5261549
Description
Flashcards by Brianne Schmiegelow, updated more than 1 year ago
|
|
Created by Brianne Schmiegelow
over 9 years ago
|
|
| Question | Answer |
| What are the 3 themes seen in the evolution of gas exchange? | 1. Expansion of surface area for gas exchange 2. Development of efficient ventilatory or pumping mechanisms 3. Evolution of respiratory pigments |
| What would happen if gas exchange systems did not evolve? | There would be severe constraints on size and metabolism so they could not be >0.5-1 mm |
| How many alveoli are there in each lung? | 300 million |
| How wide are alveoli? | 0.2 mm in diameter |
| What is the respiratory surface area? | 50-100 m^2 (vs. <2 m^2 in the rest of the body) |
| What separates air from the blood? | 2 thin cells 1 alveolar, 1 endothelial |
| How much blood is in the pulmonary capillaries? | 60-140 mL spread over the surface area of 50-100 m^2 |
| What causes the alveoli and the lungs to tend to collapse? | Elasticity and surface tension |
| What is the distribution of recoil force? | Elasticity = 1/3 Surface tension = 2/3 |
| How are the lungs kept inflated? | The pressure in the intrapleural spaces is ~5 mmHg less than that in the lungs |
| What generates the lower amount of pressure in the intrapleural spaces? | Generated partly by lymphatic drainage of pleural fluid and partly by structure of the chest |
| How much of a pressure change is required to move air in and out of lungs? | ~1 mmHg |
| What is the max expiratory effort? | ~100 mmHg |
| What is the max inspiratory effort? | ~ -80 mmHg |
| How does quiet breathing work? | Occurs via movements of the diaphragm - Inhalation: diaphragm moves down - Exhalation: resting occurs via passive recoil |
| What happens during heavy breathing? | Intercostal muscles raise and lower the rib cage During forced exhalation, there is an additional contraction of the abdominal muscles |
| What are phospholipid surfactants? | They are found in the fluid lining the alveoli Reduce surface tension and aid in breathing Secreted by Type 2 alveolar cells Lowers surface tension by >10x |
| How much pressure does it take to inflate lungs without surfactant? | ~ - 25 mmHg |
| What is Respiratory Distress Syndrome? (RDS) | Often found in premies as a result of undeveloped surfactant secretion which normally begins at ~32 weeks First breaths are strong: ~ -60 mmHg Treatment includes surfactants and cortisol to speed maturation |
| What is Boyle's Law? | Pressure of a given quantity of gas is inversely proportional to its volume |
| What determines respiration rates under normal circumstances? | CO2 or H+ concentrations |
| Where are gas concentration receptors located? | Arterial system and medulla of the brain |
| Respiration is adjusted to maintain PCO2 levels at what pressure? | 40 mmHg |
| What is hypocapnia? | State of reduced carbon dioxide in the blood Caused by hyperventilation Leads to cerebral vasoconstriction, reduced perfusion, dizziness, ischemia (inadequate blood supply to a part of the body), and acidotic condition in the brain Reduced by breathing into a paper bag |
| What is tidal volume? | The amount of air breathed in and out during normal respiration |
| Inspiratory reserve volume | Amount of air that can be forcefully taken in above normal inspiration |
| Expiratory reserve volume | Amount of air that can be forcefully expelled from the lungs following a normal expiration |
| Residual volume | Air that remains in the lungs that can't be forced out |
| Total lung capacity | Sum of tidal volume, inspiratory reserve volume, expiratory reserve volume, and residual volume |
| Vital capacity | Amount of air that can be expelled following a maximal inspiration |
| Functional residual capacity | Amount of air remaining in lungs after normal expiration |
| Inspiratory capacity | Amount of air that can be inspired following normal expiration |
| How much O2 do we use and CO2 do we produce per minute? | ~200 mL |
| Where do local decreases in O2 or pH cause local vasoconstriction? Wha? What is the significance of this? | In the alveoli ONLY This means that blood only passes through well-ventilated alveoli |
| How much more soluble is CO2 that O2 in water? | 20x |
| How is O2 transported? | It diffuses from the alveoli into the capillaries, then dissolves in plasma and then into RBCs where it combines with hemoglobin. |
| What is our respiratory pigment? | Hemoglobin |
| How much does hemoglobin increase the O2 carrying capacity of our blood? | 60-70x |
| Which is a brighter red: oxy- or deoxy-hemoglobin? | Oxyhemoglobin |
| What effect does packaging hemoglobin inside RBCs have on osmotic pressure? | It keeps the OP low |
| How is the Antarctic Icefish able to survive without respiratory pigment? | O2 is more soluble in cold, so they live in cold water and have a low metabolic rate |
| Describe vertebrate hemoglobin | Has 4 polypeptide globin subunits (beta 1&2 and alpha 1&2), each with a heme group Each heme group has Fe++ which binds 1 O2 loosely. Four molecules of O2 can be transported for every 1 heme group. |
| Difference between HbA, HbF, and HbS | HbA (adult hemoglobin) has mostly 2 alpha and 2 beta subunits HbF (fetal) has mostly 2 alpha and 2 gamma subunits. The gammas switch to betas at birth HbS (sickle cell anemia) has 2 alpha and 2 sickles |
| What is sickle cell anemia? | A disease that causes individuals to have 2 sickle hemoglobin chains instead of 2 betas (the sickle chain has 1 AA different than beta) Causes hemoglobin to polymerize and crystallize, which causes RBC rigidity and capillary obstruction ESPECIALLY in low O2 environments |
| How much higher is hemoglobin's affinity for CO than for O2? | 200x |
| What are the three means of CO2 transport in the blood? | 7% in solution as: CO2 + H20<->H2C03 <->H+ + HCO3- 70% is transported inside RBCs as: CO2 + H20 <->H2C03 <-> H+ + HCO3- <-> H+:Hb 15-25% as: CO2 + Hb -> Carbaminohemoglobin |
| What is carbonic anhydrase? | Speeds up the CO2 transportation reaction inside RBCs by 5000x |
| Where does CO2 attach to hemoglobin? | An amino acid NOT the site where O2 binds |
| What is the O2 pressure at sea level? | 160 mmHg |
| What is the pressure of O2 in the alveoli? Why? | 105 mmHg Because air in the alveoli is subjected to removal of O2 as soon as it enters |
| Is the O2 partial pressure higher in tissures during rest or during exercise? | Rest (40 vs. <20) |
| What is the Bohr effect? | In acidic conditions, hemoglobin has a lower affinity for O2 This lets Hb load more O2 in the lungs where pH is higher and unload more in the tissues where pH is lower |
| What is normal arterial pH? | 7.40 |
| What is the pH of blood during rest after it passes through the capillaries? | 7.36 |
| What is the pH in muscle with exercise? | Down to 6.9 Increases O2 unloading |
| How much does the temperature of active muscles change? | Can increase by 3-4 degrees Causes unloading of O2 |
| What is subunit cooperativity? | As each hemoglobin subunit binds O2, it increases the affinity of other subunits for O2 |
| What is the T (taut) state? | It is the state in which a hemoglobin subunit is not bound to O2 In "low-affinity" state |
| What is the R (relaxed) state? | It is the state after the 1st subunit of hemoglobin binds O2 in which the other three subunits have a higher affinity for O2 SUBUNIT COOPERATIVITY |
| How does O2 binding/unloading in hemoglobin affect CO2 affinity? | As Hb binds O2, its affinity for CO2 decreases and as it unloads O2 its affinity increases |
| What is the Haldane Effect? | Causes hemoglobin to load 2X more CO2 than oxygen in the tissues and unload the same amount more in the lungs |
| What is 2, 3 BPG? | Biphosphoglycerate Byproduct of glycolysis that has a high affinity for the T form of hemoglobin and decreases its affinity for O2 It is higher in tissues where it enhances O2 unloading |
| What can cause a lowered affinity for O2 in hemoglobin? | 2, 3 BPG binds to T form and decreases its affinity for O2 Binding of H+ and CO2 to hemoglobin in tissues shifts hemoglobin to T form, lowering its affinity for O2 |
| Why do smokers not load as much O2? | They have more 2,3 BPG in their blood |
| What happens to 2,3 BPG levels during pregnancy? What does this cause? | 30% increase Lowers the mom's affinity for O2 so more can be offloaded to the fetus. HbF (fetal) doesn't bind much BPG, so it has a higher affinity for O2 to extract it from the mom. |
| What happens to the hemoglobin/O2 saturation graph in sickle-cell anemia? | The curve is shifted right |
| What is the inspiratory region? | Region in the brainstem that generates basic rhythm for breathing by sending signals to the diaphragm |
| What is the expiratory region? | Region of the brainstem that stimulates expiratory muscles during heavy breathing Not activated during quiet breathing |
| What is the pneumotaxic center? | A region of the brainstem whose activity increases ventilation rate |
| What is the apneustic center? | Region of the brainstem that creates long breaths when activated |
| What is the Hering-Breuer Reflex? | When inhalation >1.5 L, stretch receptors begin firing to protect against overinflation |
| What is the goal of respiration? | Maintain proper concentrations of O2, CO2, and H+ |
| How does the body maintain proper concentrations of O2, CO2, and H+? | Blood is monitored by central and peripheral chemoreceptors to detect changes in gases. The receptors automatically adjust ventilation to keep blood gases within set limits. |
| Which chemoreceptors respond most to CO2 and H+? | Central chemoreceptors in the brainstem Increased levels lead to increased ventilation by action of CCs in other respiratory regions Decrease O2 levels have no effect in the brain on respiration |
| What chemoreceptors respond the most to low levels of O2? | Peripheral chemoreceptors in the carotid and aorta Only way low O2 affects respiration The act by causing the respiratory centers to increase breathing rate |
| What is the normal ventilation rate? | 12-14 breaths/min |
| When PO2 decreases by 1/2, how much does ventilation increase? | 1.5x |
| How does the ventilation rate change with a drop in pH from 7.4 to 7.0? | Leads to a 4x increase in ventilation |
| What is the effect on ventilation of increasing the pressure of CO2 by 50% | It leads to a 10x increase in ventilation |
| What is the "Braking Effect"? | The reason low O2 pressure has small effects Occurs because increased ventilation "blows off" too much CO2, causing decreased H+ Low CO2 and H+ causes dramatic inhibition of ventilation via effects on control centers, therefore the O2 pressure usually has little control over ventilation |
| Why does low CO2 and H+ cause dramatic inhibition of ventilation? | Because their regulation is important for acid-base balance |
| At most O2 pressures, is hemoglobin saturated or unsaturated with O2 | Saturated |
| What provides the strongest stimulus to breathe? | CO2 levels |
| What is the functional unit of the kidney? | Nephron |
| How many nephrons are there per kidney? | 1 million |
| What are the two types of nephrons? | Cortical: not so important for water reabsorption (5x more) Juxtamedullary: important for water reabsorption |
| How thick are the walls of the nephron? | 1 cell thick |
| What is the glomerulus? | Capillary bed inside of Bowman's Capsule Supplied by the afferent arteriole and drained by the efferent arteriole which allows control of blood pressure on either side of the glomerulus (because of arteriole sphincters) |
| What is the vasa recta? | Comes from the efferent arteriole Capillary system that surrounds each juxtamedullary nephron Important for reabsorption and secretion |
| What is the osmotic gradient from the cortex to the medulla? | 300 mOsm (cortex) to 1200 mOsm (medulla) |
| What determines how concentrated urine can be? | Length of the Loop of Henle and the size of the osmotic gradient |
| What can urine osmolarity be in some desert animals? | 3000+ mOsm |
| What are the three steps of urine formation? | Filtration, reabsorption, and secretion |
| What detects dehydration? | Hypothalamus Secretes ADH which causes the kidney to conserve |
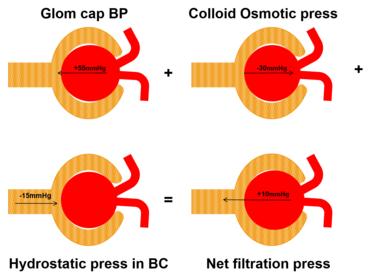
| What drives glomerular filtration? | 10 mmHg net pressure in the glomerulus |
| What gets filtered into Bowman's Capsule? | Anything less than 5,000 MW is freely filtered into the BC Based ONLY on molecule size |
| What are the pressures like around Bowman's Capsule? (picture) | |
| What does fenestrated mean? | To have holes Glomerular capillaries are fenestrated Causes glomerular capillaries to be 100x more permeable than most other capillaries |
| What are podocytes? | "foot cells" What make up the inner layer of Bowman's Capsule and cover the glomeruli |
| What are filtration slits? | Slit between pedicels of the podocytes which dictate what size molecules can be filtered (prevent anything too big from getting through) |
| What percentage of water and solutes passing through the glomerulus is filtered? | 15-25% |
| How many milliliters of water/solutes pass through the glomerulus per minute? | 125 mL/min (=45 gals/day of water) |
| What things are too large to be filtered through the glomerulus? | RBCs and most proteins |
| How much of water/salts is reabsorbed before the kidney produces final urine? | 99% Reabsorption is selective so that some wastes (like urea) become concentrated |
| How does reabsorption occur? | By transport and diffusion Ions are transported and water follows |
| What compounds are 100% reabsorbed in the kidney? | Glucose, vitamins, and amino acids |
| How are 2/3 of filtered Na+ reabsorbed? | Through active transport |
| What is the driving force for most that happens in the proximal convoluted tubule? | R |
| How are filtered proteins reabsorbed? | By endocytosis |
| How much of total filtrate is reabsorbed on the PCT? | 2/3s If he says "most reabsorbed".....assume PCT! |
| Drugs, toxins, and H+ can be secreted in the PCT. How? | The liver tags drugs/toxins with glucuronate or sulfate groups. The kidney recognizes and secretes these. |
| What are the functions of the Descending Loop of Henle? | Passive H2O reabsorption NO active transport of salts |
| What are the permeabilities in the Descending Loop of Henle? | Salt is moderately permeable Urea has low permeability High H2O permeability (H2O is pulled out by high osmolarity in the medulla via Aq1 aquaporins) |
| What controls Aq2? | ADH |
| What are the functions of the Ascending Loop of Henle? | Passive salt reabsorption in the thin part and active reabsorption in the thick |
| What are the permeabilities in the Ascending Loop of Henle? | High salt permeability (pulled out by decreasing osmolarity of the ECF as pre-urine moves toward the cortex) Low urea Low water |
| What is the Diluting Segment? | The thick part of the Ascending Loop of Henle Called that because the filtrate become hyposomotic as salt is actively transported out |
| What is the osmolarity of pre-urine at the end of the Diluting Segment? | 100 mOsm (1/3 of blood) |
| What do the actions of the Distal Convoluted Tubule and the Cortical Collecting Duct depend on? | Hormones and acid-base balance |
| Where does aldosterone stimulate Na+ reabsorption and K+ secretion? | Distal Convoluted Tubule and the Cortical Collecting Duct Way that the potassium concentration in the urine is controlled |
| When are the DCT and CCT permeable? | Only when ADH is present |
| What can be secreted into urine and reabsorbed from pre-urine? | Secreted into: K+, H+, and NH3 Reabsorbed from: Na+, Cl-, and HCO3- |
| What happens if pre-urine is too acidic?Too basic? | Acidic: H+ can be secreted (against up to a 1000x gradient) Basic: HCO3- can be secreted |
| What is the function of the medullary CD? | Mainly in variable H2O reabsorption (depends on state of hydration and concentration of ADH) |
| What happens when ADH is present? | The Medullary CD becomes permeable to H2O and the pre-urine equilibrates with the high osmolarity of medulla ADH stimulates the insertion of aquaporins (Aq2) into the membrane Also stimulates facilitated transport of urea out of pre-urine into the medullary ECF |
| How does ETOH dehydrate? | Reduces the release of ADH |
| When does the gradient reach 1200 mOsm? | Only when ADH is high Urine will be between 100 and 1200 mOsm depending on the concentration of ADH |
| What are the two mechanisms that produce the up to 900 mOsm gradient/ | Active transport of salts in the diluting segment creates 600 mOsm of gradient Facilitated transport of urea out of the medullary CD creates 300 mOsm |
| How does facilitated transport of urea out of the medullary CD create part of the gradient? | Urea becomes concentrated by ~65x as pre-urine flows through the nephron In the Medullary CD it is transported down its concentration gradient into extracellular fluid when ADH is high |
| How is the glomerular filtration rate controlled? | Through both ANS and local control ANS: strong sympathetic activity via fight/flight, exercise, or bleeding causes vasoconstriction of the afferent arteriole. This shunts blood away from the kidney, leading to decreased filtration to maintain blood volume Local: also called autoregulation; maintains filtration fairly constant over BPs from 75 mmHg to 160 mmHg because if filtrate flows through nephron fast then too little is reabsorbed (and vice versa) |
| What is myogenic autoregulation? | When high blood pressure stretches the afferent arteriole, causing a reflex smooth muscle contraction that leads to a decreased glomerular filtration rate Decreased blood pressure causes dilation of the afferent arteriole and constriction of the efferent, increasing GFR |
| What is the Juxtaglomerular Apparatus? | When activated the JGA causes increased glomerular filtration rate Area located in the angle between the afferent and efferent arterioles in the region of the DCT just after the diluting segment Formed from aff/eff arterioles + the adjoining DCT |
| What is the macula densa? | DCT cells that touch arterioles and sense [Na+] When [Na+] is low, it causes the macula densa to release NO which dilates the afferent arteriole and PGs which cause granular cells to secrete renin. |
| Why does low [Na+] cause the macula densa to release NO to dilate the afferent arteriole? | low Na+ can be caused by over-absorption in the diluting segment due to low flow, so dilating the aff. arteriole increases that flow |
| What are the granular cells? | Cells between the macula densa and the afferent arteriole which secrete renin both in response to PGs from the macula densa and in response to BP or sympathetic NS stimulation |
| What is RAAS? | renin angiotensin aldosterone system |
| What is renin? | It is an enzyme produced by granular cells that converts angiotensinogen from the liver to angiotensin I |
| How do you make Angiotensin II? | A converting enzyme in the lungs converts Angio I to Angio II |
| What does angiotensin II do? | Causes systemic vasoconstriction (greater effect on efferent arteriole than aff. to maintain SOME kidney filtration) Stimulates sympathetic NS activity Stimulates ADH secretion Stimulates thirst Causes the adrenal cortex to release aldosterone, which increases Na+, H2O, and Cl- reabsorption and K+ secretion. |
| How do ACE inhibitors work? | The block the angiotensin converting enzyme in the lungs |
| What are the three natriuretic peptides? Where are they produced? | Atrial natriuretic peptide (ANP): hormone produced by the atria B-type natriuretic peptide (BNP): hormone produced by the ventricles C-type natriuretic peptide (CNP): paracrine compound produced in the endothelium and the heart |
| What do natriuretic peptides do? When are they released? | Released when high blood volume stretches the tissues that produce them Act opposite to RAAS: inhibit sympathetic system and secretion of renin, aldosterone, and ADH Cause vasodilation and loss of Na+ and water Causes lipolysis which reduces the fat load on the heart |
| Why are BNP levels used to assess heart failure? | The heart output during heart failure can't match the venous return, so the ventricles get stretched. When they are stretched, they release BNP. |
| What are diuretics? | Most inhibit reabsorption of Na+ and Cl- so you lose both NaCl and H2O Used to treat heart failure, high blood pressure, and kidney disease |
| What are the #1 and #2 causers of nephropathy? (kidney disease) | 1. Diabetes 2. High blood pressure |
| What does nephropathy cause? | Albuminuria (loss of albumin) and hyperfiltration |
| What causes nephropathy? | High glucose and high blood pressure lead to the loss of podocytes |
| How long is the tube of the digestive tract? | 17-20 feet |
| What is the primary method of chemical digestion? | Hydrolysis Molecules are split by adding water |
| What does saliva contain? | Amylase: breaks down starch Lipase: breaks down fat Lysozyme: enzyme that lyses gram+ bacteria |
| How does the autonomic nervous system affect saliva release? | Parasympathetic stimulates Sympathetic inhibits |
| What is chyme? | Mix of food and gastric secretions from the stomach |
| What produces gastric secretions? | Cells of the gastric pits in the stomach |
| What does the stomach do? | Produces chyme Denatures proteins Disinfects Produces gastric secretions (including acid and mucus) |
| What are mucous neck cells? | Cells in the gastric glands of the stomach that produce a thick mucus/bicarbonate (basic) layer for protection |
| What are chief cells? | Cells in the gastric glands of the stomach that produce pepsinogen Pepsinogen is converted by HCl from the stomach to pepsin, which cuts proteins into small peptides |
| What does pepsinogen do? | Pepsinogen is converted by HCl from the stomach to pepsin, which cuts proteins into small peptides |
| What are parietal cells? | Cells in the gastric glands in the stomach that secrete [HCl] at a pH of about 1 Inhibited by Prilosec, Prevacid, and others |
| How strong is the proton pump of parietal cells? | Can pump against a million times gradient |
| What is the function of [HCl] in the stomach? | Disinfects, is a good solvent, and denatures 3rd degree structures of proteins |
| What are G cells? | Cells of the gastric glands of the stomach which secrete gastrin |
| What is gastrin? | Peptide hormone released by the G cells in the gastric glands which indirectly stimulate parietal cells to release HCl Excessive amounts are related to ulcers |
| How does gastrin stimulate the release of HCl? | Stimulates the secretion of histamine by the ECLs (enterochromaffin-like cells) of the gastric pits The histamine acts as a paracrine to stimulate the parietals which then release HCl |
| How do Zantac and Pepcid work? | They block histamine receptors to prevent the stimulation of parietal cells which secrete acid in the stomach |
| What effect does the parasympathetic have on parietal cells and ECLs? | Stimulates both! "Rest/DIGEST" |
| What can the stomach absorb? | Some small molecules ETOH, H2O, glucose, especially non-polars |
| How often is the lining of the stomach replaced? | Every 3 days |
| What is the intrinsic factor? | A polypeptide that is produced by parietals that is necessary for absorption of vitamin B12 in the small intestine |
| What is pernicious anemia? | Anemia that results from a lack of vitamin B12 B12 is necessary for RBC production, so too little results in low hematocrit (anemia) Occurs mostly from autoimmune attack against parietals or intrinsic factor |
| Where does most digestion occur? | Small intestine |
| How long is the small intestine? How big is the absorptive area? | 10 feet long Size of a tennis court |
| Describe the surface of the inside of the small intestine | Highly folded, covered with finger-like villi (looks like carpet), has tight junctions so nutrients have to move across membranes |
| What are microvilli? | Cover the villi of the small intestine Secrete enzymes for complete breakdown of food molecules to monosaccharides and amino acids prior to absorption |
| What part of the small intestine functions in reabsorption of nutrients? Fats? | Capillaries in the villi (nutrients) Lacteals, which are blind-ending lymph capillaries (fats) |
| How long does it take for chyme to move through the small intestine? | Several hours |
| Where is the pancreas? | Below the stomach and connected to the small intestine via the pancreatic duct |
| What enzymes are secreted by the pancreas? | Amylases: convert starches to smaller saccharides Lipase: converts triglycerides into free fatty acids and monoglycerides Proteases: convert proteins into dipeptides Bicarbonate: neutralizes stomach acid ALL PRODUCED AND SECRETED IN INACTIVE FORM |
| Why are pancreatic enzymes produced and secreted in the inactive form? | Because they are so powerful that they can digest the pancreas itself if in active form Normally activated in the small intestine |
| What is acute pancreatitis? | Pancreatic enzymes become active in the pancreas instead of in the small intestine Can cause death in a few days if not stopped |
| What is the pH in the small intestine? | 6.5-7.5 |
| Digested carbohydrates and proteins are absorbed by capillaries in the small intestine villi. Where do they go next? | Directly to the liver via the hepatic portal vein |
| What does the liver do? | Detoxifies blood Processes nutrients |
| What is the first pass effect? How do you avoid it? | Many drugs absorbed by the GI tract are broken down in the liver To avoid this, they have to be injected, absorbed transdermally, or in suppository |
| What are prodrugs? | Drugs that are designed to be absorbed in the GI tract and activated in the liver Example: dextromethorphan (cough suppressant) is activated in the liver to dextrorphan |
| What are bile acids? | Emulsifying, detergent-like molecules produced by the liver that are the first step in fat digestion Secreted by the liver constantly and stored in the gall bladder |
| What happens to the gall bladder after meals? | It contracts, sending bile to the small intestine |
| What does emulsification do? | Increases surface area for lipase to covert fat to fatty acids and monoglycerides Forms micelles |
| What are micelles? | Aggregates of fatty acids and monoglycerides that are coated with bile acids |
| What happens to the fatty acids and monoglycerides produced by lipase? | Absorbed by the small intestine villi and most then used to resynthesize triglycerides in smooth ER of the villi Some of the small fatty acids are absorbed by capillaries in the villi and go to the liver |
| What are chylomicrons? | Made in the small intestine villi Triglycerides and cholesterol are packaged with a phospholipid and lipoprotein coat Chylomicrons are then secreted into the lacteals (lymphatic system) |
| Why is plasma taken after meals often cloudy? | Because of the chylomicrons being released into the lymphatic system |
| How long is the large intestine (colon)? | 4 feet |
| How much water does the large intestine absorb? | 0.5-2L per day |
| What does the large intestine absorb? | Water, vitamins, drugs, suppositories |
| Why is the large intestine slow-moving? | Lets bacteria digest unabsorbed material (mostly cellulose) |
| How many species of bacteria are there in the large intestine? | 400+ |
| How much of the mass of feces is of bacterial origin? | 1/3 |
| What is flatus? | Gas produced by bacteria in the large intestine |
| Why do beans give you gas? | They contain undigestable carbohydrates which bacteria convert to gas |
| What do bacteria in the large intestine produce from fiber? | Vitamin K, vitamin B, and fatty acids |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.