2457732
Description
Flashcards by Anna Walker, updated more than 1 year ago
|
|
Created by Anna Walker
about 9 years ago
|
|
| Question | Answer |
| Describe Rinne's test. | This test compares the relative effectiveness of sound transmission through the middle ear by air conduction (AC), and bypassing the middle ear by bone conduction (BC). It is usually performed with a struck tuning fork held 25mm from the canal entrance for 2 seconds. Without delay the base is then firmly pressed against the mastoid for 2 seconds (will probably have to hold patient's head on the other side). Patient is then asked whether they hear it louder at or behind the ear. |
| How do you interpret the results of Rinne's test? | If air conduction is louder than bone conduction, the middle and outer ears are functioning normally (RINNE POSITIVE). If bone conduction is louder than air conduction, there is defective function of the outer or middle ear (RINNE NEGATIVE). Rinne's tells you very little about the cochlea - it is a test of middle ear function. |
| What is a FALSE RINNE NEGATIVE? | A patient with a profound sensorineural deafness may have a false Rinne’s negative. The reason being that with complete loss of innervation to that ear the patient shouldn’t be able to hear anything whether the tuning fork is presented to the canal or to the bone of the mastoid. However, they may hear the sound being transmitted through their skull to their remaining good ear on the other side and they may not be able to recognise which ear they are hearing the sound in. This may give the appearance of bone conduction being better than air conduction when in fact the ear is completely “dead”. |
| Describe the term cross-hearing. | When sound is applied to one ear, the opposite cochlear can be stimulated to varying degrees. This occurs EITHER by escaping sound travelling through air to the opposite ear OR via vibrations through the bone of the skull. Assume we know a patient has a normal ear and a dead ear, audiological tests would result in a better than expected threshold in the dead eaar due to cross-hearing. This is overcome with masking. |
| Describe Weber's test. | This is a test of lateralisation. A struck tuning fork's base is placed somewhere along the midline and the patient is asked if they hear it louder in one ear or if it is the same. The sound will lateralise to: 1. The greater conductive loss. 2. The better cochlea. |
| How do you interpret the results from Weber's test? | Normal or symmetric hearing loss = tone is heard in the midline. Unilateral or asymmetric conductive hearing loss = tone heard in the poorer ear (due to masking effect of background noise in the better ear). Unilateral or symmetric sensorineural hearing loss - tone heard in the better ear. Must be performed with Rinne's - these tests are complementary. |
| What kind of tuning fork result would you expect in a patient with a right sided perforation? | Weber to right. Rinne on right is -ve. Rinne on left is +ve. |
| What kind of tuning fork result would you expect in a patient with a unilateral profound SNHL in the left ear? | Weber to right. Rinne on right is +ve. False Rinne negative on left. |
| What kind of tuning fork result would you expect in a patient with presbyacusis? | Weber's central. Rinne +ve on both sides. This is age-related bilateral SNHL, typically affecting higher frequencies. |
| What are the pitfalls of tuning fork tests? | Only a test to determine the type of hearing loss - not the degree. Results limited to the frequency of the tuning fork used (typically 512 or 1024 - low frequencies to give a longer plateau). Cannot be performed on patients whes loss is too severe to be able to hear the tuning forks. Able to mask non-test ear with tragal rubbing or Barany box, however, tests difficult to interpret and danger of over-masking. |
| What is Pure Tone Audiometry used for? | This is a hearing test that identifies the quietest sound a person can detect. A means of quantifying hearing for diagnostic/rehab purposes. Can gain information concerning the site of a lesion and, in some cases, the nature of the cause. Can give a general indicator of the level of amplification required for hearing aids. Used to monitor hearing levels of those working in noises, patients on ototoxic drugs, and hearing status pre and post surgery. |
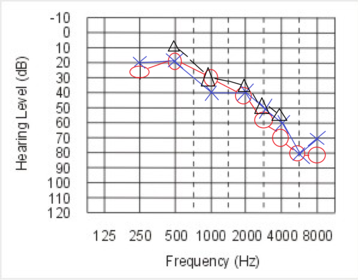
| What symbols are used on an audiogram? | Red for right ear and Blue for left ear. Circle for air conduction in right ear. Cross for air conduction in left ear. Triangle for unmasked bone conduction. Square bracket for masked bone conduction. 'L' shape for uncomfortable loudness levels. |
| What would a normal audiogram look like? | all above 25 dB |
| What is meant by cochlear/retro-cochlear hearing loss? | This is where conditions affect either the cochlea itself or the retro-cochlear pathways; a SNHL occurs. There is no significant separation between the AIR and BONE conduction results on the audiogram |
| What would an audiogram showing SNHL look like? | air and bone conduction both heading down together |
| What happens to the audiogram when there is a conductive hearing loss? | This is where conditions affect the outer and/or middle ear. There is a degree of separation between the AIR and BONE conduction results on the audiogram. Therefore, a big air-bone gap on an audiogram would suggest a conductive hearing loss. If the gap is 10-15 dB, still counted as a sensorineural loss, but if larger than this it is said to be conductive. If bone conduction is then only around 30 dB = mixed loss, as they are both below the 25 dB line. |
| Conductive loss audiogram example. | |
| What is 'masking'? | This is used to prevent cross-hearing. Masking is applied when: Air conduction between ears has a 40dB or more difference. Bone conduction is 10dB or more different to air conduction. It artificially raises the hearing threshold of the non-test ear. |
| What are the frequency limits of bone conduction? | Bone conduction can only be plotted between 500 and 4kHz - after that, the patient feels it as a vibration rather than sound. |
| Which ear should you test first with pure tone? | Test the perceived better ear first. Always accept worst result. |
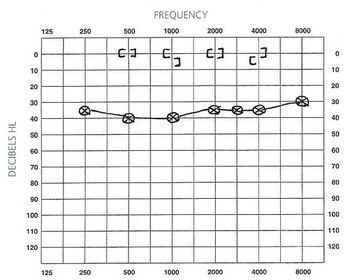
| What is tympanometry? | This is a test of middle ear function. It measures sound admittance into the middle ear, by how much is reflected back. It uses properties of the ear drum to detect problems in the middle ear. Measured over a range of pressures (from negative to positive). For adults a 226Hz tone at 65dB is used. The information is then plotted on a tympanogram. |
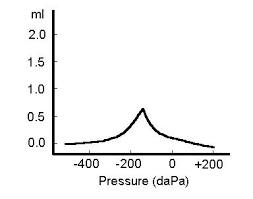
| How should a tympanogram be read? | Gives information on the compliance of the middle ear system, ear canal volume, and middle ear pressure. Maximum compliance of the middle ear system occurs when the pressure in the middle ear cavity is equal to the pressure in the external auditory canal. This compliance (static acoustic admittance) is represented by the highest peak of the curve on the graph. Pressure is indicated on the horizontal axis of the graph, and is measured in decaPascals. |
| Picture of a normal tympanogram (Type A). These indicate a normal middle ear system, free of fluid or physiological anomalies which would prevent the admittance of sound from the middle ear into the cochlea. | |
| What is a type As tympanogram? | Peak is near atmospheric pressure, but is shallow with a reduced peak height. So the middle ear has normal pressure but the curve is shallow because the middle ears contain some fluid or perhaps ossicular fixation (as arising from otosclerosis). |
| PIcture of Type As tympanogram | |
| What is a Type Ad tympanogram? | Normal pressure but deep with a higher peak. Recorded from ears with ossicular disarticulation (perhaps caused by a loud noise or skull fracture), tympanic membrane pathology (such as atrophic scarring) and tympanosclerotic plaques). |
| Picture of a type Ad tympanogram. | |
| What does a Type B tympanogram look like/indicate? | Flat line with no discernible peak. Type B tympanograms occur in ears with middle ear effusion, tympanic membrane perforation, cerumen occlusion, glomus tumour of middle ear or probe tube sealed against the canal wall. The canal volume will differentiate between an effusion or a perforation - if the canal volume is normal - effusion, if it is a large volume - up to 3 ml - it is a perforation. |
| Picture of a Type B tympanogram | |
| What does a Type C tympanogram look like/indicate? | Peaks at a negative pressure (so peak appears towards the left of the tympanogram). This occurs in the presence of negative middle ear pressure as caused by Eustachian tube dysfunction (tube becomes blocked and mucous membrane cells in the middle ear use up O2 - causing a negative pressure. If left untreated this could lead to perforation, or drainage of mucus into the middle ear - glue ear). |
| Picture of a Type C tympanogram. | |
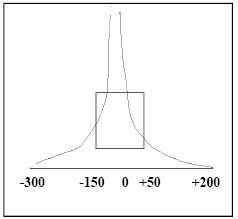
| Give the normative values for ear canal volume, middle ear pressure and gradient. | Ear canal volume: 0.5-1.5ml. Middle ear pressure: +50 to -100 daPa. Gradient: 0.1-1.0ml. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.