520683
Description
Flashcards by cristydlhz, updated more than 1 year ago
|
|
Created by cristydlhz
over 10 years ago
|
|
| Question | Answer |
| What is the Roentgen sign approach? (p 85) | It involves describing abnormal radiographic morphology in terms of a change in size, shape, location, number, margination, or opacity. Number: Too many or too few Size: too small (hypoplasia vs lysis) or too big (osteoproliferation) Shape (Abnormal vs Normal variant, remodeling) Location (Proper Alignment, narrowed or widened joint space), margin/contour (periosteal proliferation, lysis), Opacity: (5 only--Gas, fat, fluid/soft tissue, mineral, metallic) |
| List the five opacities | Gas Fat Fluid/Soft Tissue Mineral Metallic |
| What could result in changes in soft tissue size? | (1) Atrophy (Disuse, Neurogenic, Intracapsular) (2) Focal Increase (Intra-capsular and extra-capsular) (3) Diffuse increase (Trauma, impaired lymphatics, vasculitis, cellulitis) |
| List the different kinds of osteolysis and rate them in increasing order of aggressiveness: | Geographic Moth-Eaten Permeative |
| What is the difference between short and long zone of transition? | Short zone of transition is distinct and long zone is indistinct. |
| What do the different bone margin lines mean? I.e., if they are easy to trace, irregular, or very irregular? | Easy to trace, regular (inactive bone)--> smooth, solid bone formation, multilayered or lamellar bone formation Irregular line (active bone)--Columnar/palisading bone formation Very irregular line (active bone)--> sunburst/spiculated bone formation, amorphous new bone formation |
| Characterize the zone of transitions in order of aggressiveness. | Tends to be more aggressive as you move from short zone of transition to long zone of transition. Long zone of transition is more aggressive. |
| Characteritize the nerve supply in the articular cartillage | There is none. |
| HOw many layers in joint capsule: | 2 layers: outer fibrous and inner synovial |
| What is the purpose of the synovial fluid | Lubrication and nutrition and waste removal from articular cartillage |
| What is purpose of articular cartillage | It is usually made of hyaline and reduces concussion and friction, no vascular or nerve supply |
| What is the purpose of the ligaments | Keep joint surfaces in apposition (in position and close together), usually inelastic and may be intra or extracapsular Intracapsular not in joint space, covered by synovium |
| What is the meniscus and what does it do? | It is a plate of fibrocartilage partially dividing the joint. It allows for a greater variety of motion in incongruent joints. It also alleviates concussion. |
| Can you characterize Degenerative Joint Disease (DJD)? What are other names for the conditions, what species are affected, etc? | Other names: Osteoarthrititis, osteoarthrosis It is Benign, non-aggressive, chronic All species are affected at all joints Almost always secondary to: Trauma, developmental, inflammation, infetion, neoplasia, immune-mediated |
| What species are affected by DJD? | All species at all joints |
| What is DJD/What can DJD be secondary to? | Trauma, deveopmental, inflammation, infection, neoplasia, immune-mediated |
| What are common radiographic signs of DJD? | Intra-capsular soft tissue swelling (joint effusion) Osteophytes Enthesophytes |
| What are occasional radiographic signs of DJD? | Intra-articular osseous bodies/joint mice Sub-chondral bone sclerosis (Wolff's Law) Sub-Chondral Bone Cyst |
| What are uncommon radiographic signs of DJD? | Decreased joint space (Weight bearing) Sub-Chondral Bone Erosions |
| How can you use the infrapatellar fat pad to evaluate synovial volume? | Usually the infrapatellar fat pad is identified as a relatively translucent triangular region immediately caudal to the patellar ligament. When stifle synovial mass increases, either from increased synovial fluid or soft tissue, a combination of inflammatory responses and effusion causes the fat pad to become less visible (it looks smaller). |
| Describe the evolution of osteoarthritis. | From a normal joint to arthritis, you have thickening of the synovial capsule and membrane and thinning of the cartilage. From arthritis to osteoarthritis, you have destruction of cartilage, ostephytes, and cartilage remnants. |
| What is the purpose of ostephytes? Where do they occur? | Osteophytes are a physiologic attempt to stabilize a joint. Articular cartilage proflieration in non-weight bearing areas of the joint, they then outgrow nutrient supply, the cartilage dies, it is invaded by vessels, and then replaced by bone. It consistently occurs at the same locations within a joint (Patterns of disease), and ostephytes occurin WITHIN a joint capsule |
| Do osteophytes occur within or outside a joint capsule? | O. occur within a joint capsule |
| What are enthesophytes? | Enthesis: origin or insertion of a tendon, ligament or joint capsule to the bone Enthesophytes: new bone at enthesis. |
| What can enthesophyte formation b secondary to? | chronic strain, trauma, or previous avulsion |
| How are osteophytes and enthesophytes different? | Ostephytes occur in the joint capsule whereas enthesophytes are outside. Although, radiographically, these are difficult to distinguish, and most often, we use the term "osteophyte" |
| What are some intracapsular mineral bodies? (Will go over a few in other lectures) | Avulsion Fragment, Joint Mouse, Synovial Osteochondroma |
| What is synovial osteochondrosis? | Rounded mineralized bodies in the joint. |
| What is the process of synovial osteochondromatosis? | Synovial membrane-->Nodular proliferation>Break off into joint space>Vascularization >Mineralization |
| What is subchondral bone sclerosis? | It is a chronic change. The bon beneath the cartilage is subject to increased stress (trabecular collapse, microfractures). Stress usually spread through articular cartilage. Damage results in stress applied directly to bone. Radiographically--> increased bone opacity |
| Subchondral Bone Cysts | Not "true" cysts (fluid or mucus filled spaces in subchondral bone) May be caused by microfractures of subchondral trabeculae Uncommon in dogs, common equine Debate continues as to whether or not this is genuinely part of DJD |
| What is joint space widening and why does it occur? | Subluxation (dislocation of joint?)--trauma induced, radiographic feature of DFD in the dog stifle and hip. May be more of an inciting cause of DJD (abnormalities of supporting structures) May need weight bearing or "stress" view |
| What are five critical components to diagnosing lameness? | 1. History 2. Physical Examination 3. Gait analysis 4. Visual inspection of body and conformation 5. Orthopedic/Neurologic Examination |
| What kinds of questions do you ask during a history? | General history and chief complaint. What leg and how severe? When first noticed? Acute vs chronic Was there trauma (HBC, fall, playing?) Progression and response to medication? (improving, static, improved then worsened)? |
| What kinds of questions should you be asking during a history? | Remember to ask open ended questions during a history but you should be thinking of the more specific questions. |
| In a general physical examination, remember to: | examine the entire patient because it may reveal other conditions |
| Gait Analysis: What should you do in general | Focus on the chief complaint, evaluate all limbs during observation, good flooring (away from owners) . But professor also gave example of doing it in front of owners in private practice. |
| Gait Analysis: Distinguish between walk, trot, and pace | Walk: 2, 3, or 4 legs support at any one time Trot: Body is supported by 2 legs on opposite sides (contralateral). Most important gait to evaluate lameness Pace: Limbs of the same side (ipsilateral) symmetrically support the animal. |
| What is the most important gait for evaluating lameness? | Trot |
| How to do you evaluate gait? | Evaluate gate towards and away. When dog is walking towards you, focus on forelimb. When away, focus on hindlimb. |
| What do you look for in a gait analysis when studying forelimb? | Once you determine that forelimb is affected, look for a "head bob". Head lifts when lame leg bears weight. Head drops when weight bearing on normal limb (down on the sound) |
| For forelimb lameness, does head bob when weight on lame leg or normal leg? | Head lifts when lame leg bears weight. |
| What are you looking at when evaluating hind limb lameness? | The stride length is shortened on the lame leg, the normal limb reaches forward much faster than the lame leg, there is an oscillating motion during locomotion (oscillation towards the normal side), and there is a hip hike on the lame leg. |
| Quantify lameness by utilizing the 0-4 scale. | Degrees of lameness: 0: no lameness 1: mild weight-bearing lameness 2. moderate weight-bearing lameness 3. severe weight bearing lameness 4. non-weight bearing lameness |
| During a visual inspection (gait analysis) to evaluate lameness, what are you looking for in terms of conformation? | Normal standing position, know breed differences, abnormal body conformation (dependent on breed) |
| During visual inspection (gait analysis/lameness), what are you looking for in? (Posture and few others) | Posture (observe stance): Look for Body Symmetry, Areas of Muscle Atrophy (around spine of scapula, greater trochanter, quadriceps) Hyperextension/Hyperflexion Limb Length Muscle Mass Varus (inward angulation of the distal segment of a bone or joint) Valgus (algus deformity is a condition in which a bone or joint is twisted outward from the center of the body) |
| During a visual inspection (gait analysis/lameness), where would you look for areas of muscle atrophy? | Spine of scapula, greater trochanter, quadriceps |
| What is the general purpose/what do you do for palpation (for gait analysis/lameness) ? | General body palpation with animal standing (check for muscle atrophy and asymmetry) |
| Valgus | Distal deviation from joint described |
| Varus | Deviation medial to joint described |
| For lameness examination, where would you palpate? | Palpate Neck (deep palpation, ventral and lateral flexion, extend neck) Palpate back (apply pressure to spinous processes down the entire length of the spine) Check for lumbosacral pain (directly palpate lumbosacral region. So, apply pressure dorsally to lumbosacral joint without loading or extending the hips). Professor actually lips the hips off the ground with knees so doesn't put pressure (pain could be from hip-dysplasia if apply pressure to that). You would also check the medial aspect of knee joint |
| For lameness exam and during palpation, what does swelling of knee joint on medial aspect mean? | This is also known as a medial buttress. It is found on the medial aspect of the stifle. It is an indicator of cranial cruciate ligament rupture |
| What can you do to check for lumbosacral disease? | You can hike the tail. Dogs that have lumbosacral disease will respond painfully to hiking the tail. |
| To localize lameness, do you start with or without sedation? | Without sedation |
| What other examination do you do along with orthopedic exam? | Neurologic exam should be done along with an orthopedic examination |
| What are two important rules for localization (when trying to identify lameness)? | Always perform orthopedic exam at the end of the evaulation and palpate the lame leg last. If you do the lame leg first, might be so painful for the dog that he will not let you continue with the rest of the examination. |
| How would you localize lameness during orthopedic examination. | Put the dog in lateral recumbency (start at the most distal part of the leg (toes)), move each joint through the full range of motion, and apply stress to joint medially and laterally (check for excess laxity) You also want to palpate bones and joints (long bone pain, palpate each joint for heat, swelling, pain), look for joint effusion, be consistent!) |
| What is an specific Orthopedic Test? | Ortolani Sign: grasp flexed stifle and apply pressure dorsally. Apply counter pressure using other hand dorsal to pelvis SIGN OF LAXITY IN HIP. Hip Laxity in dog--hip dysplasia |
| What is the Ortolani Sign--how do you know it? | You abduct limb slowly. A positive sign is if movement is felt as femoral head clicks back into acetabulum. It is diagnostic for hip dysplasia. |
| Please describe another orthopedic test: Cranial Drawer | Use both hands on one tibia and one on femur. Move tibia cranially with respect to the femur. Positive sign is: more than 1-2 mm of movement--diagnostic for cranial cruciate ligament rupture. |
| Can you please describe another orthopedic test: Tibial Compression Test | Tarsus flexed with force. Tibia translates cranially with cranial cruciate rupture. |
| Can you please describe the orthopedic test: Patella luxation | Stifle is extended. Luxate patella manually |
| What are the goals of a specific orthopedic examination? | To localize lameness Neurologic/Orthopedic Know proper diagnostics for diagnosis |
| Why would you need to perform a sedated orthopedic examination? | You might have: Aggressive dog or cat Might need to repeat specific portion of orthopedic exam Do Radiographic Assessment Do Joint Tap Perform a biopsy |
| Why would you need to perform a radiographic assesment (for orthopedic exam/lameness section)? | Diagnose localized lesion Confirm Suspected Diagnosis Rule out Disease i your differential Evaluate other potential orthopedic diseases Documentation--Medical Record |
| What is involved with client communication (for orthopedic examination/) | Plans for Diagnostics/and Threapeutics, Risks to Patient must be elucidated, Cost involved, Prognosis, Give them all options, Discuss benefits and complications (risk:benefit ratio), Prognosis, Let the client make the decision!!!! Educate them so that they can make the decision! |
| 1. How are joints classified? Give examples of joints that fit into each category. | There are fibrous joints, cartilaginous joints, and synovial joints (which provide the greatest movement) |
| What is the function of the synovial joint (aka diarthrodial joint)? | Diarthrodial Joint Supports the musculoskeletal system Permits motion while providing stability for load transfer between bones Facilitates energy-efficient, and pain-free movement External joint support is provided by surrounding ligaments and tendons |
| What is the synovial joint composed of? What is their purpose? | Intra-articular ligaments, menisci, fat pad, articular cartilage Stress reduction during weight bearing Hyaline cartilage – load-bearing surface d |
| Please characterize the different layers of the synovial joint and the vessels and nerves: | Outer layer Fibrous connective tissue Inner layer Thin subsynovium (lamina propria) Synovium (synovial membrane) In contact with the synovial fluid Nerves, blood vessels and lymphatic vessels Between the synovial membranes and the fibrous capsule Also vascularize intra-articular ligaments Cruciate ligaments are dependent on this blood supply |
| Describe the two types of synovial cells: | Synovial A cells Macrophage-like Primarily phagocytic function Secrete interleukin-1 and prostaglandin E Synovial B cells Fibroblast-like Primarily secretory Hyaluronan |
| What is the synovial membrane composed of? | Sulfated GAGs Chondroitin sulfate Structural glycoproteins Fibronectin Collagen Dendritic cells |
| What is the function of the synovial membrane? How can it be damaged and what results? | Function Regulate the entry and egress of fluids and macromolecules Inflammation, injury, sepsis Loss of integrity |
| 2. What are the components of the synovial joint and what are the functional roles of each component in maintaining joint health? | Intra-articular ligaments, menisci, fat pad, articular cartilage a. Stress reduction during weight bearing b. Hyaline cartilage – load-bearing surface Blood supply c. Arteries supplying adjacent bone Lymph vessels d. Parallel blood supply e. Regional lymph nodes Nerves f. Pain g. Locomotion h. Branch from supply to surrounding muscles i. Joints in general are heavily innervated with nerves. Not only for pain and locomotion for also for proprioception. Tells us where our limbs are in space. . |
| What does normal synovial fluid look like? | Colorless or pale yellow, viscous |
| What are components of the synovial fluid? Where is synovial fluid located? | Mononuclear cells Synovial lining cells Monocytes (mostly) Lymphocytes PMNs Ultrafiltrate of plasma Large proteins excluded Starling’s law Located in intra-articular space Neutrophils (<10%). High number of neutrophils means inflammation? Nucleated cell counts between 3000 and 5000 cells/ul. Clear or hazy pale yellow |
| What are Synovial fluid functions ? | Lubricate joint Stabilize joint Shear stress Energy absorption Nutrition Articular cartilage Intra-articular ligaments |
| What does articular cartilage look like? Where is it? | Dense white – translucent connective tissue Covers articulating joint surfaces Avascular and devoid of nerve endings Relies on synovial fluid for nutrition |
| What are some components of articular cartilage? | Hyaline cartilage, proteoglycans, GAGs, |
| Characterize hyaline cartilage: | 10% chondrocytes 90% extracellular matrix Produced and regulated by chondrocytes High percentage of water (>70% wet weight) Translucent Collagen – mostly type II Supporting scaffold Non-collagenous proteins Enzymes Proteoglycans High molecular weight Flexibility |
| Characterize proteoglycans (as part of the articular cartilage structure) | Proteoglycans Protein core to which a GAG is covalently attached Aggrecan – major proteoglycan in articular cartilage Locked into place by collagen Hold water Control the transport of molecules and ions Resist deformation Form aggregates with hyaluronan Viscoelastic Semi permeable nature of cartilage |
| Charactertize GAGS (articular-cartilage structure): | Chondroitin sulfate Keratan sulfate |
| In terms of the articular cartilage, what are some functions of the proteoglycans and GAGS? | High molecular weight Provide resilience and flexibility to connective tissue matrix Structure to cartilage |
| Characterize hyaluronan (in articular-cartilage): | Glycosaminoglycan (GAG) Present in large quantities in synovial fluid and structural component of cartillage 0.1-5 mg/ml Highly charged Provides lubrication as well as nutrition to the joints Not sulfated Not a proteoglycan No protein core Glycosaminoglycan (GAG) Present in large quantities in synovial fluid and structural component of cartillage 0.1-5 mg/ml Highly charged Provides lubrication as well as nutrition to the joints Not sulfated Not a proteoglycan No protein core Glycosaminoglycan (GAG) Present in large quantities in synovial fluid and structural component of cartillage 0.1-5 mg/ml Highly charged Provides lubrication as well as nutrition to the joints Not sulfated Not a proteoglycan No protein core Glycosaminoglycan (GAG) Present in large quantities in synovial fluid and structural component of cartillage 0.1-5 mg/ml Highly charged Provides lubrication as well as nutrition to the joints Not sulfated Not a proteoglycan No protein core High affinity for water Gives high viscosity to synovial fluid Allows fluid to support transient shear stresses Absorbs some of the energy generated by movement Boundary lubrication |
| What separates Zone 3 and Zone 4 in articular cartilage? | The tide mark |
| What are the different zones of articular cartilage (basic): | Zone 1 – Superficial or Tangential zone Zone 2 - Transitional zone Zone 3 - Radial zone Tide mark Zone 4 - Zone of calcified cartilage –anchor to subchondral bone Subchondral bone |
| Please characterize zone 1 of articular cartilage: | Zone 1 - Superficial or tangential zone Chondrocytes relatively small and flat Long axis parallel to the joint surface Collagen fibrils mostly tangential to the articular surface Withstands tension in the plane of the articular surface |
| Charactertize zone 2: transitional zone (of articular cartilage0 | Wider than the superficial zone Spherical chondrocytes and matrix with large collagen fibrils Collagen fibrils arranged in an intricate 3-D network Increased resilience to compressive loading |
| Characterize zone 3 of articular cartilage: | Largest zone Chondrocytes in short columns perpendicular to joint surface Highest proteoglycan content and the least water Collagen fibrils form a more rigid mesh that may be impregnated by crystals of hydroxyapatite in calcified cartilage Increased resilience to compressive loading |
| Characterize zone of calcified cartilage in ariticular cartilage. | Zone of calcified cartilage Separated from the preceding zones by the “tidemark” This zone anchors cartilage to subchondral bone (First area where some nerve ending/blood vessels) All nutrients going to be derived here. |
| What are the functions of articular cartilage (joint) | Facilitates gliding motion of the joint Low-friction load- bearing surface Shock absorber Buffer forces Distributes mechanical loads Prevents or minimizes injury to underlying subchondral bone |
| What is the meniscus made of and what is its function? | Fibrocartilage Distribution of joint fluid lubrication Shock absorption Load bearing Joint congruency Stabilization of joint Proprioception Prevent synovial entrapment |
| What is weeping lubrication? | Fluid trapped between cartilage surfaces |
| What happens to fluid during compression (movement) | Fluid exuded during compression Trapped between cartilage surfaces = Weeping lubrication Decreased friction |
| Joint Movement and Lubrication: What happens? Leading Edge/Trailing Edge. | Joint movement Leading edge Fluid exuded Trailing edge Fluid imbibed (sucked back up) Equilibrium reached Increased congruity of opposing articular surfaces Increase joint stability Thixotropy – ability of joint fluid to change its viscosity based on movement of the joint Load sharing within the cartilage matrix Collagen fibrils - tensile properties Proteoglycans - resist compression Loading Increased contact area Increased joint conformity Thin gel of concentrated lubricant between articular surfaces |
| For joint lubrication/movement: what is the difference between collagen fibrils and proteoglycans in terms of load sharing? | Collagen fibrils--tensile properties Proteoglycans--Resist compression |
| What is subchondral bone? What does it do? | Mixture of trabecluar and compact bone Structural support to the overlying articular cartilage Bending of the subchondral plate during loading Congruent contact of joint surfaces Stress dissipation across the joint |
| What would result in abnormal joint motion? | Ligament rupture Developmental or anatomic abnormalities Abnormal physiologic loads on cartilage Fracturing or fissuring of the cartilage matrix Disruption of the collagen fibril network Cell death |
| What is an articular fracture? What is the goal? | Due to abnormal load on the joint? Goal is for internal fixation (anatomic reduction or rigid stabilization) |
| What should you do for long bone fractures? (Joint Function/Structure PPT) | Avoid improper or prolonged immobilization |
| What is hip dysplasia? | Joint laxity!! |
| Cartilage Injury and healing: Characterize superficial lacerations and healing | Do not extend to subchondral bone No inflammatory response Chondrocyte proliferation New matrix production Incomplete repair Less efficient as animal ages NO INFLAMMATORY RESPONSE |
| Charactertize full thickness defects in cartilage injury and healing: | Full thickness defect Extends to subchondral bone Inflammatory response Fibrin and collagen Defect fills with fibrocartilage |
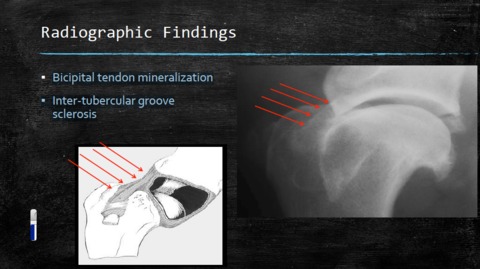
| What is bicipital tenosynovitis? Please characterize it. How can we visualize it? | Full thickness defect Extends to subchondral bone Inflammatory response Fibrin and collagen Defect fills with fibrocartilage |
| Which are lateral and which are medial? Biceps brachii, supraspinatus, greater tubercule, infraspinatus | Lateral aspect of the scapula/humerous: biceps brachhi (can see a little) and most importantly, infraspinatus Medial aspect: Supraspinatus, greater tubercule |
| What kind of radiographic view will you take for BICIPITAL TENOSYNOVITIS? | Cranioproximal-craniodistal Oblique View (“Skyline”) |
| What radiographic findings might you encounter with BICIPITAL TENOSYNOVITIS? | |
| What is polyarthropathy? | Polyarthritis is any type of arthritis which involves 5 or more joints simultaneously. |
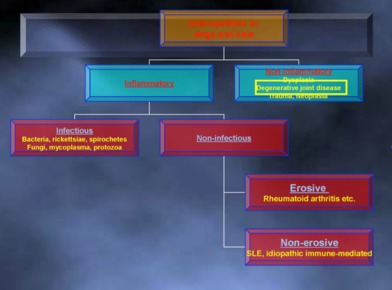
| What are the two types of polyarthropothy? | Non-Erosive and Erosive |
| Characterize non-erosive polyarthropothy: | Immune-mediated – Systemic lupus erythematous (SLE) ▪ Inflammatory – Tick borne ▪ Lyme Disease – Borrelia spp. ▪ Rocky Mountain Spotted Fever – Rickettsia spp. – Chinese Shar-pei Fever ▪ amyloidosis Inflammatory disease of joints WITHOUT articular damage ▪ Acute disease – Can be monoarticular early in disease process – Radiographic signs may not be present ▪ Chronic disease – Joint effusion – Normal bones – Tarsus, carpus and stifle most commonly affected |
| Between erosive and non-erosive polyarthropathy, which does not cause articular damage? | Non-Erosive |
| Characterize erosive polyarthropathy. What species tend to be afffected? | Results in articular cartilage damage – Usually involves the distal extremities ▪ Rheumatoid arthritis (RA) – Young to middle age small and toy breeds most commonly affected ▪ Shetland sheepdogs are predisposed – Stifles and elbows occasionally involved ▪ Feline periosteal proliferative arthritis – Young, male cats most commonly affected – Stifles, elbows, shoulders, and hips occasionally involved |
| Is Rheumatoid arthritis erosive or non-erosive polyarthropathy? | Erosive. Young to middle age small and toy breeds most commonly affected ▪ Shetland sheepdogs are predisposed – Stifles and elbows occasionally involved |
| Is Feline periosteal proliferative arthritis erosive or non erosive? (Polyarthropathy/polyarthritis) | Feline periosteal proliferative arthritis – Young, male cats most commonly affected – Stifles, elbows, shoulders, and hips occasionally involved EROSIVE |
| What radiographic findings might you find with erosive polyarthritis? | Subchondral Erosions Joint subluxation Effusion |
| Characterize septic arthritis: What animals does it occur in, adults vs juveniles | ▪ Uncommon in small animals, very common in large animals – Bacterial etiology most likely ▪ Fungal, viral, protozoal ▪ Mono-articular (adults) ▪ Direct inoculation – Puncture/perforating wound – Surgery – Poly-articular (juvenile) ▪ Hematogenous (through blood) |
| What is the process of septic arthritis? | Start with intracapsular effusion (severe)-->+- Intracapsular gas > Cartilage destruction > Joint space narrowing (7-10 d), subchondral lysis > +- concurrent DJD changes |
| What are some characteristics of joint associated tumors? | Monoarticular ▪ Location – Stifle (most common) Elbow Shoulder Carpus Tarsus Hip (less common) ▪ Differentials – Synovial cell sarcoma, histiocytic sarcoma, fibrosarcoma, chondrosarcoma, etc. |
| What are the locations for joint associated tumors? (possibly from most common to least?) | Location – Stifle (most common) Elbow Shoulder Carpus Tarsus Hip (less common) |
| What are some differentials for joint associated t umors? | Differentials – Synovial cell sarcoma, histiocytic sarcoma, fibrosarcoma, chondrosarcoma, etc. |
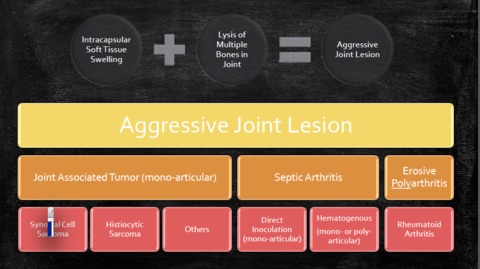
| How do you differentiate between erosive polyarthritis, septic arthritis, and joint neoplasia from each other? | |
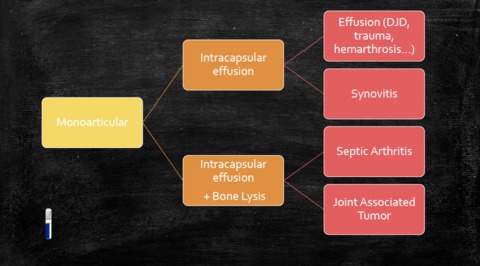
| Monoarticular problem--how do you characterize disease? (Picture with how to figure out what kind of aggressive disease you have) |
Image:
Monoarticular (image/jpg)
|
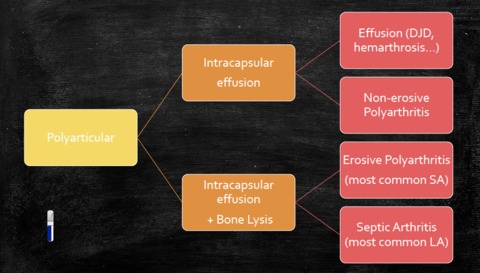
| Polyarticular problem--how do you characterize disease? (Picture with how to figure out what kind of aggressive disease you have) |
Image:
Polyarticular (image/jpg)
|
| From Lecture 5, this is a flow-chart of characterizing Arthropathies in Dogs and Cats (Two categories). Draw it out. |
Image:
Lecture5 (image/jpg)
|
| 1. Define the term osteoarthritis. | It is primarily non-inflammatory degenerative joint disease characterized by articular cartilage degeneration, marginal bone hypertrophy and synovial membrane changes. Seen in up to 20% > 1 year old. Synonyms: Degenerative joint disease (DJD) and osteoarthrosis |
| Characterize osteoarthritis: | Slowly progressive Degenerative Diarthroidal joints Confined to the joint Pain and disability Ankylosis (severe restriction and range of motion due to fibrous tissue deposition) |
| Difference between ankylosis and arthrodisis? | Ankylosis: mother nature does to stabilize the joint and arthrodis is a fusion of joint surgically |
| What is difference between primary and secondary osteoarthritis? | Primary: No identifiable cause, rare (just happens) Note: Professor note agree with this. Secondary: Known cause, common Previous trauma, joint instability, inflammation, developmental conditions, joint incongruency (more applicable to hip dysplasia) |
|
Image:
JD1 (image/jpg)
|
Image:
JD2 (image/jpg)
|
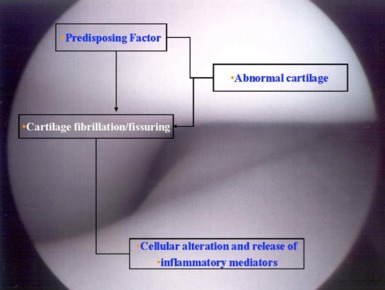
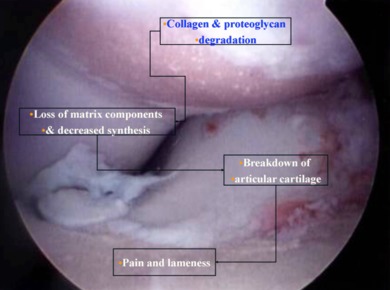
| 2. What is the pathophysiology of osteoarthritis | You have some sort of predisposing factor (like abnormal cartilage), cartilage fibrillation/fissuring, cellular alteration and release of inflammatory mediators, collagen and proteoglycan degradation, loss of matrix components and decreased synthesis, breakdown of articular cartilage, pain and lameness. |
| 3. What are the typical history and clinical signs/findings in patients with joint disease? | Clinical Signs: Pain and Lameness Variable, though. Stiffness, exercise intolerance, lethargy, visually more palpable joint effusion, lameness, pain, and disuse atrophy. Decreased joint range of motion, crepitus, muscle atrophy, muscle asymmetry. |
| What are some Radiographic Findings for Osteoarthritis? | Osteophytes and enthesiophytes, joint effusion, subchondral bone sclerosis, bone remodeling, thickening of periarticular soft tissues, cartilage destruction |
| What are five basic principles for treatment of joint disease? | 1. Weight management (Amazing how effective this is!) 2. Nutritional supplementation 3. Exercise moderation 4. Physical rehabilitation therapy 5. NSAIDS and other therapies |
| In terms of treatment of joint disease, how does weight management help? | a. Decrease load on joints, lessens and delays clinical signs of OA, may decrease the need for pain medication and surgery, BCS 4.5 recommended, Feed 80-100% RER for targeted body weight |
| Each level above the target level (for dog's body condition score) represents X percent excess body weight. | 10% |
| What is one inciting factor for OA (in terms of weight management) ? | Obesity |
| What is the difference between arachidonic acid and dihydroxyeicosapentaenoic acid? | Arachidonic--pro-inflammatory Dihdry--not pro inflammatory |
| Treatment of Joint Disease: Nutritional Supplementation: What is a major supplement (lots of evidence for)? | Omega-3 FA (replace arachidonic acid with dihydroxyeicosapentaenoic acid) to Decrease pain and inflammation |
| Treatment of Joint Disease: Nutritional Supplementation: Examples of weak nutrient supplementation (not used so much) | Green lipped mussel preparation, P54fP Tumeric Extract, Boswelia Serrata Extract |
| Treatment of Joint Disease: Nutritional Supplements: What re some of the benefits of Chondroprotectives/DMOA | Suggested benefits include : Chondroprotectives/DMOA (not hugely strong evidence for this) Some suggested benefits include: Promote cartilage matrix synthesis, slow cartilage breakdown, decrease breakdown products, some have anti-inflammatory effects. DMOA (Disease modifying osteoarthritic agent) |
| What are some examples of chondroprotectives and how do they work? | Chonroitin Sulfate: GAG, cartilage component PSGAG--GAG, cartilage component Hyaluronic acid: Increased Viscosity and anti-inflammatory Manganese: Co-factor for GAG synthesis (good for cross-linking) Ascorbate: Free radical scavenger and required for collagen cross-linking. Dogs make it in the liver!!!! |
| Treatment of Joint Disease: Supplement: Chondroprotective. Be careful of what? | Over the counter oral products. FDA Approved--Adequan-PSGAG, Cosequin (oral)-GAG, CS, Ascorb, MAn, Glycoflex (oral) GAG |
| What are some contraindications for chondroprotectives? | Oral has a few side effects (GI upset most common) PSGAG (Heparinoid-like activity, can decrease platelets, and can promote bleeding!!!!!) |
| Can you characterize the chondroprotective pentosan polysufate? | Antithrombotic/lipidemic agent Approved to treat interstitial cystitis in humans |
| Treatment of Joint Disease: Controlled Exercise: Purpose and how do you approach this? | Correct abnormalities, gradual introduction, Consistent Activity (avoid inactivity and extreme activity), Rehabilitation (like underwater treadmill) |
| Treatment of Joint Disease: Physical Rehabilitation Therapy: What does it do? How does it work? Benefits? | Increase muscle strength and endurance, increase joint range of motion, decrease edema, promote tissue repair and metabolism, and decrease muscle spasms and pain |
| Treatment of Joint Disease: Medical Therapy: What kinds of therapy would you use? | NSAIDS, steroids, antimicrobials, other agents |
| Treatment of Joint Disease: Medical Therapy: What is most commonly used agent? What are benefits of this? | NSAIDS: Most common means of OA management and can be used as needed or continuously It reduces pro-inflammatory mediators (e.g. thromboxanes, prostaglandins, prostacyclins and oxygen radicals) by inhibiting cyclooxygenase 1 and 2 (COX-1 and COX-2) and lipooxygenase pathways Effective for 2 week period and then tapers off. |
| Treatment of Joint Disease: NSAIDS inhibit XXX | COX 1 and COx 2 |
| Treatment of Joint Disease: NSAIDS: Use Ibuprofen and Naproxen? | NOOO!!!! Stay away. |
| Treatment of Joint Disease: Example of COX Non-specific NSAIDS | Aspirin, phenylbutazone, ibuprofen, naproxen |
| Treatment of Joint Disease: Examples of COX-2 Preferential NSAIDs | Carprofen, Etodolac, meloxicam (good for small dogs) |
| Treatment of Joint Disease: NSAIDS: Examples of COX-2 selective | Deracoxib, firocoxib |
| Treatment of Joint Disease: NSAIDS: Cox and Lipoxygenase inhibition | Tepoxalin |
| Treatment of Joint Disease: NSAIDS: List Counterindications | Gastrointestinal ulcers/GI upset Nephrotoxicity Hepatotoxicity-Carprofen Keratoconjunctivitis sicca-Etodolac (Liver disease Kidney disease G.I. disease Bleeding tendencies ) |
| Treatment of Joint Disease: NSAIDS: Counterindication for Carprofen | Hepatoxicity |
| Treatment of Joint Disease: NSAIDS: Counterindication for Keratoconjunctivitis | Etodolac |
| Treatment of Joint Disease: Steroids: What do they do? Include counter indications | Inhibit Phospholipase A2 Decrease catabolic activity in the joint (Metalloproteinase may protect cartillage) Decrease synovial inflammation Counterindications: Can decrease collange and proteoglycan synthesis and matrix proteoglycan content, adverse systemic effects |
| Treatment of Joint Disease: Other Potentially useful agents: Analgesics | Tramadol: Opiod analgesic Weak inhibition of opioid receptors Can combine with NSAIDS Effects serotonin release and re-uptake AMANTADINE: combine with NSAID, inhibit NMDA receptor GABAPENTIN: can combine with NSAIDS, block voltgage gated Ca channels AMITRIPYTLINE: No clinical trial in dogs, antidepresant |
| How can you diagnose septic arthritis? | Take sample of joint fluid and synovium. Bacterial culture, suceptibility testing, identify causative organisms |
| How do you medically manage septic arthritis? What are your options? | 1. Antimicrobials only 2. Antimicrobials and surgical lavage 3. antimicrobials and arthroscopic lavage 4. antimicrobials and lavage and drain placement 5. antimicrobials and open joint management (SEVERE CASES and rare?) |
| Septic Arthritis: Medical Management: Describe antimicrobial therapy : When? How long? | Administer immediately after samples are taken. Alter based on suceptibility results. Treat 4-6 weeks (LONG!), 2 weeks after resolution of clinical signs Gram positive--(most common)--so use first generation cephalosporim. Doxycylie. |
| Treatment of Joint Disease: Non-Erosive Polyarthritis: Idiopathic Immune Mediated. How would you treat? | Medical treatment: Prednisone, azathiprine (myelosupression), cyclosporine (myelsupression), Cyclophosphamide (therapeautic drug monitoring) |
| Treatment of Joint Disease: Non-Erosive Polyarthritis: Systemic Lupus Erthematosus | Medical Treatment: Prednisone Prednisone and Levamisole Cyclosporine Cylophosphamide Chlorambucil in cats |
| Treatment of Joint Disease: Erosive Polyarthritis: How would you treat rheumatoid arthritis? | Combination of immuno-supressive drugs with or without arthrodesis |
| Treatment of Joint Disease: Erosive Polyarthritis: How would you treat feline chronic progressive polyarthritis? | Prednisolone, chlorambucil |
| Treatment of Joint Disease: Discuss surgical treatment | Joint prosthesis, excision arthroplasty, arthrodesis, joint debridement, joint stabilization, amputation Arthroplasty--FAO is another word for this? Can't arthrodes the hip |
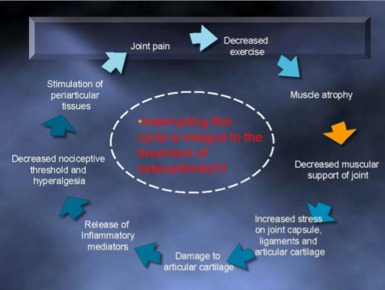
| Treatment of Joint Disease: Please describe the cycle that must be interrupted in order to treat osteoarthritis | |
| How does normal bone develop? (Normal Bone development) | You start with the fetal skeleton which is composed of cartilage. The cartilage cells replaced by osteoclasts and osteoblasts. Then there is mineralization and resorption of cartilage (replaced by bone). Then start forming growth plates. Primary Ossification Center (Compact bone) and also a secondary ossification center (Cancellous bone) |
| How does longitudinal bone growth occur? | • Endochondral ossification • Epiphyses of Immature Bone Develop as Centers of Ossification • Joint Side • Articular-Epiphyseal Cartilage Complex • Grows as the Epiphysis Enlarges • Maintains Shape of Bone Ends • Articular Surface Remains Cartilaginous Throughout Life Longitudinal bone growth • Metaphyseal Side • Physeal Growth Plate (Physis) • Longitudinal bone growth • At skeletal maturity-ossifies and growth ceases |
| 1. What is endochondral ossification? | Orderly calcification, vascular invasion by osteogenic granulation tissue and replacement of cartilage by bone tissue The process by which bone is formed is termed osteogenesis or ossification. Bone is never formed as a primary tissue: it always replaces a preexisting support tissue. There are two types of bone formation: intramembranous and endochondral ossification. Endochondral ossification involves the replacement of a cartilage model by bone. This ossification process can be studied in the long bones, such as the bones of the limbs. In a typical adult long bone, one can distinguish grossly a cylindrical shaft or diaphysis of compact bone (with a central marrow cavity) and, at the ends of the shaft, the epiphyses, each consisting of spongy bone covered by a thin peripheral shell of compact bone. In the growing long bone, the epiphysis and the diaphysis are united by a transitional zone called the metaphysis. |
| What happens to chondrocytes in the former proliferative zone of articular cartilage and the diffuse zone of calcified cartilage during endochondral ossification? | At maturity - chondrocytes in the former proliferative zones of articular cartilage now function to maintain the joint surface and transfer energy to the underlying subchondral bone The diffuse zone of calcified cartilage narrows to a thin zone that is only a few chondrocytes in thickness |
| What is osteochondrosis (OC)? | • Developmental orthopedic disease • Disruption of EO • Osteochondral junction • Focal area on developing articular cartilage • Failure of calcification • Thickened focal area of degenerating cartilage |
| Which growth plates can osteochondrosis affect? | • Can Affect Any Growth Plate • Articular-Epiphyseal Complex • Metaphyseal • Apophyseal |
| Osteochondrosis: Pathogenesis: Characteristic the disturbance of endochondral ossification | • Failure of Matrix Calcification and Vascular Ingrowth • Cartilage Retention Results in Thickening of the Articular Epiphyseal Cartilage |
| Briefly talk about the pathogensis of osteochondrosis: | • Disturbance of Endochondral Ossification • Failure of Matrix Calcification and Vascular Ingrowth • Cartilage Retention Results in Thickening of the Articular Epiphyseal Cartilage • Thickened Articular-Epiphyseal Cartilage Complex: • Poor Diffusion of Nutrients From Synovial Fluid • Necrosis at Deep Portion of Thickened Cartilage– Susceptible to Trauma • Abnormal Arrangement, Metabolism, Function of Chondrocytes • Matrix Molecules Become More Like Articular Cartilage • Which Does Not Undergo Endochondral Ossification • Separation Between Noncalcified and Calcified Layers (Tidemark) • Cartilage Flap = Osteochondritis Dissecans (OCD |
| 3. What is the difference between osteochondrosis (OC) and osteochondritis dissecans (OCD)? | OCD is when you get a cartilage flap |
| What is the separation between non-calcified and calcified layers called? | Tidemark |
| Osteochondrosis: What can happen with the cartilage flap? | (1) • Flap May Reattach to Subchondral Bone • Bleeding into the Defect Brings Mesenchymal Cells (2) • Vertical Fracture of Articular Cartilage May Form (most of the time) • Minimal Trauma / Motion of Flap During Weight-Bearing • Irritation Causes Synovitis – Pain, Lameness, OA • Synovial Fluid in Defect Prevents Healing (3) • Fragments May Detach - Joint Mice • Joint Irritation • May Resorb • May Enlarge Due to Nutrition From Synovial Fluid |
| What are causes of osteochondrosis? | No one really knows but there are speculations: Trauma, anatomical factors, hormonal factors, over nutrition, rapid growth rates, heredity, ischemia, lipid metabolism defect in cartilage |
| Causes of osteochondrosis: Characterize Trauma | • Known Cause of Osteochondrosis in Humans • Ischemia of Subchondral Bone in Humans (Not Dogs) • Occurs in Areas of Biomechanical Stress • Repeated Microtrauma • May Simply Contribute to Flap Formation and Clinical Signs |
| Osteochondrosis Etiology: Characterize Anatomical Factors | • Canine Humeral Head - Caudal Cartilage Normally Thicker • Caudal Medial Aspect Develops More Slowly • More Susceptible to Microtrauma From Glenoid |
| Osteochondrosis Etiology: Characterize Hormonal Factors | • Excess Growth Hormones • Somatotropin and Thyrotropin Cause Lesions Similar to OC • Hormonal • Testosterone • Stimulates Epiphyseal Growth • Synergistic With Growth Hormones • Delayed Endochondral Ossification • Incidence Higher in Males • Estrogen • Encourages Cartilage Calcification |
| Osteochondrosis: Etiology: Characterize over nutrition | • Excess Dietary Calcium • Inhibits Cartilage Maturation • Free-Fed Great Danes – OC Lesions |
| Osteochondrosis: Etiology: Characterize Rapid Growth Rate | • During Periods of Rapid Growth • Species and Breeds With Rapid Growth Rates |
| Osteochondrosis: Etiology: Characterize heredity: | • Familial Tendency • Definitive Evidence of Heritability Unproven? • Dogs: • Certain Breeds Predisposed • Dogs With Adult Weights >20 kg |
| Osteochondrosis: Etiology: Characterize ischemia | • Abnormal Blood Vessels Noted in Some Species (Pigs, Horses, Humans) • Lead to Cartilage Necrosis • Ischemia May Be Related to Rapid Growth Rate |
| Ischemia (Abnormal Blood vessels) has been noted in which species: | Pigs, horses, humans |
| Osteochondrosis: Etiology: Characterize lipid metabolism | Might delay cartilage calcification |
| When is period of rapid growth in dogs? | 4-8 months in dogs (later for larger dogs) |
| How would you diagnose OCD? | • Signalment • History • Physical and orthopedic examination findings • Neurological examination • Radiography ± arthrogram • MR, CT, bone scan |
| 5. What breeds are commonly affected by OC ? | a. Free-fed great Danes (OC Lesions) (weak evidence?) b. Horses seem to be much greater causal relationship between diet and OC (no real ) c. Rapidly growing large-giant breed male dogs d. Dogs with high planes of nutrition e. Occurs during periods of rapid growth f. German Shepherds |
| True or False: Is OCD bilateral? | Yes, it often is bilateral disease! So radiograph both joints!!!!!!!!!!!! |
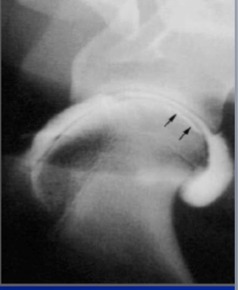
| What is the signalment, usually, for dogs affected with shoulder OC? And where is the subchondral bone defect? | • 5-10 months of age • Males > females • Ratio 2:1 to 6:1 • 20-85% bilateral • Both limbs equally affected • Subchondral bone defect in the caudal aspect of the humeral head |
| When looking at a shoulder, what are you looking for to confirm shoulder OC? Subchondral bone defect! |
Image:
Shoulder_OC (image/jpg)
|
| What clinical signs will you see with a dog who has shoulder OC? | • Mild to moderate unilateral forelimb lameness • Gradual onset lameness • Lameness improves after rest and worsens with exercise • Affected limb externally rotated and elbow abducted • Joint effusion • Mild atrophy of the supraspinatus, infraspinatus and deltoideus muscles • Pain on hyperextension and flexion of the scapulohumeral joint |
| How do you treat a dog with shoulder OC? Discuss the options | • Medical management • < 7 months old • Small radiographic lesions • No joint mice • No clinical pain • Surgical management • Persistent lameness • > 6 weeks • Presents with pain and lameness • Flap present • > 8 months old • Large lesion • Joint mice present |
| Discuss medical management of dog with shoulder OC: Age?>? | • < 7 months old • Small radiographic lesions • No joint mice • No clinical pain |
| Discuss surgical management in a dog with shoulder OC: | • Surgical management • Persistent lameness • > 6 weeks • Presents with pain and lameness • Flap present • > 8 months old • Large lesion • Joint mice present |
| What is the typical signalment of elbow OC in a dog? | • Clinical signs < 1 year of age • Lameness at 5-7 months of age • Males > females • Ratio 2:1 • 20-50% bilateral • Both limbs equally affected • Radiolucent concavity on the distal trochlear ridge of the medial aspect of the humeral condyle • CT can enhance diagnosis |
| Where do you typically find/look for defect for shoulder OC in dog? | • Subchondral bone defect in the caudal aspect of the humeral head |
| Where do you typically look for Elbow OC in dog? | • Radiolucent concavity on the distal trochlear ridge of the medial aspect of the humeral condyle |
| What are clinical signs of elbow OC? | • Mild or intermittent lameness • Lameness worse after rest and worsens with exercise • Affected elbow slightly adducted • Joint effusion • Pain on extension and lateral rotation of the elbow • Crepitus on palpation • Decreased ROM particularly during flexion |
| What is a tip-off that dog has elbow OC? | Affected elbow slightly adducted |
| How would you medically manage elbow OC? | • Medical management • < 7 months old • Small radiographic lesions • No joint mice • No clinical pain |
| How do you medically treat elbow OC? | • Persistent lameness • Presents with pain and lameness • Flap present • > 8 months old • Large lesion • Joint mice present |
| 7. List the joints and specific anatomical locations within the joints where OC is commonly seen. | • Elbow OC: Radiolucent concavity on the distal trochlear ridge of the medial aspect of the humeral condyle • Shoulder OC: Subchondral bone defect in the caudal aspect of the humeral head Hock: • Subchondral radiolucency on the medial trochlear ridge of the talus – 79% • Stifle: • Flattening of the subchondral bone on the medial aspect of the lateral femoral condyle |
| 8. What is the incidence of OC in the joints that are commonly affected? | Elbow OC: Not very common. 20-50% bilateral. • Shoulder: 20-85% bilateral Stifle: 76% of dogs, 72% bilateral (both limbs equally affected) • Hock: 40% bilateral • > 70% of cases seen in Rottweilers and Labrador Retrievers |
| What are clinical signs of stifle OC? | • Gradually developing intermittent lameness • Lameness worse after exercise • Disuse muscle atrophy • Joint effusion • Pain and crepitus on manipulation of the joint • Decreased ROM particularly during extension • Crouched stance if the disease is bilateral |
| What is a difference in clinical signs for stifle OC? | • Crouched stance if the disease is bilateral |
| Describe medical management in stifle OC | • Small radiographic lesions • No joint mice • No clinical pain |
| Describe surgical management in stifle OC: | • Persistent lameness • > 6 weeks • Presents with pain and lameness • Flap present • > 8 months old • Large lesion • Joint mice present |
| Characterize Hock OC: Signalment | • Lameness at 5-7 months of age • Males = females • 40% bilateral • > 70% of cases seen in Rottweilers and Labrador Retrievers |
| What breeds are typically affected by hock OC? | Rottweiler and Labrador Retriever |
| (Osteochondrosis lecture): A hind limb lameness in a large breed dog is usually: | Cruciate ligament lameness? |
| What are clinical signs of hock OC? | • Intermittent non-weightbearing lameness • Exercise intolerance • Signs progressive and usually of several months duration • Hyperextension of the affected tarsal joint • Crepitus on palpation • Decreased ROM |
| Where do you tend to see Hock OC? | • Subchondral radiolucency on the medial trochlear ridge of the talus – 79% • Lesion usually on the plantar aspect of the ridge |
| How would you clinically manage HOCK OC? | • Medical management • Older dogs with severe DJD • Small radiographic lesions • Mild lameness |
| How would you surgically manage HOCK OC? | • Early intervention • Minimally invasive approach • Overdebridement of the defect will lead to joint instability |
| What is the prognosis for Shoulder OC? | Very good to excellent 75% of dogs no lameness postoperatively |
| What is the prognosis for elbow oC? | Good DJD progresses after medical management or surgical management |
| What is the prognosis for stifle OC? | Guarded Progression of DJD common |
| What is the prognosis for tarsus OC? | Poor Moderate to severe lameness persists even with surgical intervention |
| What is the prognosis for various Joint OC? | |
| In general, how do we treat OC? | • Used for small lesions • Strict cage rest for 4-6 weeks • NSAIDs • DMOAs • Restricted diet • Decrease caloric intake and stop calcium supplementation |
| What is to "forage"? (OC lecture) | To put a hole in a bone to improve vascularization |
| What is the general surgical treatment for OC? | More rapid return to function and minimizes the development of OA • Surgical disease • Aims • Remove cartilage flap or joint mice • Remove non-adherent cartilage in periphery of the lesion • Stimulate defect to heal by fibrocartilage formation • Curettage • Forage • Abrasion arthroplasty Surgical treatment • Arthrotomy • Prefer muscle separating approaches • Limited exposure of the joint • Arthroscopy • Less invasive • Complete exploration of the joint • Excellent lavage • Technically more difficult • Specialized equipment and training Arthroscopy |
| Compare arthrotomy and arthroscopy: | • Arthrotomy • Prefer muscle separating approaches • Limited exposure of the joint • Arthroscopy • Less invasive • Complete exploration of the joint • Excellent lavage • Technically more difficult • Specialized equipment and training |
| Talk about the prognosis for shoulder, stifle, elbow, and tarsus osteochondrosis | |
| Where can the OATS procedure be applied?! (OS) | Stifle !! |
| What is the OATS procedure? | • Osteochondral Autograft Transfer System • Transfer articular cartilage and subchondral bone from one site to the other in the same patient |
| For OS surgery (osteochondrosis), what are some post-operative care consideratiins and what are some complications? | • Postoperative care • Limited activity for 4 weeks • ± Modified R-J bandage • Mild physical therapy • PROM exercises; swimming • Leash walks • Complications • Seroma • Wound dehiscence • Infection • Chronic lameness |
| Juvenile Bone Disease: What are some radiographic signs for OC? | Flattening or concavity of the subchondral bone •Surrounding subchondral bone sclerosis •Cartilage flap may be mineralized –Joint “mouse” •Separate osteochondral fragment •May attach to synovium and enlarge over time •Subchondral bone defect on opposite articular surface sometimes present –“kissing lesion” •Joint effusion •Secondary DJD |
| What is a kissing lession? | When a subchondral bone defect is seen involving the articular surface opposite the primary lesion. |
| Juvenile Bone Disease: How can you distinguish OCD and OC? | Separation of the abnormal flap of cartilage from the subchondral bone (OCD) •Usually cannot determine from survey radiographs –Arthrogram –CT •*** If mineralized cartilage flaps are not seen radiographically, the term osteochondrosis should be used *** |
| Juvenile Joint disease: What are common sites of OC (canine)? | Common Sites (canine): –Shoulder •Caudal humeral head –Elbow •Medial aspect of humeral condyle –Stifle •Lateral > Medial femoral condyle –Hock •Medial > Lateral ridge of the talus |
| Is Fibula lateral or medial? | Lateral |
| Is radius medial or lateral? | Radius is medial. (Ulna like hook) |
| What are some developmental conditions that lead to elbow DJD? (Elbow Dysplasia): | Several developmental conditions that lead to elbow DJD –Ununited anconeal process –Fragmented medial coronoid process –Osteochondrosis of the medial humeral condyle –Joint incongruity •Asynchronous growth of the radius/ulna •One or more may be present •Usually bilateral |
| For Juvenile Bone Disease: What breeds are at risk for Ununited Anconceal Process? | At risk breeds: –Bernese Mountain Dogs –Mastiffs –Rottweilers –Saint Bernards |
| What are the Roentgen Signs for a dog with ununited anconeal Process (UAP) | Radiolucent line b/w anconeal process and olceranon in dogs older than 5 months Takes at least 5 months for it to fuse normally!!! |
| What does Ununited Anconeal Process look like? | |
| What kind of view would you take to look at ununited anconceal process in a dog? And is this uni or bilateral (the condition)? | Flexed lateral view in addition to regular views Bilateral |
| Juvenile Bone DZ: Characterize fragmented medial coronoid process | Most common developmental disorder •Often bilateral •Difficult to visualize fragment radiographically –CT •Sometimes presumed based on degenerative changes AND no evidence of UAP or OC |
| What are some Roentgen signs associated with fragmented medial coronoid process? | Earliest signs associated with osteoarthritis •Development of osteophytes on the anconeal process and radial head •Sclerosis of the trochlear notch of the proximal ulna |
| How many physis does the ulna have? | One |
| Radius/Ulna Asynchronyous Growth (Elbow Dysplasia): How manny physes does ulna have? What about its growth? | The ulna has only one physis distal to the elbow •Growth from this physis must equal the growth from both radial physes |
| What happens with premature ulnar physis closure? | Distal ulnar physis susceptible to trauma because of conical shape •Possible sequelae: –Radius curvus (bowed radius) –Humeroulnar subluxation |
| What is ULNAR OSTECTOMY? | Cut out portion of ulna, lets space fill with bone. |
| Characterize premature radial physis closure: | Not as common as ulnar closure •Humeroradial subluxation |
| Characterize Panosteitis: What breeds get it? Which bones affected? | Self-limiting disease •Long bones of young, large breed dogs •At risk breeds: –Basset Hound –Shar-Pei –Giant Schnauzers –German Shepherds •Most often seen between 5-12 months of age •Males more commonly affected |
| Age range for dogs that develop panosteitis? | Most often seen between 5-12 months of age |
| What are early Roentgen Signs for dogs with Panosteitis? | Increased intramedullary opacity •Usually seen in the diaphysis near the nutrient foramen •Blurring of the trabecular pattern |
| What are late Roentgen signs of Panosteitis? | Medullary opacities become better delineated giving a patchy appearance •Smooth periosteal reaction may be seen on the adjacent cortex |
| Increased intramedullary opacity •Usually seen in the diaphysis near the nutrient foramen •Blurring of the trabecular pattern | |
| •Medullary opacities become better delineated giving a patchy appearance •Smooth periosteal reaction may be seen on the adjacent cortex | |
| Characterize hypertrophic osteodystrophy (HOD): What breeds, age, etc? | Large, rapidly growing dogs •At risk breeds: –Boxer –Great Dane –Irish Setter –Weimaraner •2-7 months of age •Usually self-limiting –If severe premature physeal closure •Definitive etiology not known |
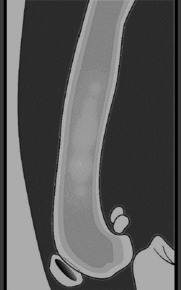
| What are the Radiographic findings for HOD (hypertrophic osteodystrophy)? | •Bilaterally symmetrical lesions •Metaphyses of the distal radius, ulna, and tibia most commonly affected •Early Stage –Soft tissue swelling adjacent to physis –Linear irregular lysis adjacent, and parallel, to physis •Physis preserved •“Double physis” sign •Intermediate Stage –Marked metaphyseal periosteal reaction due to sub-periosteal hemorrhage •Late Stage –Periosteal new bone blends with cortex and |
| What are the three different stages for HOD (Radiographic findings): Hypertrophic osteodystrphy | Early Stage –Soft tissue swelling adjacent to physis –Linear irregular lysis adjacent, and parallel, to physis •Physis preserved •“Double physis” sign •Intermediate Stage –Marked metaphyseal periosteal reaction due to sub-periosteal hemorrhage •Late Stage –Periosteal new bone blends with cortex and remodels to normal shape |
| What is a key radiographic finding to HOD (HYPERTROPHIC OSTEODYSTROPHY (HOD) | "Double Physis" Sign in Early Stage. Linear irregular lysis adjacent and parallel to the physis |
|
Image:
Double_Physis (image/jpg)
|
Note the irregular shaped linear area of lucency adjacent, and parallel, to the physis |
| What is retained cartilaginous core? | Disruption of normal endochondral ossification –Temporary inadequate blood supply to metaphysis central core of cartilage not transformed to bone •Large breeds commonly affected •May cause angular limb deformity –Cartilage retention can lead to asynchronous ulnar growth |
| What are radiographic signs of retained cartilaginous core? | Cone-shaped radiolucent area –Distal ulnar metaphysis (most common) –Narrow zone of adjacent sclerosis |
| What is the most common cause of hind limb lameness in the dog? | Cranial cruciate ligament rupture |
| What are the three types of cranial cruciate ligament ruptures? | Complete tear, partial tear, and avlusion |
| Functions of the CCL | Limits cranial translation of the tibia with respect to the femur Cranial drawer motion Cranial tibial thrust Prevents hyperextension of the stifle joint Limits internal rotation of the tibia Limited degree of valgus-varus support to the flexed stifle Mechanoreceptors – proprioceptive feedback |
| What is the typical signalment for an animal with CCL rupture? | Either gender Any age or breed Higher incidence in females Young to middle-aged Active Large breeds Seen less frequently in small breeds Straight-legged Mastiff, Chow Chow, Akita, Labrador retriever, Rottweiler, St. Bernard, Newfoundland Occasionally seen in cats |
| What is the etiology for CCL rupture? | Uncertain but Chronic degenerative changes Acute trauma Conformation |
| Characterize the etiology of acute trauma and chronic degenerative changes for CCL rupture: | Acute trauma Small percentage of dogs Acute history Distinct traumatic event Avulsion in young dogs Typically failure of the tibial attachment site Chronic degenerative changes Episodic lameness Declining strength of CCL with age Loss of fiber bundle organization and metaplastic changes of cellular elements More marked in central core of ligament |
| Charactertize conformation abnormalities as as a cause for CCL rupture | Conformation Postural arthosis Stifle hyperextension Straight rear limbs Femoral conformation Narrowing of intercondylar notch Tibial conformation Internal rotation Abnormal slope of TPA (increased TPA) Anatomy Posture Obesity Excessive stress on CCL Chronic deterioration Eventual rupture |
| For CCL rupture, how do you distinguish between acute and chronic injury and partial tears? | During the history: Acute injury – sudden onset non-weight bearing lameness followed by improvement May not improve if there is a concurrent meniscal injury Chronic injury- prolonged weight-bearing lameness Difficulty rising and sitting Sit with the affected limb out to the side of the body Partial tear Mild weight bearing lameness associated with exercise May resolve with rest May last for months May have bilateral injury Differentiate from neurologic disease |
| If you hear a click during walking or on stifle flexion, this is suggestive of: | A meniscal injury |
| What may you find during physical examination of dog with CCL rupture? | Pain Cranial drawer motion (may cause discomfort) Tibial compression test Joint effusion Periarticular fibrosis Medial buttress Posture during sitting Weight shifting during standing Thigh muscle atrophy Crepitus during joint flexion and extension May need to sedate or anesthetize to complete examination Compare with opposite limb if unsure Click” during walking or on stifle flexion and extension is suggestive of meniscal injury Absence of joint noise does not rule out a meniscal injury Always assess collateral stability |
| Craniomedial and craniolateral band in CCL | Craniomedial band Taught in extension and in flexion Caudolateral band Taught in extension Relaxed in flexion |
| True or False: Fractures usually require blocking | False. Usually have localizing signs that make blocking unnecessary |
| What are some symptoms for fractures of the 3rd phalanx? (P3) | Acute lameness (3/5) Positive to hoof testers Increased digital pulse +/- Coffin joint effusion |
| What is one way to diagnose P3 fractures? | Radiographs, though may not show up for 10-14 days (lysis along the fracture line) |
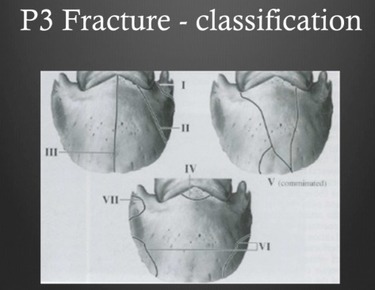
| Be slightly be familiar with P3 Fracture classification. | |
| How would you treat P3 fractures? This depends on the type of fracture. | Types I, II, III, V: Immobilize the hoof wall. Shoeing cast. Call surgeon? Types II, III, IV: Lag screw but difficult Type IV: Surgical, Removal, Lag |
| Treatment for Type 4 fracture on P3? | Can do removal/surgery |
| What is the prognosis for P3 Fractures? | Types I, II: Good Type III, IV: Guarded-Fair Type V: Good (trauma), Guarded (Osteomyelitis), Type VI: Excellent Depends on: Extend of articular involvement, Presence of sepsis May need to do PD neurectomy after complete healing I and II (farther back on the side of foot)--do OK. 1--non articular, treat with shoe. Not part of shoe. most foals will actually have these. Very common 2--because far out on edges of articular surfaces, tend to do better than type 3, which are right in the middle of articular surface. 4--extensor process. bigger are, lower prognosis is. because of problems with extensor tendons. bigger they are, harder the repair 5--commonnuded ones? if can keep clean, will do better. if infected, prognosis goes down. 6--solar margin, down at edge of bone. Those are really simple fractures. Have a great prognosis because once get bone chip out, they heal and do really well. Like an abscess just jacked up on steroids. Occasionally, do neurectomy to make more comfortable. Won't know if you will have to do this until horse has had time to heal. Even though II is inatraartciuar surface--on the side. The 3's are in the middle--so more useful and important region of weight-bearing. 4--depends on size more likely. 5--once get infected, goes downhill. Type 6--solar margins most likely. I and II (farther back on the side of foot)--do OK. 1--non articular, treat with shoe. Not part of shoe. most foals will actually have these. Very common 2--because far out on edges of articular surfaces, tend to do better than type 3, which are right in the middle of articular surface. 4--extensor process. bigger are, lower prognosis is. because of problems with extensor tendons. bigger they are, harder the repair 5--commonnuded ones? if can keep clean, will do better. if infected, prognosis goes down. 6--solar margin, down at edge of bone. Those are really simple fractures. Have a great prognosis because once get bone chip out, they heal and do really well. Like an abscess just jacked up on steroids. Occasionally, do neurectomy to make more comfortable. Won't know if you will have to do this until horse has had time to heal. Even though II is inatraartciuar surface--on the side. The 3's are in the middle--so more useful and important region of weight-bearing. 4--depends on size more likely. 5--once get infected, goes downhill. Type 6--solar margins most likely. |
| What is a common etiology of 2nd phalanx fractures? | Sudden stops and turns on supported leg. |
| How would you diagnose 2nd phalanx fractures? | PE, Radiographs, Sudden acute lameness. Most are going to be grade 5/5. |
| How would you apply first-aid to horse with a P2 fracture? | You could use a bandage with a splint. Straighten the fetlock. Keep the fetlock from moving. Horse walk on toe, refer! Kimzey Splint: Metal splint that wraps around leg. What it does is the horse actually walks on the metal shoe and it transfers weight bearing to upper part of limb. Distal limb. You can also put these horses in a cast, PVC, anything that is solid enough. Broom handle is NOT enough. 2X4. Refer--get some place else!! |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.