8826925
Description

Flowchart by Molly Frost, updated more than 1 year ago
|
|
Created by Molly Frost
over 8 years ago
|
|
Flowchart nodes
- Antepartum Haemorrhage
- "APH is defined as bleeding from or in the genital tract, occurring from 24+0 weeks of pregnancy and prior to the birth of the baby" (RCOG, 2011)
- Most common causes:- Abruption- Placenta Praevia- Uterine Rupture- Vasa Praevia
- 3-5% of pregnancies affected by APH
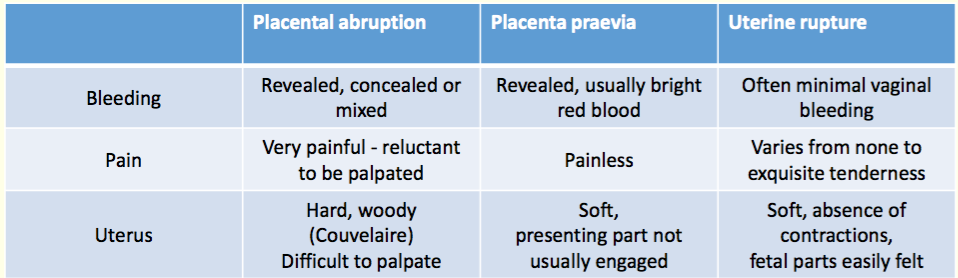
- Abruption
- Placenta Praevia
- Uterine Rupture
- "Complete or partial separation of a normally situated placenta after 24th week of pregnancy and prior to delivery"
- Recognition- Sudden severe abdominal pain and hypovolaemic shock- Board-like uterus + excess pain - Fetal parts difficult to palpate
- - Placental separation triggered by bleeding into decidua basalis- Blood seen doesn't represent severity s abruption may be concealed- Bleeding may be revealed, concealed or mixed - May be history of reduced or excessive FMs - Where <1000ml blood lost = hypoxic foetus - Where >1500ml women is in shock and foetus dead
- Risk Factors - Previous abruption (4.4% incidence of recurrent abruption. Recurs in 19-25% of women who've had two previous pregnancies complicated by abruption) - Pre-eclampsia: High blood pressure means high force blood flow - Fetal Growth Restriction: Poor placental function- Polyhydramnios: sudden decrease in pressure, causing abruption - Advanced maternal age: likely to have other risk factors due to this
- Incidence 2 maternal deaths from placental abruption from 2009-2012 in UK & Ireland (MBRRACE, 2014)
- "Placenta praevia exists when the placenta is inserted wholly or in part into lower segment of uterus"
- Major: Placenta lies over internal cervical osMinor/ Partial: Leading edge of placenta is in lower uterine segment but not covering cervical os
- Recognition - Bleeding PAINLESS, FRESH RED AND RECURRENT- SOFT uterus and NON-TENDER- PRESENTING PART high not central
- TRANS-VAGINAL USS is safe + more accurate than trans-abdominal
- Clinical suspicion raised:- Vaginal bleeding >20wks- High presenting part- Abnormal lie- Painless provoked bleeding- Irrespective of previous USS, a more low lying placenta at present(RCOG, 2011)
- Incidence 1 maternal death from placental praevia from 2009-2012 in UK & Ireland (MBRRACE, 2014)
- Risk factors:- Prev placenta praevia- Prev C-sections: the more = higher risk - Prev termination of pregnancy: scar tissue- Multiparty: placenta sites over os due to lack of space- Advanced maternal age: likely to have other risk factors from this
- Uterine dehiscence: disruption of uterine muscle with intact serosa (outer layer of uterus or perimetric)
- Uterine Rupture: disruption of uterine muscle extending to and involving the uterine serosa or disruption of uterine muscle with extension to bladder or broad ligament (RCOG, 2007)
- Incidence 4 maternal deaths from uterine rupture from 2009-2012 in UK & Ireland (MBRRACE, 2014)
- Recognition- Symptoms vary from NONE to severe abdominal pain- Hypovolaemic shock- Fetal parts easy to palpate- Fetal HR - compromise - Subrapubic pain present between contractions and often felt despite analgesia- Exquisite tenderness on palpation of lower segment- Rising maternal pulse - Intrapartum vaginal bleeding- Sudden cessation of contractions- Palpations detects malpresention/ fetal parts easily palpable- Fetal presenting part moves up on VE- Maternal shock and collapse- Haematuria
- Risk Factors - Previous CS- 2 X risk if induced - prostaglandins + oxytocin causes hyper stimulation + weaken previous scars making them susceptible to rupture
{kind=link}
- Delivery- If woman still pregnant, birth of baby must be planned - Time: essential to stabilise woman, time of day, steroids for baby- Team: Senior staff essential- Place: Appropriate facilities e.g. theatre NICU- Route: C/S or vaginally
- - Increased maternal age- Increased risk if over >42 weeks- Increased risk if fetus >4000g- Cases documented in primips with no risk factors
- - Multiple pregnancy: sites over os due to lack of space- Smoking: larger placenta to compensate for poor blood flow- Assisted conception- Deficient endometrium due to uterine scar, fibroid, manual removal of placenta
- - Multiparty: 2nd twin issue of placenta coming away too soon- Low BMI: poor nutritional state therefore poor placenta function- Assisted reproductive technique pregnancy- Intrauterine infection: impair placental function - PROM: increase chance of infection- Abdominal trauma: DV or RTC - Smoking + drug misuse: vasoconstriction to placental blood flow causing hypoperfusion and ischemia( RCOG, 2011)
- MOANS teamM - mother, senior midwife, 2nd midwifeO - Obstetrician, Reg, SHOA - Anaesthetist, ODPN - NICU, Haematologist, HCA, MSW, PorterS - Scribe
- Mother - inform her of what's happening, and depending on severity then the chance of going to theatre
- Senior Cons/ Reg - Prepare women for delivery/ theatre with Ranitidine 50mg, Metoclopramide 10mg or Sodium Citrate 30mls Gain consent implied/ verbal for theatre
- Senior Midwife - put out 2222 crash call, give advice from senior knowledge, delegate roles
- 2nd Midwife - Catheterise with hourly bag, and cannulate, taking bloods = FBC, Clotting, G&S, X match, Blood cultures
- SHO - Cannulate other hand and put up IV fluids - Colloids 500ml+ Crystalloid 1L x2
- Anaesthetist - Manage Airway: Facial O2Breathing: Resps, O2 sats Circulation: HR, Cap refillDisabilityExposureHypovolaemic shockODP - Alert theatre, gown for mother
- Neonatal Team/ NICU: Inform NICU unexpected admission, senior neonatal team for NLS as baby will be compromised Cord bloods/ gases required
- Scribe: Document obs on Meows + fluid balance, drug charts HDU chart. Documents roles, drugs, times, routes, amounts Transcribed by midwife after adding rationale and storing notes with mother and baby's notes for 25 years in line with NMC Code (2015)
- LTC - Mother- Anaemia - Infection- Maternal Shock- Renal Tubular Necrosis- Consumptive Coagulopathy- PPHProlonged hospital stay- Psychological stress- Complications of blood transfusions (RCOG, 2011)
- LTC - Baby- Fetal hypoxia - SGA + IUGR- PREM- Fetal death(RCOG, 2011)
- TIME CRITICAL EMERGENCY
Want to create your own Flowcharts for free with GoConqr? Learn more.