Colon Cancer |
| Change in bowel habit Diarrhea or constipation Blood in stool Feeling of fullness in the rectum Unusual narrowing of stool Bloating, cramps or gas pain Unintentional weight loss Fatigue Anemia | SXS of Colon Cancer |
| LABS A complete blood count (CBC) may detect anemia. Liver function tests to rule out liver metastasis. Carcinoembyronic antigen (CEA) levels can detect prognosis and extent of the cancer.Fecal Occult Blood Testing (FOBT) examines the stool for hidden blood that occasionally sheds from adenomatous polyp sand cancer. Fecal Immunochemical test (FIT) detects antibodies specific to human globin in the stool. Colonoscopy- Gold standard, cost effective, reliable. Permits biopsy for pathologic Confirmation of malignancy. CT colonography- Two and three Dimensional views are taken Through colonoscopy. | DX of Colon Cancer |
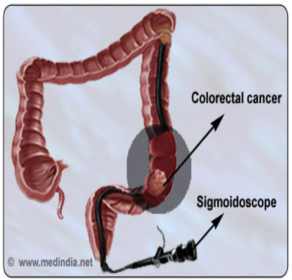
| Flexible sigmoidoscopy Looks inside the rectum and sigmoid colon. Only a portion of distal colon is examined. Computed Tomography Looks beyond the intestinal layers. Most useful in detecting metastasis | |
| Barium enema – Liquid barium sulfate and air is inflated into the inner part of the colon and rectum followed by x-rays to look for obstruction | DX of Colon Cancer: Imaging for obstruction |
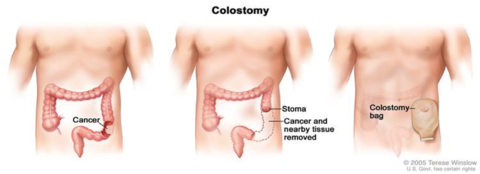
| Local excision and polypectomy are done at stage 0 and early stage I, can be done through colonoscope. In Colectomy, the cancerous segment of the colon as well as immediate lymph nodes is removed through an abdominal incision also termed as resection and anastomosis. A temporary or permanent colostomy is made for fecal diversion . | |
| Works well and safe Shrink or slow the growth of tumors and reduce pain. Adjuvant chemo is given after the surgery to shrivel the remaining cancer cells. Neo adjuvant chemo is done before surgery to shrink the cancer and make surgery easy to manage. In target therapy, drug stops the action of molecules that aid the growth of cancer. Works differently from chemotherapy and less side effects. | TX for colon cancer |
| Aimed when the cancer has adhered to an adjacent internal organ or the inner layer of the abdomen. May be used before, during and after surgery to shrink the tumor and reduce the risk of recurrence. Most often, it is used in stage IV to alleviate symptoms in people with progressive cancer causing intestinal blockage, bleeding, or pain. | TX for colon cancer |
| Stages for Colon Cancer | |
| Tests that detect adenomatous polyps and cancer Colonoscopy every 10 years Flexible sigmoidoscopy every 5 years Double contrast barium enema every 5 years CT colonography every 5 years | Years for colonoscopy, sigmoidoscopy, barium enema, and CT colonography ? |
| Tests that primarily detect cancer FOBT every year FIT every year Stool DNA test every 3 years | Screening in years for FOBT, FIT, Stool DNA. |
| A well-balanced diet. Increase fruits and vegetables, and reduce the fat, particularly animal fat. Maintaining body weight, exercise and physically active lifestyle. Quit smoking. A low dose aspirin a day can lower the chances of developing polyps, especially in patients with previous history of polyps or colorectal cancer | Patient Education of Colon Cancer |
| 1. Most reliable, preferred and cost effective diagnostic test to detect colon cancer is Sigmoidoscopy Barium enema Colonoscopy Labs and Fecal Occult Blood Test | Colonoscopy |
| 2. One of the recommendations from the Society of Geriatric Oncology (SIOG) in regards to the treatment goal for elderly is To provide the most intensive and applicable treatment thought to be safe and potent to their biological age and comorbidities. Treat them like young patients. Treatment is very limited as there is usually risk for complications in elderly. Maximize the survival rate even though complication arises | To provide the most intensive and applicable treatment thought to be safe and potent to their biological age and comorbidities. |
| 3. What is metastasis? Cancer cells detached from primary source and attaches within five inch of primary source. Cancer cells detached from primary source and travels to distant parts of the body. Cancer cells detached from primary source and infiltrates in the liver. Cancer cells detached from primary source and forms of an obstructive mass. | B. Cancer cells detached from primary source and travels to distant parts of the body. |
| . According to the American Cancer Society, colonoscopy should be done Beginning at age 50, every ten years. Beginning at age 45, every ten years. Beginning at age 50, every year. Beginning at age 60, every ten years. | A. Beginning at age 50, every ten years |
| hile educating your patients on colon cancer, you will explain them to watch for which of the pertinent colon cancer symptoms? Change in bowel habit, weight gain and headache. Diarrhea with abdominal pain for two – three days. Belching and heartburn. Change in bowel habit, dark and narrow stool, fatigue and unusual weight loss. | D. Change in bowel habit, dark and narrow stool, fatigue and unusual weight loss. |
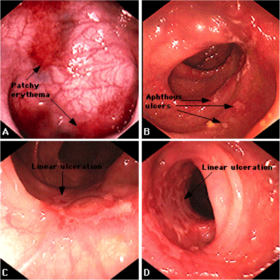
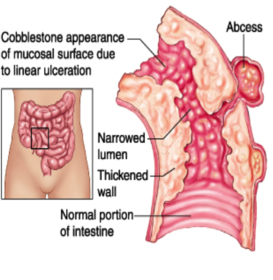
| A chronic recurrent gastrointestinal disease characterized by patchy trans mural inflammation that can involve any part of the GI tract from the mouth to anus. | Crohn’s Disease: (CD) |
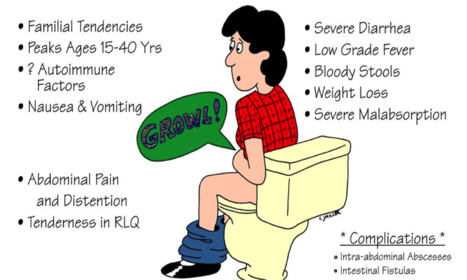
| Most prevalent in Northern states compared to Southern states in the United Sta an autoimmune disease targeting GI tract Peaks age is 15-40 years old Hereditary tendency | Crohns |
| CD results from an abnormal immune response, producing tissue damage and inflammation through all layers of the GI tract-such as abscesses, perforation and ulcerations. | Crohn's |
| crohns | |
| Crohns | |
| BILATERAL LOWER QUADRANT PAIN INSIDIOUS ONSET FEVER CHRONIC DIARRHEA WEIGHT LOSS FATIGUE MALNUTRITIONS ABDOMINAL DISTENTION AND OR MASS | SXS of Crohns |
| crohns | |
| Assess for other autoimmune related symptoms such as: joint tenderness, swelling or psoriatic lesions Detailed medical/family history Rule out other diseases that may mimic CD such as: C. difficle, lactose intolerance and celiac disease | DX of Crohns |
| #1 diagnostic procedure is a upper/lower endoscopy with biopsies of mucosa to rule out H. pylori or cancer Fact: 10% of cases difficult to distinguish ulcerative colitis from CD. Biopsies that contain granulomas highly suggest CD diagnosis. | |
| CT or MRI: to visualize bowel thicken, tissue perfusion and r/o appendicitis Labs: CBC, CMP, ESR Stool cultures: test and rule out pathogens such as C. difficle, E. coli, ova and parasites | Dx for Crohns |
| Nutritional management Well balanced diet-low fat and low roughage diet Understand food triggers Smaller meals, adequate water Vitamins B-12, probiotics Lifestyle modifications Cessetion of all tobacco use | Lifestyles Changes for Crohns |
| Nutritional management Well balanced diet-low fat and low roughage diet Understand food triggers Smaller meals, adequate water Vitamins B-12, probiotics Lifestyle modifications Cessetion of all tobacco use | TX for Crohns |
| 10-15% new diagnosis in patients older than 65 years old Less likely to present with normal symptoms and present with more weight loss, oral ulcers and anemia Correct diagnosis often delayed to due presenting as other disease processes and not as common in elderly | Geriatric crohns |
| Increased mortality when first diagnosed age 60 or greater Medication dosage may need to be reduced due to decreased GFR, hepatic elimination Common to see noncompliance due to other disease processes | Geriatrics crohns |
| Avoid NSAID/ASA Understand not curable and management only Smoking cessation is imperative Emotional support important Nutritional management huge factor with triggers Need to have regular physicals, gastroenterologist and colonoscopy's often | Patient education for Crohns |
| Which of the following stool characteristics would be present in a client diagnosed with Crohn’s disease? a. Chronic Constipation b. Diarrhea with alternating constipation c. Normal stool d. Chronic Diarrhea | Chronic diarrhea |
| Which factor is thought to be linked to Crohn’s disease? A. BMI B. Lack of exercise C. Genetics D. Gender | Genetics |
| Which associated disorder may the patient with CD present with? A. Malabsorption B. C. difficile C. Celiac disease D. Lactose deficiency | Malabsorption |
| When diagnosing a patients with CD its important to educate to follow which type of diet? A. High fat-low roughage diet B. Low fat-low roughage diet C. Low carbohydrate diet D. No change l | low fat and low roughage |
| Which of the following areas of the gastrointestinal tract is affected in CD? A. Only the rectum B. The small bowel and colon C. The colon D. The small bowel | small bowel and colon |
| Spirochete multiplys and systemactically spread. S/S. more diffused lymph nodes involvement, fever, hadache, nausea, rashes and joint pain. more central neurologival symptoms appears, such as anemia, jaundice and stiff neck, or meningitis and deaf. | Primary, secondary or tertiary |
| The spirochete eventually spreads to central nerves system, muscular skeletal system, and cardiovascular system. Syphilis encephalopathy resulted. | primary, secondary,teritary |
| Primarily focused on complete sexual history. S/s from physical exam. Serolgic tests. includes none treponemal tests and treponemal test | DX of syphilis |
| Treponemal tests: Venereal Diesase Research Laboratory(VDRL) and Rapid plasma reagin test( PPR) are to detect the presence of antibodies. often fives out false positive usually used for first line screening. Direct tests: Darkfield microscopic examination. | Labs for Syphilis |
| 1st: Plainless chancre sore and lymphadenopathy 2nd: Rashes over soles and palms, joint pain and stiff neck. 3rd: Cencephlopathy | Syphilis |
| Penicillin G 2.4 million unit,IM. ,or Docycyline 100mg BID for 4 days. ,or Ceftriaxone 1g IM for 10 days. | TX: Primary syphilis |
| Penicillin G 2.4 million unit for 3 weeks. Tertiary syphillis: Penicillin G , IV, q 3 to 4 hours for 14 days and then daily for 3 weeks. | TX Secondary syphillis: |
| educations for the usage of protective sex, such as condoms. prevention is more important than treatment. high risk people need to be screened more frequently, every 3-6 months. HIV pt also need to be screened for syphillis. | Patient Education: syphillis |
| At what stage of syphilis can neurosyphilis occur? A. primary syphilis B. Secondary syphilis C. Early latent syphilis D. any state of disease | early latent syphilis |
| Which of the following is true regarding the progression of syphilis? a. the most common clinical manifestation of primary syphilis is a chancre at the site of inoculation. b. mucocutaneous lesions may occur during secondary syphilis. c. tertiary syphilis is rare. d. all of the above. | A. |
| Which of the following is true about primary syphilis? A. a pailful chancre occurs at the site fo inoculation. B. the chancre is generally pailess and resolves without treatment C. Nontreponemal serologic tests are always postive. | A and B |
| Syphillis- what is the stage? | |
| Syphilis- what is the stage? |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.