6692302
Description
Flashcards by Esther Kim, updated more than 1 year ago
|
|
Created by Esther Kim
about 8 years ago
|
|
| Question | Answer |
| Features of R ventricle | - most anterior cardiac surface - thin wall - Under lower pressure |
| Features of L ventricle | - Lies behind R ventricle (except for apex) - Powerhouse of the pump |
| Which side of heart sounds louder? | Left heart sounds are more prominent and louder |
| Anatomy: Base of Heart | - Superior aspect of the heart - Rt & Lt 2nd ICS - Defines junction between pulmonic a. & R ventricle - Close to sternum |
| Anatomy: Apex | - Bottom of heart, defines inferior tip - Apex at 5th ICS - 7-9 cm from midsternal line |
| Name the arteries and their respective valves | 1. Pulmonary artery --> Pulmonic Valve 2. Aorta --> Aortic Valve |
| Where are the Atrioventricular Valves? | 1. R Atrium to R Ventricle --> Tricuspid valve 2. L Atrium to L ventricle --> Mitral Valve (Bicuspid) "try before you buy" |
| Circulation: heart to lungs | Flows from R ventricle --> lungs via pulmonary artery |
| Circulation: lungs to heart | Blood returns from lungs--> L atrium through pulmonary veins |
| Circulation: heart to body | Left ventricle to all over body |
| Circulation: body to heart | Blood returns from body to R atrium via vena cava |
| Systole | ventricular contraction |
| Diastole | ventricular relaxation |
| Valves during systole | Aortic & Pulmonic valves --> open Mitral & Tricuspid valves --> close |
| Cardiac Cycle | 1. Pulmonary veins pump blood from lungs to L atrium 2. Passes through mitral valve into L ventricle 3. Pressure in L ventricle > L atrium, mitral valve closes 4. Blood ejected out aorta through aortic valve 5. Mitral valve closure = S1 |
| When does systole begin? | After S1 |
| When/which valves close/open during Systole? | 1. LV pressure > Aortic pressure --> Aortic Valve opens - Blood pumped out of heart into aorta 2. LV pressure < Aortic pressure --> Aortic Valve closes 3. Aortic valve closure = S2 |
| When does diastole begin? | Begins with S2 |
| When and which valve opens during diastole? | Mitral valve opens as pressure rises in L atrium (not normally audible) |
| When/where does contraction occur in diastole? | After period of rapid ventricular filling, atrial contraction occurs (Usually inaudible) |
| S3 | Rapid Ventricular Filling in Diastole |
| S4 | Atrial Contraction in Diastole |
| Which part of cardiac cycle is auscultated? | - CLOSURE of valves responsible for heart sounds - normal heart sounds: S1 and S2 (sometimes s3 and s4 heard) |
| Cardiovascular Exam | 1. Assess Jugular Venous Pressure (JVP) 2. Assess Carotid Pulse 3. Examine Heart - Inspection - Palpation - Auscultation 4. Peripheral Vascular Exam |
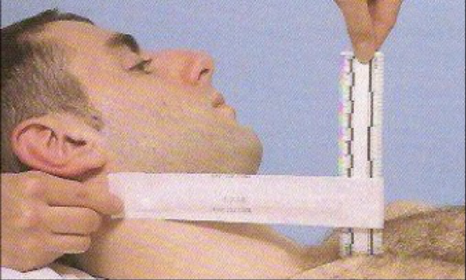
| JVP exam | - pt comfortable & supine - Head raised to 30˚ and tilted away from you - use tangential lighting to identify landmarks ID amplitude and timing of venous pulsations |
| Measure JVP | - ID highest pt of venous pulsation of internal jugular along SCM border - Measure vertical distance above sternal angle |
| JVP look and feel | - Arterial pulsations: look and feel like single strong impulses - Venous pulses: look like billowing sails with gentler wave forms - Compare with apical/radial pulse |
| Normal JVP vs. Significance of Abnormal JVP | Normal JVP: < 4 cm above sternal angle Elevated JVP may indicate volume overload or R heart failure (CHF) |
| Pt position for Carotid Pulse | Supine with head of bed elevated at 30˚ |
| where to inspect for carotid pulse | medial to sternocleidomastoid muscles |
| What to palpate for carotid pulse | - Amplitude - Rate - Contour - Thrills |
| How to auscultate carotid pulse (before palpation) | - Have pt hold breath - Use stethoscope bell to listen for bruit - listen for rumbling sound of turbulent blood flow through artery |
| Pt's position for cardiac exam | - Starting position supine w/head elevated to 30˚ - Other positions include: a. Left Lateral Decubitus (LLD) b. Sitting up, leaning forward |
| Examiner's positioning for cardiac exam | stands on R side of patient |
| What to look for in Cardiac Exam: Inspection | - Heaves - Point of Maximum Intensity (PMI) or Apical Impulse |
| What to feel for in Cardiac Exam: Palpation | - Lifts and heaves, thrills, PMI - Cardiac Silhouette |
| What to listen for in Cardiac Exam: Auscultation | - Heart Sounds - Murmurs |
| Location of Apical Impulse | 4th or 5th intercostal space |
| Normal Diameter of Apical Impulse | Less than 2.5 cm |
| Normal Amplitude of Apical Impulse | Usually small, brisk, tapping |
| How to measure duration of Apical Impulse | Listen, feel, and estimate proportion |
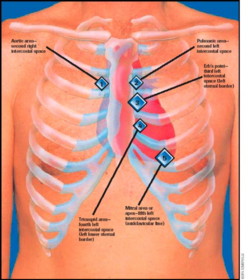
| Designated Areas of Precordium to Auscultate | - Right 2nd ICS - Left 2nd through 5th ICS - Apex |
| Proper Cardiac Auscultation: Bell vs. Diaphragm | Use both diaphragm and bell: - Diaphragm for higher pitched sounds - Bell for lower pitched sounds |
| Proper Cardiac Auscultation for Left Lateral Decubitus Position | - Use bell - Bring LV closer to chest wall Accentuates S3, S4, and mitral stenosis murmur |
| Proper Cardiac Auscultation for Sitting Up, Leaning Forward | - Use Diaphragm - Accentuates aortic murmurs |
| Purpose of Cardiac Auscultation using Squatting, Valsalva maneuvers | Makes different murmurs louder or softer |
| When/Where is S1 and S2 loudest? | - S1: loudest at apex (mitral valve closing) - S2: loudest at base (aortic valve closing) |
| When do you hear systole and diastole? | - Systole: between S1 and S2 - Diastole: between S2 and S1 |
| Which is longer- systole or diastole? | Systole is shorter than diastole |
| When are pulses palpable? | During systole |
| Significance of L heart sounds | S1 = mitral closure S2 = aortic closure |
| Significance of R heart sounds | S1 = tricuspid closure S2 = pulmonic closure |
| Which side of heart contracts later? | Right side contracts slightly later S1 = M1*T1 S2 = A2*P2 |
| Splitting Heart Sounds | - Splitting refers to separation of heart sounds into 2 components - Though both S1 and S2 an be split, splitting of S2 is more clinically important |
| When are physiologic splitting heart sounds accentuated? When do they disappear? | - Separation of S1 or S2 into separate sounds accentuated by inspiration - Disappears with expiration |
| What causes Extra Heart Sounds in Systole | - Ejection sounds are pathologic, caused by opening of valves that should be closed - occurs early in systole, immediately after S1 |
| Which valves are affected with extra heart sounds in systole | Aortic or pulmonic valves |
| Auscultating Extra heart sounds in systole | - High pitched - Sharp, clicking quality - Heard best with diaphragm |
| Systolic Clicks | - Heard mid-to-late systole - most common in Mitral Valve Prolapse - High-pitched |
| Extra heart sounds in Diastole: Opening Snap | - Heard early in diastole - Usually caused by opening of stenotic MV - Loud, high-pitched snapping sound |
| Extra heart sounds in Diastole: S3 (Ventricular Gallop) | - Physiological OR pathological - Heard early in diastole during rapid ventricular filling - Can be physiologic in children but usually pathologic in patients >40 yo |
| Extra Heart Sounds in Diastole: S4 | - Atrial Gallop - Heard late in diastole, just before S1 - Dull, low-pitched sound - Heard best with Bell - Can be physiologic, but more often pathologic |
| Heart Murmurs | - Longer duration than heart sounds - Often caused by turbulent blood flow through a valve - can indicate disease or be benign - heard best over respective auscultatory areas for the involved valve |
| Innocent Mumurs | - Turbulent blood flow across valve due to strong ventricular ejection of blood - common in children & young adults - no evidence of cardiovascular disease - no physiological/structural abnormalities |
| Pathologic Murmurs | - arise from structural abnormalities in valves - stenosis --> hardening/narrowing of valve --> impedes valve blood flow - Regurgitation --> failure of valve to close completely --> allows blood backflow |
| Important Traits to Note in Heart Murmurs | - Location - Intensity - Timing - Pitch - Quality - Radiation |
| Heart Murmurs: Grading (1-6) | - Grade 1: very faint - Grade 2: quiet, but heard immediately - Grade 3: moderately loud - Grade 4: loud - Grade 5: very loud, heard with stethoscope partially off of chest - Grade 6: heard with stethoscope completely off of chest |
| Systolic Mumurs | May be innocent OR pathologic - Early Systole - Midsystolic - Late systolic - Holocystolic |
| Diastolic Murmurs | ALWAYS pathologic - early diastolic - mid-diastolic - late diastolic |
| Qualities of Heart Murmurs | - Harsh (stenosis) - Blowing (regurgitation) - Rumbling - Musical |
| Characteristics of Heart Murmur Contours | Pattern of sound intensity over time - crescendo: gets louder - descrescendo: gets softer - crescendo-decrescendo - plateau: intensity constant |
| Adventitious Heart Sounds | Mixed cycle: not confined to one aspect of cardiac cycle |
| Pericardial friction rub | Type of mixed cycle - inflammation of pericardial sac |
| Patent Ductus Arteriosus | Type of adventitious heart sounds mixed cycle - congenital opening between aorta and pulmonary arteries |
| Venous Hum (continuous) | - Type of mixed cycle - Adventitious heart sounds - benign turbulent blood flow in jugular veins |
| Documenting CV Exam: precordium | Precordium is quiet without lifts - No carotid pulations or JVD noted |
| Documenting CV exam: JVP | JVP measured at 3cm above sternal angle with HOB elevated to 30 degrees |
| Documenting CV exam: carotid pulses | 2+ and equal without thrills or bruits - upstrokes are brisk |
| Documenting CV exam: PMI | -tapping, 7 cm lateral to MSL in 5th ICS - No lifts or thrills of precordium or apical impulse |
| Documenting CV exam: S1, S2 | - Crisp S1, S2: louder at base - S1 louder at apex - physiologically split S2 |
| Documenting CV exam: S3, S4 | - No S3, S4 gallops - No murmurs or rubs |
| CV exam checklist | - Inspect precordium with pt supine at 30 - Inspect carotid arteries & jugular veins for pulsations/distention - Measure JVP - Auscultate carotid arteries before palpating for thrills - Palpate precordium for lifts and thrills; palpate apical impulse - Palpate for PMI in LLD - Auscultate with diaphragm in aortic, pulmonic, tricuspid, mitral areas Auscultate with bell in A/P/T/M areas Auscultate with bell in LLD Auscultate with diaphragm sitting up, leaing forward |
| Points of Cardiac Auscultation: 1. Aortic (R 2nd ICS) 2. Pulmonary (L 2nd ICS) 3. Tricuspid (L 4th ICS) 4. Mitral/Apex (L 5th ICS) |
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.