4103877
Descripción
Fichas por Emma Richardson6484, actualizado hace más de 1 año
|
|
Creado por Emma Richardson6484
hace alrededor de 10 años
|
|
| Pregunta | Respuesta |
| Psoriasis | |
| Psoriasis (nail pitting) | |
| Koebner's Phenomenon (psoriasis post-trauma) | |
| Psoriasis Vulgaris (trunk) | |
| Psoriasis Vulgaris (extensor surfaces) | |
| Psoriasis Vulgaris (knees & extensor surfaces) | |
| Guttate Psoriasis - discrete - all over | |
| Guttate Psoriasis (dark skin) - discrete - all over | |
| Psoriasis - pitting - onycholysis (nail lifting) | |
| Psoriasis (scalp) | |
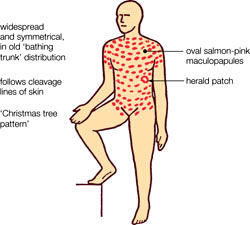
| Pityriasis Rosea - multiple red mac/pap progress to to oval, pink/red with fine scale in center - parallel skin tension lines (xmas tree distribution) | |
| Pityriasis Rosea - black skin --> hyper pigmented & @ folds (neck), proximal extremities, axillae, & groin | |
| Pityriasis Rosea | |
| Herald Patch - Pityriasis Rosea - preceded by prodrome (URI) - HHV-7 | |
| Herald Patch - Pityriasis Rosea DDX: - Secondary syphilis (palm/sole [≠ PR], LAD) - Tinea corporis - Guttate psoriasis - Parapsoriasis | |
| Acute Parapsoriasis (PLEVA) - recurrent crops 2-4 mm red papules - progress --> central crusts - can leave depressed scars "Chicken Pox that won't heal" | |
| PLEVA - can be very itchy | |
| Chicken Pox vs. PLEVA Mucosal involvement = ? | Chicken Pox (Varicella) |
| Chicken Pox vs. PLEVA NO mucosal involvement = ? | PLEVA |
| Chicken Pox vs. PLEVA Lasts 2 weeks = ? | Varicella |
| Chicken Pox vs. PLEVA Lasts 9-12 months = ? | PLEVA |
| Chronic Parapsoriasis (PLC: pityriasis lichenoides chronica) | |
| Chronic Parapsoriasis (PLC: pityriasis lichenoides chronica - salmon colored - oval plaques - central thin scale (≠ crust) - boxer shorts distribution - mimics PR | |
| PLEVA ~ Chicken pox | |
| Lichen Planus - polygonal - purple-red - papules | |
| Lichen Planus - polygonal - purple-red - papules | |
| Lichen Planus Nail dystrophy | |
| Lichen Planus Hypertrophic version: thick & scaly | |
| Lichen Planus Lower legs = scaly plaques | |
| Wickham's Striae (Lichen Planus) | |
| Lichen Striatus - along lines of blascho (migration route) - extremity - resolve on own over 3-6 months - skin colored / pink / brown | |
| Lichen Striatus | |
| SLE - Malar Rash Red scaly mac-pap eruption over nose & cheeks | |
| SLE - Discoid lesion Persistent focal plaques @ face, are & scalp. Nummular w/ atrophy & follicular accentuation. Disfiguring (Seal). | |
| SLE Erythematous scaly plaques on dorsal hand BETWEEN knuckles | |
| SLE Periungal erythema (dilated blood vessels) | |
| SLE Subacute cutaneous lupus erythematous | |
| Neonatal Lupus | |
| Dermatomyositis Gottron's papules: flat-topped, red/purple, scaly nodules OVER knuckles | |
| Dermatomyositis Heliotrope Rash (periorbital edema) | |
| Dermatomyositis (rash may precede muscle weakness by months WITHOUT pain) Heliotrope Rash | |
| Epithelial Cyst (Epidermoid / Sebaceous) Dilated | |
| Dermoid Cyst Newborn: lateral border of eyebrow OR in scalp More fixed to bone than epidermoid. | |
| Branchial Cyst Lateral aspect of neck (defect of embryological closure) | |
| Milia | |
| Milia | |
| Pilomatricoma - Adnexal tumor - cells of HAIR MATRIX - NOT fixed - blue (?) - stretched skin - Teeter totter sign (seesaw) | |
| Pilomatricoma Multi lobar papules NOT fixed Hard (calcify) | |
| Syringoma - Adnexal Tumor Cells of eccrine sweat glands. Eyelids, cheeks, etc. Most common in DOWN Syndrome | |
| Trichoepithelioma Cells of HAIR FOLLICLE Firm, Benign. Cheeks, nose. Confused with acne. | |
| Trichoepithelioma | |
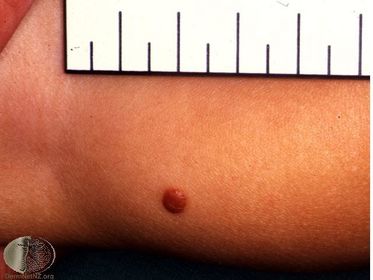
| Dermatofibroma well-defined. round. often pigmented. @ leg/trunk. SCAR BALL | |
| Dermatofibroma PINCH SIGN: lateral pressure produces DIMPLING on its surface Area of PREVIOUS TRAUMA (e.g. shaving) -- reactive proliferation of FIBROBLASTS | |
| Hypertrophic Scar Overgrowth of scar tissue. Remains at site of injury | |
| Keloid esp. @ earlobe, presternal area, neck, face No definition of border (noncompliant of previous scar) - shiny & hairless - progressively enlarging | |
| Neurofibroma BUTTON-HOLE sign (dx): involutes into skin Benign tumor of nerve sheath cells Elephantiasis = whole limb | |
| Plexiform Neurofibroma Large clustering of neurofibromas (often gathering of hair in that area). Often associated with neurofibromatosis. | |
| Lipoma - soft & squishy - SubQ nodules - Mobile (UNattached to overlying skin) - Solitary - Begin in adolescence (≠ children) - @ neck, chest, arms (forehead: elderly) | |
| Granuloma Annulare small, firm pap/nod Circle / semicircle Misdx: ringworm Usually solitary (can have multiple) @ ankles, WRISTS (aural areas, digits) Dusky violaceous or skin-colored hue | |
| Granuloma Annulare small, firm pap/nod Circle / semicircle Misdx: ringworm Usually solitary (can have multiple) @ ankles, wrists (aural areas, digits) Dusky violaceous or skin-colored hue | |
| Juvenile Xanthogranuloma (JXG) Orange/pink to yellow-brown. Soft nodules. Often MULTIPLE. Large accum. of MACROPHAGES @ dermis Also found on trunk, etc. | |
| Juvenile Xanthogranuloma (JXG) @ IRIS --> glaucoma (hyphema) | |
| Juvenile Xanthogranuloma (JXG) Orange/pink to yellow-brown. Soft nodules. Type of Non-Langerhan's Cell Histiocytosis. | |
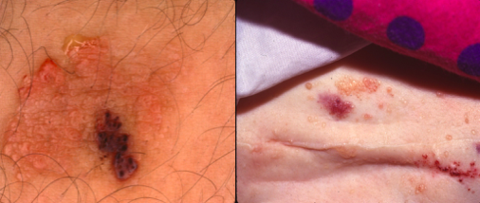
| Pyogenic Granuloma (PG) @ Acral areas: hands, fingers, face Solitary Dull red. Firm (perhaps pedunculated) BLEEDS easily: increased expression of vascular endothelial growth factor. | |
| Pyogenic Granuloma (PG) @ Acral areas Solitary. Dull red. Firm nodules. May be smooth/glistening...but often ulcerated & crusted if open. | |
| Langerhan Cell Histiocytosis (LCH) Discrete. Papules or nodules. Hemorrhage/petechia do NOT blanch Red, orange, and/or yellow-brown. Seborrheic Distribution. Crusted scaling of SCALP, post auricular, perianal, & axillary areas. | |
| Langerhan Cell Histiocytosis (LCH) Organs & lymph nodes may be affected. Diagnosis via Biopsy. Tx = chemotherapy | |
| Congenital Self-Healing Reticulohistiocytosis looks like LCH or PG (type of LCH) Solitary CRATERIFORM central erosion. No tx, but monitor over time. | |
| Benign Cephalic Histiocytosis JXG on the head (non-LCH). @ Face & neck. Resolve during childhood (≠ tx) | |
| Benign Cephalic Histiocytosis JXG on head (non-LCH) 2-5mm (small) Yellow-red to tan papules. | |
| Kawasaki Disease Mucocutaneous & lymph node 1. Abrupt high fever ≥ 5 days 2. Eyes: bilateral injection of conjunctiva (NO purulence or crusting) 3. Mouth: strawberry tongue; erythema 4. Cervical LAD. 5. Rash: nonspecific 6. Extremities: red palms/soles, Beau's lines (transverse lines on nail plates) | |
| Kawasaki Disease Beau's lines | |
| Kawasaki Disease Nonspecific exanthem (no vesicles/crusts) Treatment (acute: w/in 10 days of onset) 1. IVIG 2. ASA 80-100mg/kg/day (after fever controlled for 4-5 days) 3. Low dose aspirin 3-5mg/kg/day (continue forever if coronary artery abnormalities) | |
| Erythema Multiforme TARGET or IRIS lesion (concentric zone of color ∆) - preceded by herpes labialis (?): HSV-specific host response - NO prodrome. - ABRUPT & symmetric | |
| Erythema Multiforme TARGET or IRIS lesion (concentric zone of color ∆: central duskiness, crust, or blister) DDX: Urticaria Sx relief: oral antihistamines Recurrent dz: oral acyclovir -NOT steroids | |
| Left = ? Right = ? | Left = Erythema Multiform - fixed (7 days) - NO relief with Epi Right = Urticaria - transient (< 24 hrs) - relief w/ Epi SQ - clear center w/ red border |
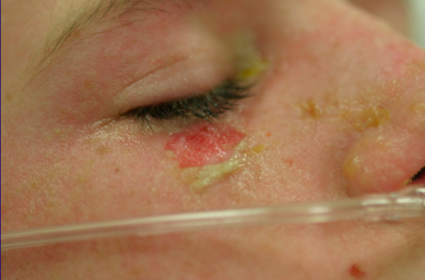
| Stevens Johnson Syndrome Prodrome 1-4 days ≥ 2 mucosal sites (oral / eyes) HEMORRHAGIC crusts Rapid progression to BULLAE & EROSIONS | |
| Stevens Johnson Syndrome Etiology - Drugs: NSAIDs, Sulfonamids, Anti-convul. - Infection: Mycoplasma pneumonia, HSV Tx: supportive care | |
| Stevens Johnson Syndrome Tender red skin w/ dusky discoloration (lesions are targetoid) | |
| Urticaria Acute. Itchy/burning. Clear in center. Transient. Tx: Oral Antihistamine, Epi, Anti-Leukotriene | |
| Urticaria | |
| Urticaria | |
| Angioedema SubQ edema; Deep hives. Large deep swelling with indistinct borders. Eyelids, Lips, Hands. | |
| Dermatographism Physical Urticaria | |
| Heat- and Exercise-Induced Urticaria (Physical Urticaria) Sombrero Lesion: large flare with small central tiny wheal Persistent | |
| Delayed Pressure Urticaria | |
| Salmon Patch (Nevus simplex) "Stork Bite" / "Angel Kisses" CAPILLARY Malformation Most common Face: fade over time...EXCEPT @ NECK | |
| Port Wine Stain CAPILLARY Malformation Lacy. Reticulated. Purple. BLANCH. Darker over time. | |
| Port Wine Stain Capillary Malformation Face: hypertrophy, verrucous (warty) after puberty Tx: pulsed-dye laser (PDL) | |
| Sturge-Weber Syndrome Facial Port Wine Stain in V1 Distribution (unilateral OR bilateral PWS) Assoc. with CNS & EYES abnormalities | |
| Sturge-Weber Syndrome Capillary Malformation V1 distribution (PWS) | |
| Klippel-Trenaunay Syndrome Overgrowth of extremity associated with PWS, venous malformation, or mixed malformation. Soft Tissue Hypertrophy. Swelling. | |
| Klippel-Trenaunay Syndrome PWS/Venous/Mixed | |
| Klippel-Trenaunay Syndrome Sometimes assoc. with varicose veins. PWS/Venous/Mixed | |
| Parkes-Weber Syndrome Overgrowth of extremity assoc. with arteriovenous malformation (AVM) Similar to Kippel-Trenaunay, but - higher flow (seen on imaging) - pulsatile (AVM) | |
| Venous Malformation STATIC (grows only with child, since birth) Never regresses | |
| Venous Malformation Can sometimes look like hemangiomas | |
| Arteriovenous Malformations PALPABLE THRILL. Rare. Frequently over-diagnosed. | |
| Microcystic Lymphatic Malformation (lymphangioma circumscriptum) If localized, they look like FROG EGGS. More infiltrative. Difficult to completely excise. | |
| Macrocystic Lymphatic Malformation (cavernous lymphangioma - cystic hygroma) Less infiltrative. More easily excised | |
| Cutis Marmorata Telangiectasia Congenita More common in DOWN Syndrome. Present at birth. Stays fixed (fades over time). UNILATERAL. Atrophy of skin/limb. Mottled | |
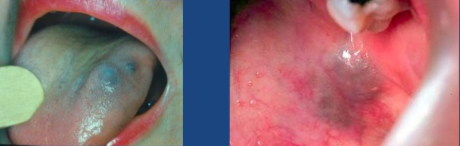
| Hemangioma (pictured: white/blue macule) Tumor of CAPILLARY endothelium. MOST COMMON tumor of infancy Rapid growth phase out of proportion to growth of child. Long period of regression. | |
| Hemangioma | |
| Hemangioma (pictured: telangiectasia) More common if: FEMALE, PREMATURE, CVS, AMNIO | |
| Hemangioma (pictured: red papules) | |
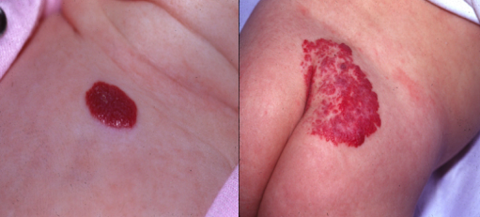
| Hemangioma Pictured: superficial "strawberry" | |
| Hemangioma Pictured: deep Soft compressible RUBBERY bluish nodule under skin. | |
| Hemangioma Pictured: mixed RAPID growth phase: 4-8 wks thru 6-9 m.o. Proliferation (6-12 mo): grows slowly & APPROXIMATES GROWTH of infant Slow INVOLUTION begins: > 12 mo (softer, less warm, flattens out) | |
| Hemangioma BEARD distribution = AIRWAY involvement | |
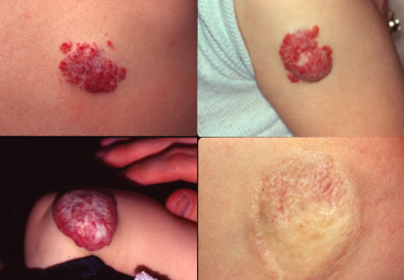
| Hemangiomas (top left = deep | |
| Hemangiomas Worry about cartilage destruction | |
| Ulceration of Hemangioma (complication - others include, bleeding, infection [STAPH AUREUS], obstruction of vital fxn, HIGH OUTPUT CARDIAC FAILURE) | |
| Involution of Hemangioma | |
| Residua of Hemangiomas - Hypopigmentation - Telangiectasia - Fibrofatty deposits - Excess skin | |
| Diffuse Neonatal Hemangiomatosis May have HUNDREDS of lesions < 2 cm May have INTERNAL INVOLVEMENT (e.g. central hypothyroidism | |
| Spider Telangiectasia Red/pink ill-defined macule @ cheeks, nose, posterior hands BLANCH completely w/ pressure (put glass slide over it to make sure) | |
| Spider Telangiectasia Sun-exposed area 2-6 yo kids Fair-skinned individuals Dilation of CENTRAL feeding ARTERIOLE w/ multiple radiating capillaries. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.