5764651
Description
Quiz by Rachel Nall, updated more than 1 year ago
|
|
Created by Rachel Nall
almost 8 years ago
|
|
Question 1
Question
[blank_start]Cardiac output[blank_end] is the quantity of blood pumped each minute into the aorta by the heart.
Answer
-
Cardiac output
-
Venous return
-
Cardiac index
-
Peripheral resistance
Question 2
Question
[blank_start]Venous return[blank_end] is the quantity of blood flowing from the veins into the right atrium (RA) each minute.
Answer
-
Venous return
-
Cardiac output
-
Cardiac index
-
Stroke volume
Question 3
Question
VR and CO must [blank_start]equal[blank_end] each other except for a few heartbeats at a time when blood is temporarily stored in or removed from the heart and lungs.
Answer
-
be less than
-
be greater than
-
equal
-
add to
Question 4
Question
Which of the following factors does NOT affect cardiac output?
Answer
-
Basal metabolic rate
-
Gender
-
Age
-
Body habitus
-
Increased energy requirements (exercise)
Question 5
Question
Cardiac Index = [blank_start]CO[blank_end] / [blank_start]m2[blank_end]
m2 = [blank_start]Body Surface Area[blank_end]
Answer
-
CO
-
Stroke volume
-
m2
-
Venous return
-
Body Surface Area
Question 6
Question
The average CO for a resting adult is [blank_start]5[blank_end] liters/minute
The average CI for a resting adult is [blank_start]3[blank_end] liters/minute/m2
Answer
-
5
-
3
Question 7
Question
At what age is a person's cardiac function the highest?
Answer
-
10
-
20
-
30
-
40
Question 8
Question
Peripheral circulatory factors that affect the flow of blood from the veins into the heart provide the primary control of CO.
Answer
- True
- False
Question 9
Question
Blood flow does not increase in proportion to each tissue's metabolism.
Answer
- True
- False
Question 10
Question
If arterial BP is constant, long-term CO will typically have an [blank_start]inverse[blank_end] relationship to total peripheral resistance.
This is a form of [blank_start]Ohm's[blank_end] law.
Answer
-
inverse
-
proportional
-
Ohm's
-
Reynold's
-
Frank-Starling
Question 11
Question
The Frank-Starling law states that the [blank_start]stroke volume[blank_end] of the heart increases in response to an an increase in the volume of blood filling the heart (end diastolic volume), when all other factors remain constant.
Another way to state this: a large volume of blood flows into the ventricle, the blood will stretch the walls of the heart, causing a greater expansion during diastole, which in turn increases the force of the contraction and thus the quantity of blood that is pumped into the aorta during diastole. The increased volume of blood stretches the ventricular wall, causing cardiac muscle to contract more forcefully.
Answer
-
cardiac output
-
cardiac index
-
stroke volume
Question 12
Question
According to the Frank-Starling curve, the normal heart can pump an amount of venous return up to what times the normal venous return before the heart becomes a limiting factor in the control of cardiac output?
Answer
-
2
-
2.5
-
3
-
3.5
Question 13
Question
Sympathetic stimulation and parasympathetic inhibition can significantly increase heart rate and contractility. The result of this combination is known as what kind of heart?
Answer
-
Effective
-
Hypoeffective
-
Hypereffective
-
Optimized
Question 14
Question
A number of factors can lead to a hypoeffective heart. Examples include increased arterial pressure (afterload), due to hypertension, valvular heart disease, and congenital heart disease. Select other causes of the hypoeffective heart.
Answer
-
Sympathetic nervous system inhibition
-
Sympathetic nervous system excitation
-
Pathological dysrhythmias
-
Acute coronary syndrome
Question 15
Question
The nervous system is instrumental in maintaining arterial blood pressure when peripheral blood vessels are [blank_start]dilated[blank_end] and venous return and CO [blank_start]increase[blank_end].
Answer
-
dilated
-
constricted
-
increase
-
decrease
-
stay the same
Question 16
Question
Fill in the blanks for the following:
Intense exercise [blank_start]increases[blank_end] SNS outflow, causing large vein [blank_start]constriction[blank_end], and [blank_start]increase[blank_end] in heart rate and an [blank_start]increase[blank_end] in contractility.
Answer
-
increases
-
decreases
-
constriction
-
dilation
-
increase
-
decrease
-
increase
-
decrease
Question 17
Question
Beriberi disease leads to a manifestation of insufficient dietary vitamin B1 (thiamine). The results of auto-regulatory compensation [blank_start]increases[blank_end] cardiac output.
Answer
-
increases
-
decreases
-
maintains
Question 18
Question
Select the other pathologic states that increase cardiac output:
Answer
-
Arteriovenous (AV) fistula
-
Hypothyroidism
-
Hyperthyroidism
-
Anemia
Question 19
Question
Conditions that produce low CO generally fall into one of two categories:
1. Abnormalities that [blank_start]reduce[blank_end] the pumping effectiveness of the heart.
2. Abnormalities that cause venous return to [blank_start]fall too low[blank_end].
Answer
-
reduce
-
increase
-
fall too low
-
become too high
Question 20
Question
[blank_start]Hemorrhage[blank_end] is the most common non-cardiac peripheral factor that decreases venous return.
Answer
-
Hemorrhage
Question 21
Question
Non-cardiac factors that decrease cardiac output due to decreased venous return include:
Answer
-
Obstruction of the large veins
-
Decreased tissue mass
-
Arteriovenous Fistula
-
Hypothyroidism
Question 22
Question
The two primary factors that must be evaluated in the quantitative analysis of CO regulation are:
Answer
-
The pumping ability of the heart (cardiac output)
-
The heart's end-diastolic volume (preload)
-
Venous return curves
-
The pressure on the wall of the left ventricle during ejection (afterload)
Question 23
Question
The normal external pressure on the heart is equal to the normal [blank_start]intrapleural[blank_end] pressure (which is -4 mmHg).
Answer
-
intrapleural
Question 24
Question
A shift to the [blank_start]right[blank_end] reflects the increase RA pressure that will be required to fill the cardiac chambers to offset the [blank_start]increase[blank_end] in external pressure.
Answer
-
right
-
left
-
increase
-
decrease
Question 25
Question
Select the following factors that can shift the CO curve:
Answer
-
Cyclical changes in intrapleural pressure during respiration
-
Breathing against a negative pressure
-
Positive pressure breathing
-
Opening the thoracic cage
-
Cardiac tamponade
Question 26
Question
Principle factors that affect VR to the heart from the systemic circulation:
◦ 1. [blank_start]RA pressure[blank_end]
Exerts a backward force on the veins to impede
flow of blood from the veins into the RA
◦ 2. The degree of filling of the [blank_start]systemiccirculation[blank_end]
Measured by the mean systemic filling pressure (Psf) which forces the systemic blood toward the heart.
Answer
-
RA pressure
-
systemic circulation
Question 27
Question
[blank_start]Psf[blank_end] is the abbreviation for mean systemic filling pressure.
Answer
-
Psf
Question 28
Question
The principle factor that affects Venous Return to the heart from the systemic circulation is resistance to blood flow between the peripheral vessels and the RA.
Answer
- True
- False
Question 29
Question
The normal venous return curve demonstrates that if the pumping ability of the heart decreases, the RA pressure will [blank_start]rise[blank_end], and the backward force of this rising pressure on the systemic vasculature will [blank_start]decrease[blank_end] VR.
Answer
-
rise
-
fall
-
stay the same
-
decrease
-
increase
Question 30
Question
Without compensatory ANS reflexes, VR decreases to zero when the RA pressure rises to what number in mmHg?
Answer
-
4
-
5
-
6
-
7
Question 31
Question
When both arterial and venous pressure flow in the systemic circulation [blank_start]ceases[blank_end].
Answer
-
ceases
-
increases
-
decreases
Question 32
Question
Most of the resistance to venous return occurs where?
Answer
-
Arterioles
-
Veins
-
Smaller arteries
Question 33
Question
Select what can compensate in resistance to venous return:
Answer
-
`small artery
-
aorta
-
arterioles
-
venuoles
Question 34
Question
What is another word for preload?
Answer
-
End-diastolic pressure
-
Venous return
-
Afterload
Question 35
Question
Regardless of the chamber, the [blank_start]preload[blank_end] is related to the chamber volume just prior to contraction.
Answer
-
preload
Question 36
Question
Factors that increase preload include all except the following:
Answer
-
Increased venous return
-
Decreased venous compliance
-
Decreased thoracic blood volume
-
Increased thoracic blood volume
Question 37
Question
What is the pressure within the thoracic space between the organs (lungs, heart, vena cava) and the chest wall?
Answer
-
intrapleural pressure (Ppl)
-
Preload
-
Pulmonary filling pressure
-
intrarterial pressure
Question 38
Question
[blank_start]Skeletal muscle[blank_end] has to do with venous return because the one-way valves in the veins of the legs and arms are instrumental in directing blood flow away from the limbs and towards the heart.
Veins within large skeletal muscle groups also undergo compression as muscles contract and decompress as the muscles relax.
Answer
-
Skeletal muscle
-
Cardiac muscle
-
Smooth muscle
Question 39
Question
The Oxygen Fick Method, indicator dilution method, echocardiography, and ventriculogram are all methods of measuring [blank_start]cardiac output[blank_end].
Answer
-
cardiac output
Question 40
Question
The Oxygen Fick Principle states that:
[blank_start]Cardiac Output[blank_end] (L/min) = 02 absorbed per minute by the lungs (mL/min) / arteriovenous 02 difference (mL/L of blood)
Answer
-
Cardiac Output
Question 41
Question
Place in order the electrical pathways of the heart.
[blank_start]3[blank_end] AV node
[blank_start]1[blank_end] SA node
[blank_start]2[blank_end] Internodal pathway
[blank_start]4[blank_end] Left and right bundles of Purkinje fibers
Answer
-
1
-
2
-
3
-
4
-
1
-
2
-
3
-
4
-
1
-
2
-
3
-
4
-
1
-
2
-
3
-
4
Question 42
Question
Identify the pace of each area of the heart.
SA Node: [blank_start]70 - 80 BPM[blank_end]
AV Node: [blank_start]40 - 60 BPM[blank_end]
Purkinje Fibers: [blank_start]15 - 40 BPM[blank_end]
Answer
-
70 - 80 BPM
-
40 - 60 BPM
-
15 - 40 BPM
Question 43
Question
Heart muscle _________________.
Answer
-
is single-nucleated
-
lacks gap junctions
-
is syncytial
-
lacks striations
Question 44
Question
[blank_start]Sinus Node[blank_end] (where normal rhythmical impulse is generated) -> [blank_start]Internodal Pathways[blank_end] (conduct impulse from SA node to AV node) -> [blank_start]AV Node[blank_end] (delays impulse from atria to ventricles) -> [blank_start]AV Bundle[blank_end] (conducts impulse from atria to ventricles) -> Right & Left Bundle branches of Purkinje fibers (conduct impulse to ALL parts of the [blank_start]ventricles[blank_end])
Answer
-
Internodal Pathways
-
Sinus Node
-
AV Node
-
AV Bundle
-
ventricles
Question 45
Question
There are almost no contractile fibers in the SA node.
Answer
- True
- False
Question 46
Question
The SA node is located in the [blank_start]superior posterolateral wall[blank_end] of the right atrium, slightly below and lateral to the opening of the [blank_start]SVC[blank_end].
Answer
-
superior posterolateral wall
-
SVC
Question 47
Question
Which of the following is NOT a type of cardiac muscle ion channel?
Answer
-
Fast sodium channels
-
L-type calcium channels
-
Ligand-gated calcium channels
-
Potassium channels
Question 48
Question
The SA node has [blank_start]spontaneous[blank_end] depolarization.
Answer
-
spontaneous
Question 49
Question
Select the membrane potential for the SA node.
Answer
-
-40 to -50
-
-30 to -40
-
-60 to -70
-
-55 to -60
Question 50
Question
At what membrane threshold potential do slow Na-Ca channels to open up?
Answer
-
-30 mV
-
-40 mV
-
-50 mV
-
-60 mV
Question 51
Question
Place what is happening in the SA node with its appropriate location.
{kind=link}
Answer
-
Slow depolarization due to Na & Ca leak.
-
Na-Ca channels open.
-
K channels open during repolarization
Question 52
Question
Match the channels with the appropriate description:
[blank_start]I na (Fast Na Channels)[blank_end]
Rapid depolarizing phase of AP
• Atrial and ventricular muscle & in Purkinje fibers • (inactive at -55)
[blank_start]Slow Na Current:[blank_end] inherent leakiness of the SA node is responsible for self-excitation
[blank_start]K+ Current Ik[blank_end]
Responsible for repolarizing phase of AP in
ALL cardiomyocytes
[blank_start]Ca2+ current(ICa)[blank_end] •Depolarizing phase of AP
• SA node and AV node
• Also triggers contractions in all cardiomyocytes
Answer
-
I na (Fast Na Channels)
-
Slow Na Current:
-
K+ Current Ik
-
Ca2+ current(ICa)
Question 53
Question
•[blank_start]Self-excitation[blank_end] to cause AP (leaky Na+ & Ca channels) -> Recovery from AP (K+ channels open) -> [blank_start]Hyperpolarization[blank_end] after AP is over (K+ channels remain open) -> Drift of the "Resting" Potential to [blank_start]Threshold[blank_end] (leaky Na+ & Ca channels) -> [blank_start]Re-excitation[blank_end] to elicit another cycle
Answer
-
Self-excitation
-
Hyperpolarization
-
Threshold
-
Re-excitation
Question 54
Question
The [blank_start]inherent leakiness[blank_end] of the sinus nodal fibers to sodium and calcium ions causes their self-excitation.
Answer
-
inherent leakiness
Question 55
Question
The SA node has no true resting potential.
Answer
- True
- False
Question 56
Question
Label the contractile cell or autorhythmic cell.
{kind=link}
Answer
-
Autorhythmic cell
-
Contractile cell
-
Autorhythmic cell
-
Contractile cell
Question 57
Question
Assign the appropriate label to what is happening in the ventricular myocyte.
{kind=link}
Answer
-
Na channels open
-
Na channels close
-
Ca channels open; fast K channels close
-
Ca channels close; slow K channels open
-
Resting potential
Question 58
Question
[blank_start]Bachman's Bundle:[blank_end] Anterior interartrial band carries impulses to left atrium.
Answer
-
Bachman's Bundle:
Question 59
Question
The delay in the AV node is:
Answer
-
0.04 seconds
-
0.09 seconds
-
0.10 seconds
-
.20 seconds
Question 60
Question
The delay in the AV bundle is:
Answer
-
.04
-
0.09
-
0.10
-
0.14
Question 61
Question
The total delay in AV node/AV bundle system is [blank_start]0.13[blank_end] seconds.
Answer
-
0.13
Question 62
Question
The [blank_start]AV node[blank_end] is located in the posterior wall of the right atrium immediately behind the tricuspid valve
Answer
-
AV node
Question 63
Question
The Bundle branches and then divide into extensive system of [blank_start]Purkinje fibers[blank_end]
Answer
-
Purkinje fibers
Question 64
Question
Transmission time between A-V bundles and
fibers is:
Answer
-
0.04 seconds
-
0.10 seconds
-
0.90 seconds
-
0.06 seconds
Question 65
Question
The Purkinje fibers transmit impulses [blank_start]faster[blank_end] than other fibers.
Answer
-
faster
-
slower
Question 66
Question
The Purkinje fibers are [blank_start]larger[blank_end] than ventricular muscle fibers.
Answer
-
larger
-
smaller
Question 67
Question
The Purkinje fibers have [blank_start]high[blank_end] levels of permeability of the gap junctions between successive cells in the conducting pathways.
Answer
-
high
-
low
Question 68
Question
The [blank_start]SA Node[blank_end] is the pacemaker
Answer
-
SA Node
Question 69
Question
SA node discharges both the AV node & Purkinje fibers [blank_start]before[blank_end] either of these can undergo self-excitation.
Answer
-
after
-
during
-
before
Question 70
Question
Select the resting membrane potential of the ventricular muscle cell.
Answer
-
-55 to -60
-
-85 to -90
-
-100 to -110
-
40 to 60
Question 71
Question
What doesn't happen when the AV node is blocked?
Answer
-
Impulse can’t get past atria to ventricles
-
Atria continue beating at normal SA node rate and rhythm
-
New pacemaker in Purkinje system takes over driving ventricular contraction 15 to 40 bpm
-
New pacemaker is Bachman Bundle, which takes over driving the ventricular contraction.
Question 72
Question
Sudden AV block: Delay in pickup of the heart beat is the “[blank_start]Stokes-Adams[blank_end]” syndrome
Answer
-
Stokes-Adams
Question 73
Question
[blank_start]Parasympathetic[blank_end] (vagal) activation decreases conduction velocity (negative [blank_start]dromotropy[blank_end]) at the AV node
• Decreases slope of Phase [blank_start]4[blank_end]
• leads to [blank_start]slower[blank_end] depolarization of adjacent cells, and reduced velocity of conduction
Answer
-
Parasympathetic
-
Sympathetic
-
dromotropy
-
inotropy
-
0
-
3
-
4
-
slower
-
faster
Question 74
Question
Parasympathetic fibers in the heart are [blank_start]muscarinic[blank_end].
Answer
-
nicotinic
-
muscarinic
Question 75
Question
Acetylcholine released by [blank_start]vagus[blank_end] nerve
• Binds to cardiac [blank_start]muscarini[blank_end]c receptors
• [blank_start]Decreases[blank_end] intracellular cAMP
Answer
-
vagus
-
muscarinic
-
Decreases
Question 76
Question
[blank_start]Vagal[blank_end] stimulation releases acetylcholine. This goes to muscarinic receptors that decrease cAMP. This causes increased K permeability, which decreases transmission of impulses. Ventricular escape occurs.
Answer
-
Vagal
-
Adrenergic
-
Sympathetic
Question 77
Question
[blank_start]Digitalis[blank_end] increases the vagal activity to the heart.
Answer
-
Digitalis
Question 78
Question
Sympathetic nerves release [blank_start]norepinephrine[blank_end].
Answer
-
norepinephrine
-
aCH
-
cAMP
Question 79
Question
[blank_start]Sympathetic[blank_end] activation increases conduction velocity in the AV node • Rate of depolarization increased
• i.e. slope of Phase [blank_start]0[blank_end] increase
• Leads to more rapiddepolarization of adjacent cellsàmore rapid conduction of action
potentials
• [blank_start]Positive[blank_end] dromotropy
Answer
-
Sympathetic
-
Parasympathetic
-
0
-
3
-
4
-
Positive
-
Negative
Question 80
Question
Normal delay of conduction thru AV node reducedàtime between
atrial and ventricular contraction reduced
• Increase in AV conduction velocity manifests as [blank_start]decrease[blank_end] in P-R interval on EKG
Answer
-
decrease
-
increase
Question 81
Question
[blank_start]Esmolol[blank_end] is a beta blocker that's metabolized in the blood.
Answer
-
Esmolol
Question 82
Question
Parasympathetic Nerves
• Releases [blank_start]acetylcholine[blank_end]
• Binds to [blank_start]muscarinic[blank_end]
• [blank_start]Increases[blank_end] conductivity of K and [blank_start]decreases[blank_end] conductivity of Ca2+
• [blank_start]Decreases[blank_end] heart rate of rhythm and excitability of AV junctional fibers and AV node
• Excitatory signals are no longer transmitted into the ventricles.
Answer
-
acetylcholine
-
norepinephrine
-
muscarinic
-
nicotinic
-
Decreases
-
Increases
-
decreases
-
increases
-
Decreases
-
Increases
Question 83
Question
SympatheticNerves
• Releases [blank_start]norepinephrine[blank_end] at
sympathetic endings.
• Binds to [blank_start]β1[blank_end] receptors
• [blank_start]Increases[blank_end] the rate of sinus nodal discharge.
• [blank_start]Increases[blank_end] the overall heart activity.
• [blank_start]Increases[blank_end] the permeability of Na+ and Ca2+ ions.
Answer
-
acetylcholine
-
norepinephrine
-
β1
-
β2
-
Decreases
-
Increases
-
Decreases
-
Increases
-
Decreases
-
Increases
Question 84
Question
Phase 0 is [blank_start]depolarization[blank_end].
Answer
-
depolarization
Question 85
Question
Conduction velocity is altered by:
Sympathetic stimulation ([blank_start]increases[blank_end])
Vagal stimulation ([blank_start]decreases[blank_end])
Ischemia/Hypoxia: [blank_start]decreases[blank_end]
Drugs (adrenergic and cholinergic): increase or decrease
Answer
-
decreases
-
increases
-
decreases
-
increases
-
decreases
-
increases
Question 86
Question
Label the effects of the parasympathetic and sympathetic nerve activations appropriately.
{kind=link}
Answer
-
Sympathetic
-
Vagal/Parasympathetic
Question 87
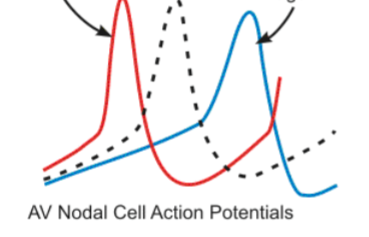
Question
Key Difference in Pacemaker Cell AP
•The higher the slope of Phase [blank_start]4[blank_end], the higher the rate
•Vagal stimulation [blank_start]slows[blank_end] phase 4 depolarization
•Rate slows •Catecholamines speed it up
Answer
-
0
-
3
-
4
-
slows
-
speeds
Question 88
Question
Essentially/primary hypertension is [blank_start]95[blank_end] percent of cases.
Secondary/demonstrable causes are [blank_start]5[blank_end] percent of cases.
Answer
-
95
-
5
Question 89
Question
[blank_start]Salt[blank_end] and H2O retention is the final common pathway shared by all of these etiologies; Interplay of these 2 determined by kidneys
Answer
-
Salt
Question 90
Question
Extracellular fluid volume increases, then arterial pressure [blank_start]increases[blank_end]
• increase in arterial pressure, then the kidneys to [blank_start]lose[blank_end] Na+ and water then returns arterial BP to return to normal
Answer
-
decreases
-
increases
-
lose
-
retain
Question 91
Question
The [blank_start]renal function curve[blank_end] depicts the effect of increasing arterial BP on urinary output (UOP).
Answer
-
renal function curve
Question 92
Question
Fill in the blanks for the renal function curve.
• [blank_start]50[blank_end] mm Hg = UOP = 0
• [blank_start]100[blank_end] mm Hg = normal UOP
• [blank_start]200[blank_end] mm Hg = 6-8 times normal
Answer
-
50
-
100
-
150
-
200
Question 93
Question
Over time, output must = intake
• The point at which this occurs is where the two lines intersect is known as the [blank_start]equilibrium point[blank_end].
• The equilibrium point tends to be at an arterial BP of [blank_start]100[blank_end] mm Hg
Answer
-
equilibrium point
-
100
Question 94
Question
If arterial BP [blank_start]increases[blank_end] then the loss of H2O and Na+ will be greater than the intake → a [blank_start]decrease[blank_end] in fluid volume and BP will [blank_start]decrease[blank_end] until the arterial pressure falls exactly back to the equilibrium point
Answer
-
decreases
-
increases
-
decrease
-
increase
-
decrease
-
increase
Question 95
Question
If arterial BP falls below the equilibrium point, intake of Na+ and H2O will be [blank_start]greater[blank_end] than the output → an [blank_start]increase[blank_end] in fluid volume and BP until the arterial pressure returns exactly back to the equilibrium point
Answer
-
greater
-
less
-
decrease
-
increase
Question 96
Question
This equilibrium point for the kidneys will occur as long as (1) [blank_start]renal output[blank_end] of salt and water and (2) [blank_start]intake[blank_end] of salt and water remain in balance
Answer
-
renal output
-
intake
Question 97
Question
2 primary ways to change long-term arterial pressure levels
• Shifting [blank_start]equilibrium point[blank_end] of the renal output curve to a different pressure
• Changing level of [blank_start]H2O[blank_end] and Na+ intake
Answer
-
equilibrium point
-
H2O
Question 98
Question
[blank_start]Renal artery stenosis[blank_end] can cause the renal output curve and equilibrium point to shift to the right.
Answer
-
Renal artery stenosis
Question 99
Question
As the intake of water/salt
[blank_start]increases[blank_end], the equilibrium point shifts to the right (160 mm Hg)
• If there were a [blank_start]decrease[blank_end] in water/salt intake, the equilibrium point and the arterial BP would also decrease
Answer
-
decreases
-
increases
-
decrease
-
increase
Question 100
Question
Effect of Total Peripheral Resistance TPR
Acutely, if TPR [blank_start]increases[blank_end], arterial BP [blank_start]increases[blank_end]
• Arterial pressure = CO x TPR
Answer
-
decreases
-
increases
-
decreases
-
increases
Question 101
Question
If renal vascular resistance (RVR) is NOT affected (i.e., increased when TPR is increased), then the equilibrium point for BP [blank_start]will not[blank_end] change
Answer
-
will
-
will not
Question 102
Question
Changes in TPR do not typically affect the [blank_start]long-term[blank_end] arterial pressure level
Answer
-
long-term
-
short-term
Question 103
Question
Which of the following conditions does NOT have a long-term effect on TPR and therefore equilibrium point.
Answer
-
Beriberi
-
AV shunts
-
Pulmonary disease
-
Paget's disease
-
Diabetes mellitus
-
Hypothyroidism
Question 104
Question
An increase in TPR without any change in renal resistance would:
Answer
-
Transiently increase arterial pressure
-
Transiently increase sodium and water excretion
-
Decrease extracellular fluid (ECF)
-
All of the above
Question 105
Question
autoregulation— blood volume has [blank_start]increased[blank_end] then tissue blood flow [blank_start]increases[blank_end] throughout body; [blank_start]constricts[blank_end] blood vessels everywhere
Answer
-
decreased
-
increased
-
decreases
-
increases
-
constricts
-
vasodilates
Question 106
Question
As Na+ intake increases, two things happen:
• ECF osmolality [blank_start]increases[blank_end] → stimulation of the thirst center to drink more water to return the ECF salt concentration to normal
• This excess water intake → ↑ ECFV
• The increased osmolality also stimulates the release of [blank_start]ADH[blank_end] → kidney reabsorption of H2O → ↑ ECFV
Answer
-
decreases
-
increases
-
ADH
-
Angiotensin
-
Aldosterone
Question 107
Question
The first stage in a volume-loading hypertension is an increase in [blank_start]cardiac output[blank_end]. The reduction in total peripheral resistance is more related to a [blank_start]baroreceptor[blank_end] effect.
The initial increase in BP is the result of the rise in CO.
Answer
-
cardiac output
-
baroreceptor
Question 108
Question
2nd stage – • HTN exists
• CO returns to near [blank_start]normal[blank_end] • At same time [blank_start]increased[blank_end] TPR
occurs
Answer
-
normal
-
increased
Question 109
Question
Which of the following doesn't happen several weeks following initial-onset volume loading?
Answer
-
Hypertension
-
Significant increase in TPR
-
Nearly complete return of ECFV, BV, and CO back to normal.
-
Significant decrease in TPR.
Question 110
Question
Angiotensinogen-converting enzyme (ACE) lives mostly in where?
Answer
-
Liver
-
Lungs
-
Kidneys
-
Heart
Question 111
Question
Where is renin mostly made and stored?
Answer
-
Liver
-
Lungs
-
Kidneys
-
Heart
Question 112
Question
Which enzyme in the blood and tissues inactivates angiotensin II?
Answer
-
Angiotensin I
-
Renin
-
Angiotensinases
-
Aldosterone
Question 113
Question
Angiotensin Effect on Retention of Salt/Water By Kidneys
1. Direct renal effects
• Renal arteriole [blank_start]constriction[blank_end]
• Less blood flow thru kidneysàless fluid filtered thru glomeruli into the tubules
• Slowedbloodflowresultsinlessperitubularcapillariespressureàrapidreabsorption of fluid from tubules
• Act directly on tubular cells to#tubular [blank_start]reabsorption[blank_end] of sodium & water
Answer
-
constriction
-
reabsorption
Question 114
Question
causes aldosterone secretion by adrenal glands
• Results in significant [blank_start]increase[blank_end] in sodium reabsorption by renal tubules then H2Oretention, which leads to [blank_start]increase[blank_end] in fluid volume and an increase in BP
Answer
-
increase
-
increase
Question 115
Question
Which of the following does not increase renal excretion of Na and water-increasing BP?
Answer
-
Angiotensin II
-
Aldosterone
-
Atrial natriuretic peptide
-
Sympathetic nervous system
-
Endothelin
Question 116
Question
Factors that decrease renal excretion of Na & Water to increase BP:
1. [blank_start]Aldosterone[blank_end]
2. [blank_start]Angiotensin II[blank_end]
3. [blank_start]Endothelin[blank_end]
4. [blank_start]Sympathetic nervous system[blank_end]
Factors that Increase Renal Excretion of Na and Water, Reducing Blood Pressure
1. [blank_start]Atrial natriuretic peptide[blank_end]
2. [blank_start]Dopamine[blank_end]
3. [blank_start]Nitric oxide[blank_end]
Answer
-
Aldosterone
-
Angiotensin II
-
Endothelin
-
Sympathetic nervous system
-
Atrial natriuretic peptide
-
Dopamine
-
Nitric oxide
Question 117
Question
Atrial natriuretic peptide is secreted from the [blank_start]right atrium[blank_end].
Answer
-
right atrium
Question 118
Question
[blank_start]Angiotensin II[blank_end]
• Constricts renal arteriolesàless blood flow to kidneys
• Stimulates aldosterone secretionàincreases Na+ reabsorption
• Directly stimulates Na+ reabsorption in proximal tubules, loops of Henle, distal tubules and collecting tubules
[blank_start]• Aldosterone[blank_end]
• secreted by adrenal glands
• Sodium reabsorption which is followed by water reabsorption
• [blank_start]Sympathetic nervous activity[blank_end]
• Constricts renal arterioles, reducing GFR; low levels of SNS activation acts on
alpha receptors on renal tubular cells increasing Na reabsorption; also stimulates release of renin and AGII formation
• [blank_start]Endothelin[blank_end]
• Amino peptide in endothelial cells released in response to vessel trauma • Intense vasoconstriction
Answer
-
Angiotensin II
-
• Aldosterone
-
Sympathetic nervous activity
-
Endothelin
Question 119
Question
[blank_start]Atrial natriuretic peptide[blank_end]
¤ Causes decreased Na and H2O
reabsorptionà#UOPàreturn blood volume to normalà$BP
̈[blank_start]Nitric oxide[blank_end]
¤Vasodilator
¤ Basal level of NO in kidneys, helps
maintain renal vasodilation allowing normal renal excretion of salt/water
̈[blank_start]Dopamine[blank_end]
¤ At low doses, stimulates dopamine-
1 receptors
nCause renal vessel vasodilation nStimulates natriuresis
Answer
-
Atrial natriuretic peptide
-
Nitric oxide
-
Dopamine
Question 120
Question
Use the dropdown to choose the appropriate stage in the cardiac cycle:
[blank_start]Diastole[blank_end]: Muscle re-establishing Na/K/Ca gradient
[blank_start]Systole[blank_end]: Contraction of muscle & ejection of blood from chambers
[blank_start]Systole[blank_end]: Muscle stimulated by action potential
[blank_start]Diastole[blank_end]: Relaxation of muscle & filling chambers with blood
Answer
-
Diastole
-
Systole
-
Diastole
-
Systole
-
Diastole
-
Systole
-
Diastole
-
Systole
Question 121
Question
Drag and drop to the appropriate location on the cardiac cycle:
[blank_start]P-wave[blank_end]: Also known as the atrial wave, represents the spread of depolarization
[blank_start]QRS[blank_end]: Ventricle depolarization
[blank_start]T-wave[blank_end]: Ventricular repolarization
Answer
-
P-wave
-
QRS
-
T-wave
Question 122
Question
Choose if the following descriptions match the atria or the ventricles:
[blank_start]Atria[blank_end]: Contraction enhances ventricular filling.
[blank_start]Ventricles[blank_end]: Blood flows from the RV and LV into the pulmonary artery and aorta
[blank_start]Atria[blank_end]: Blood flows from the IVC and SVC
Answer
-
Atria
-
Ventricles
-
Atria
-
Ventricles
-
Atria
-
Ventricles
Question 123
Question
True or false: The amount of blood pumped out of the RV will always equal the amount of blood pumped out of the LV.
Answer
- True
- False
Question 124
Question
The fullest the ventricle will be is the end diastolic volume (EDV). This number is what?
Answer
-
40 to 50 mL
-
50 to 100 mL
-
110 to 120 mL
-
150 to 200 mL
Question 125
Question
The emptiest the ventricle will be is the end systolic volume (ESV). What number is this?
Answer
-
40 to 50 mL
-
50 to 100 mL
-
100 to 150 mL
-
150 to 200 mL
Question 126
Question
The comparison of the end diastolic volume to the end systolic volume is what?
Answer
-
Total peripheral resistance
-
Pulmonary filling pressure
-
Ejection fraction or stroke volume
-
Arterial pressure
Question 127
Question
The average ejection fraction in a healthy adult is what?
Answer
-
30 percent
-
40 percent
-
50 percent
-
60 percent
Question 128
Question
Select the two factors that can change the EDV and the ESV.
Answer
-
Strength of contraction
-
Increases in diastolic filling
Question 129
Question
Drag and drop the appropriate part of the heart to the area it works.
[blank_start]Right Ventricle (RV)[blank_end]: Deoxygenated blood from RA
[blank_start]Right Atrium (RA)[blank_end]: Deoxygenated blood from IVC and SVC
[blank_start]Left Ventricle (LV)[blank_end]: Oxygenated blood from LA
[blank_start]Left Atrium (LA)[blank_end]: Oxygenated blood from pulmonary circulation
Answer
-
Right Ventricle (RV)
-
Right Atrium (RA)
-
Left Ventricle (LV)
-
Left Atrium (LA)
Question 130
Question
The atrium is the [blank_start]weaker[blank_end] pump of the heart.
The [blank_start]right[blank_end] ventricle sends blood to the pulmonary circulation.
The [blank_start]left[blank_end] ventricle sends blood to the peripheral circulation.
Answer
-
stronger
-
weaker
-
left
-
right
-
left
-
right
Question 131
Question
Name the three types of cardiac muscle in alphabetical order:
[blank_start]Atrial[blank_end] muscle
[blank_start]Excitatory[blank_end] / conductive muscle
[blank_start]Ventricular[blank_end] muscle
Answer
-
Atrial
-
Excitatory
-
Ventricular
Question 132
Question
Which of the following is a difference between cardiac muscle and skeletal muscle?
Answer
-
Striations
-
Actin and myosin filaments
-
Low-Resistance intercalated disks
Question 133
Question
Heart muscle is a [blank_start]syncytium[blank_end] of many heart muscle cells. When one cell becomes excited the action potential spreads to all of them
Answer
-
syncytium
Question 134
Question
Identify the three characteristics of cardiac muscle and how an impulse travels.
[blank_start]Autorhythmic cell[blank_end]
[blank_start]Gap junction[blank_end]
[blank_start]Contractile cell[blank_end]
Answer
-
Autorhythmic cell
-
Nerve
-
Gap junction
-
Neuromuscular junction
-
Contractile cell
-
Muscle cell
Question 135
Question
Contraction of cardiac muscle is initiated by the [blank_start]SA node[blank_end].
Answer
-
SA node
-
AV node
-
Bundle of His
-
Purkinje fibers
Question 136
Question
Action Potentials:
The resting membrane potential of cardiac muscle is [blank_start]-85 to -95[blank_end].
The action potential of cardiac muscle is [blank_start]105[blank_end] millivolts.
The plateau lasts [blank_start]0.2 to 0.3[blank_end] seconds in ventricular muscle -- much longer than skeletal muscle.
Answer
-
-85 to -95
-
-100 to -120
-
-60 to -70
-
105
-
120
-
95
-
0.2 to 0.3
-
0.3 to 0.4
-
0.5 to 0.7
Question 137
Question
Which of the following is responsible for the influx of intracellular calcium in cardiac muscle?
Answer
-
Intracellular sarcoplasmic reticulum
-
Activation of the dihydropridene (DHP) channels
-
Activation of the ligand-gated channels
-
Passive sodium flow
Question 138
Question
In cardiac muscle, after the outflow of K+ ions during an action potential (AP), the permeability to K+ ions [blank_start]decreases[blank_end] tremendously.
This prevents the early return of the AP voltage to its resting level.
Answer
-
decreases
-
increases
Question 139
Question
Action potentials of the cardiac cell is much [blank_start]longer[blank_end] than the AP of the nerve cell.
Answer
-
longer
-
shorter
Question 140
Question
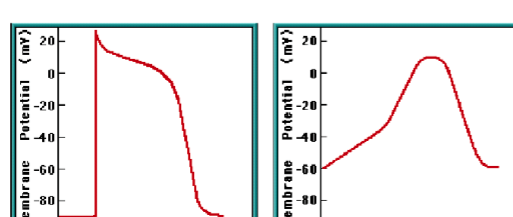
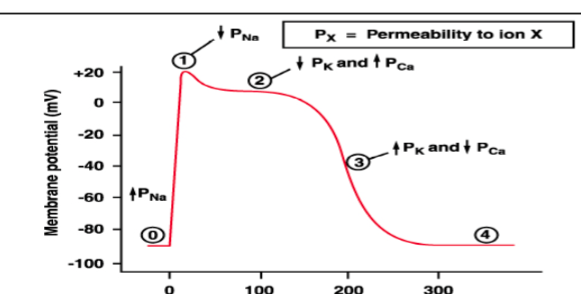
Label the portions of the ventricular muscle action potential:
{kind=link}
Answer
-
Fast Na channels open, then slow Ca chan
-
K channels open
-
Ca channels open more
-
K channels open more
-
Resting membrane potential
Question 141
Question
Put the steps of rapid depolarization of a cardiac cell in order:
[blank_start]Rapid change membrane pot. from + to -[blank_end]
[blank_start]Voltage pauses above 0 mV level[blank_end]
[blank_start]Membrane potential inc. to Na[blank_end] and [blank_start]dec to K[blank_end]
[blank_start]Begins absolute refractory period[blank_end]
[blank_start]Cardiac muscle can't be excited again.[blank_end]
Answer
-
Rapid change membrane pot. from + to -
-
Voltage pauses above 0 mV level
-
Membrane potential inc. to Na
-
dec to K
-
Begins absolute refractory period
-
Cardiac muscle can't be excited again.
Question 142
Question
Put the steps of initial re-polarization in order for cardiac muscle:
1. [blank_start]Movement of Na into cells STOPS[blank_end]
2. [blank_start]Sodium gates close[blank_end]
3. [blank_start]C enters cell.[blank_end]
4. [blank_start]K leaves cell.[blank_end]
5. [blank_start]When Na stops, voltage begins to decline[blank_end].
6. [blank_start]SLOW influx of Ca begins via slow Ca[blank_end] channels.
Answer
-
Movement of Na into cells STOPS
-
Sodium gates close
-
C enters cell.
-
K leaves cell.
-
When Na stops, voltage begins to decline
-
SLOW influx of Ca begins via slow Ca
Question 143
Question
SA node action potential has [blank_start]fewer[blank_end] phases than other cardiac muscle types.
Answer
-
fewer
-
more
-
the same amount
Question 144
Question
Place in order the phases of the SA node.
Phase 0: [blank_start]Na & Ca influx[blank_end]
Phase 3: [blank_start]K efflux[blank_end]
Phase 4: [blank_start]Progressively slowed K efflux[blank_end] & intrinsic [blank_start]Na influx leak causes spontaneous[blank_end] depolarization.
Answer
-
Na & Ca influx
-
K efflux
-
Progressively slowed K efflux
-
Na influx leak causes spontaneous
Question 145
Question
[blank_start]Refractory period:[blank_end] During this time, the cardiac muscle cannot be re-excited.
[blank_start]Relative refractory period:[blank_end] Cell can be excited, but the signal must be very strong. Example is an early or "premature" contraction.
Answer
-
Refractory period:
-
Relative refractory period:
Question 146
Question
Cardiac T-tubules are five times [blank_start]larger[blank_end] than skeletal muscle T-tubules.
Answer
-
larger
-
smaller
Question 147
Question
Excess Ca causes [blank_start]spastic contraction[blank_end].
Low Ca causes [blank_start]cardiac dilation[blank_end].
Answer
-
spastic contraction
-
cardiac dilation
Question 148
Question
Atrioventricular (AV) valves allow blood flow in one direction FROM atria to ventricle.
[blank_start]Tricuspid valve[blank_end]: Between RA & RV
[blank_start]Mitral valve:[blank_end] Between LA & LV
Answer
-
Tricuspid valve
-
Mitral valve:
Question 149
Question
The semilunar valves are the outlet valves of the ventricles. They provide blood from each ventricle into large outflow tract vessel.
[blank_start]Pulmonary valve[blank_end]: Between RV & Pulmonary artery
[blank_start]Aortic valve[blank_end]: Between LV & aorta
Answer
-
Pulmonary valve
-
Aortic valve
Question 150
Question
Label the parts of the Atrial Pressure Wave:
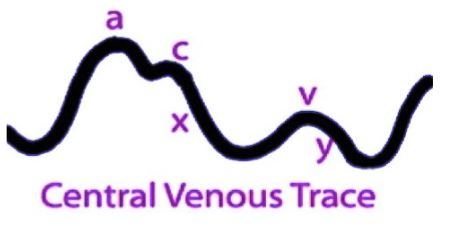{kind=link}
Answer
-
Atrial Contraction
-
Ventricular contraction (AV valves bulge
-
flow of blood into the atria
Question 151
Question
Diastole
-Isovolumic relaxation
-A-V valves [blank_start]open[blank_end]
-Rapid inflow of blood
-Diastasis
-Slow flow into ventricle
-Atrial systole
-Extra blood in following P wave.
-Accounts for 20-25 % of filling
Answer
-
close
-
open
Question 152
Question
Systole
1. Isovolumic contraction
2. A-V valves [blank_start]close[blank_end]
ventricular press>atrial press
3. Aortic valve opens
4. Ejection phase
5. Aortic valve closes
Answer
-
close
-
open
Question 153
Question
Aortic Pressure Curve
1. Aortic pressure starts to [blank_start]increase[blank_end] during systole after the aortic valve opens
2. Aortic pressure [blank_start]decreases[blank_end] toward the end of the ejection phase.
3. Aftertheaorticvalvecloses,an incisura occurs because of sudden cessation of back-flow toward left ventricle.
4. Aortic pressure [blank_start]decreases[blank_end] slowly during diastole because of the elasticity of the aorta.
Answer
-
decrease
-
increase
-
decreases
-
increases
-
decreases
-
increases
Question 154
Question
[blank_start]Ejection Fraction[blank_end] = (SV/EDV) x 100
Answer
-
Ejection Fraction
Question 155
Question
Compute the following to calculate ejection fraction:
EDV = 150
End-Systolic Volume = 50
Answer
-
55%
-
60%
-
67%
-
70%
Question 156
Question
If heart rate is 70 and stroke volume is 70, what is the cardiac output?
Answer
-
3.5 L/min
-
4 L/min
-
4.9 L/min
-
6 L/min
Question 157
Question
The normal value for ejection fraction is [blank_start]60 to 70[blank_end] percent.
An EF less than [blank_start]40[blank_end] percent is associated with significant left ventricular impairment.
Answer
-
60 to 70
-
50 to 60
-
40 to 60
-
40
-
50
-
30
Question 158
Question
Select the normal valve area for the Aortic valve.
Answer
-
1.5 to 3.0
-
2.5 to 4.5
-
3 to 5
-
4 to 6
Question 159
Question
What is the normal valve area for the mitral valve?
Answer
-
2.5 to 4.5
-
3 to 5
-
1 to 3
-
4 to 6
Question 160
Question
Mean Pressure Gradient (mmHg)
1. Aortic <[blank_start]5[blank_end]
2. Mitral <[blank_start]2[blank_end]
Answer
-
5
-
3
-
2
-
5
-
3
-
2
Question 161
Question
Because of smaller opening, velocity through aortic & pulmonary valves [blank_start]exceed[blank_end] that through the A-V valves.
Answer
-
exceed
-
are less than
Question 162
Question
Label the ventricular pressure/volume loops.
{kind=link}
Answer
-
Mitral Valve (MV) Closes
-
Aortic Valve (AV) Opens
-
Aortic Valve Closes
-
Mitral Valve Opens
-
Stroke Volume (70mL)
-
End Systolic Volume (50mL)
-
End diastolic volume (120 mL)
-
Afterload
-
Preload
Question 163
Question
Know these key points from Ray's powerpoint.
{kind=link}
Answer
-
Systole begins, diastole ends
-
Systole ends, Diastole begins
Question 164
Question
Increased contractility [blank_start]increases[blank_end] stroke volume.
Answer
-
decreases
-
increases
Question 165
Question
Increased preload [blank_start]increases[blank_end] stroke volume.
Answer
-
decreases
-
increases
Question 166
Question
Increased afterload [blank_start]decreases[blank_end] stroke volume.
Answer
-
decreases
-
increases
Question 167
Question
Increasing the arterial pressure in the aorta does not decrease the CO until the MAP rises above what?
Answer
-
80
-
100
-
120
-
160
Question 168
Question
Frank-Starling Law
Intrinsic ability of the heart to adapt to increasing volumes of inflowing blood
Greater the heart muscle is stretched during filling, the [blank_start]greater[blank_end] force of contraction, the greater amt of blood pumped to aorta
Answer
-
greater
-
lesser
Question 169
Question
The Frank-Starling Relationship says that
[blank_start]Increased[blank_end] ventricular filling
[blank_start]Increased[blank_end] Preload
[blank_start]Increased[blank_end] LVEDP
[blank_start]Increased[blank_end] Stroke Volume
Answer
-
Decreased
-
Increased
-
Decreased
-
Increased
-
Decreased
-
Increased
-
Decreased
-
Increased
Question 170
Question
What are the ways to increase cardiac output?
[blank_start]Increase[blank_end] contractility
[blank_start]Increase[blank_end] preload
[blank_start]Decrease[blank_end] after load
Change the rate
Answer
-
Decrease
-
Increase
-
Decrease
-
Increase
-
Decrease
-
Increase
Want to create your own Quizzes for free with GoConqr? Learn more.