5156181
Description
Flashcards by Anna Hogarth, updated more than 1 year ago
|
|
Created by Anna Hogarth
about 8 years ago
|
|
| Question | Answer |
| What is thrombosis? | Pathological process - uses tools normally used for vessel healing. |
| How is the coagulation cascade activated? What is the final product? | 1) Proteolytic activation of a number of enzymes. 2) Fibrin |
| What is fibrin? | Network which stabilises the hemostatic plug - physically stops the bleeding |
| Define thrombosis | Formation of a solid mass from constituents of the blood within the living circulation. Can form in any vessel and the heart. |
| What is the key difference between a blood clot and a thrombus? | Thrombus forms in the living situation. |
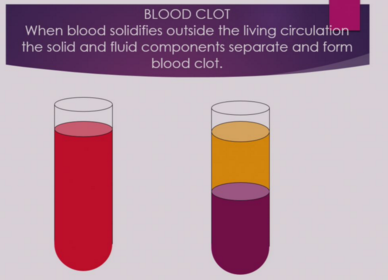
| How can you tell the difference between a blood clot and a thrombus post mortem? | After death blood can separate out - corpuscular part accumulates on vessel. Blood clot is very elastic and very easy to remove. |
| Solid = platelets (fragments of cells) Liquid = Serum and protein content | |
| What is the physiological response to vascular injury? | Hemostasis - hemostatic plug to stop the bleeding |
| What is the key difference between hemostatic plugs and thrombosis? | Thrombosis isn't as finely regulated. |
| What is hemostasis split into? | Primary and secondary |
| What are the stages of primary hemostasis? | 1) Vasoconstriction - reflex neurogenic mechanism + endothelin stimulation 2) Endothelial injury exposes thrombogenic extracellular matrix (ECM) - prothrombotic effect 3) ECM facilitates platelet adherence, activation and aggregation |
| What is the point of the first stage? | Reduce blood flow to the injury site and reduce the size of the injury/hole. Last a very short period of time. |
| What are the stages of secondary hemostasis. | Removal of endothelial layer exposes superficial layer of coagulation factors. 1) Coagulation cascade to produce fibrin 2) Permanent plug |
| What prevents thrombotic effects under normal circumstances? (3) | 1) Endothelial layer prevents coagulation factors being exposed 2) Endothelial cells release t-PA (tissue plasminogen activator) which causes fibrinolysis 3) Thrombomodulin block the coagulation cascade |
| Where do thrombi occur? | Arterial circulation (central to periphery) and venous circulation (periphery to central) |
| What is a key difference between arterial and venous circulation? | Much higher pressure - walls are contracting. |
| How do thrombi in arterial circulation appear? What are they associated with? Capillaries? | 1) Small and pale, composed of platelet and fibrin in arteries with fast flow. Associated with atherosclerosis 2) Tiny, predominantly composed of platelet in capillaries. |
| Where is atherosclerosis commonly found? What does it result from? | 1) Elderly population 2) Progressive damage to vascular wall with accumulation of lipids underneath the endothelium. Predominantly arterial. |
| Describe venous circulation thrombi. | 1) Large and red, fibrin-rich, red blood cell rich in very low-pressure venous system. |
| What are the sites of deep vein thrombosis? What is different about the sites? | Axillary Subclavian Portal Mesenteric Cerebral Pelvic - Increased risk of thrombosis. |
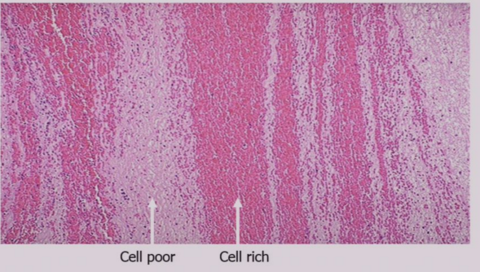
| Describe a thrombus | Cellular and serum phases - striated series of alternating layers of cell poor and cell rich. |
| What are the layers of thrombus called? | Lines of Zahn. |
| 1) Cell poor = fibrin 2) Cell rich = red blood and white cells. | |
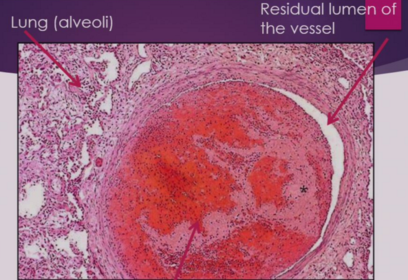
| Lung parenchyma - alveoli, very little space in vessel not occluded by thrombus | |
| What are the components of Virchow's Triad? (ie what are the factors which lead to thrombosis) | 1) Abnormality in/altered vessel wall (endothelial integrity) 2) Abnormal coagulative quality of the blood 3) Abnormal blood flow |
| What happens if you change the vessel wall (increase irregularity) ie reduce smoothness of lining? | 1) Loss of endothelial integrity - increased risk of thrombosis due to atheroma. |
| What is an atheroma? | Degeneration of the walls of arteries caused by the accumulation of fatty deposits and scar tissue leading to restriction of the circulation and a risk of thrombosis. |
| How do you reduce the interaction of platelets with the vessel wall? | Increase regularity of blood flow - more laminar than turbulent. |
| How do changes in blood flow lead to thrombosis? | Disturbances of blood flow allows large numbers of platelets to come into contact with endothelium |
| What are coagulation factors intrinsic to? | The blood itself. |
| How do changes in coagulative qualities of the blood result in increased risk of thrombosis? | Alteration in coagulability of the blood by increasing no. platelets or decreasing serum results in increased dysregulation of coagulation - more intrinsic factors and more platelet interaction with vessel walls. |
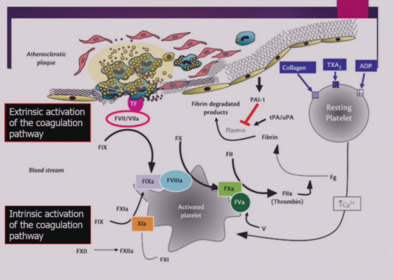
| What are the two coagulation pathways? | 1) Intrinsic - all the enzymes which progressively activate each other are included in the blood 2) Extrinsic - Factors associated with the endothelial |
| What can causes changes in coagulative qualities in the blood? (4) What do they result in? | 1) Genetic 2) Pregnancy (post partum) 3) Surgery 4) Major Injury Increased platelet count - increased coagulation factors - increased risk of thrombosis. |
| How does intact endothelium prevent thrombosis? (4) | 1) Express sulphates mucopolysaccharides (heparin and heparin like molecules) 2) Expressing tissue plasminogen activator (TPA) 3) Synthesizing prostacyclin (PG12) 4) Prevents the exposure of subendothelial ECM and exposure of coagulation factors. |
| What is the role of heparin/heparin like molecule expression? | Disrupt coagulation cascade at various time points. Heparin like molecules degrade thrombin |
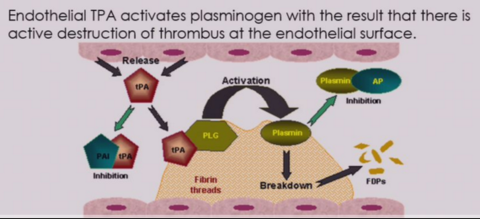
| What is the role of TPA? | Degrades fibrin network |
| What is the role of PGl2? | 1) Vasodilation - Enlarge caliber of vessel making blood flow more laminar 2) Antagonises aggregation of platelets. |
| What do sulphated mucopolysaccharides (heparin and heparin-like molecules) coat and what do they carry? | Coat endothelial cell surface - carry a large negative charge. |
| What do sulphated mucopolysaccharides activate? Give an example. | 1) Antithrombotic enzymes 2) Antithrombin 3 |
| What is the role heparin? What is this trying to achieve? | 1) Activates antithrombin 3 - binds, induces conformational change which results in a hundred fold increase in activity. Degrades thrombin. 2) Prevent formation of fibrin |
| What is the role of TPA? | 1) Converts plasminogen (usually circulating inactivated) into plasmin which destroys thrombus. Removes fibrin if heparin is unsuccessful. |
| X | |
| When do endothelial cells generate PGl2? How is this offset? | 1) When damaged. 2) Platelet produces other prostaglandins with opposing effects. |
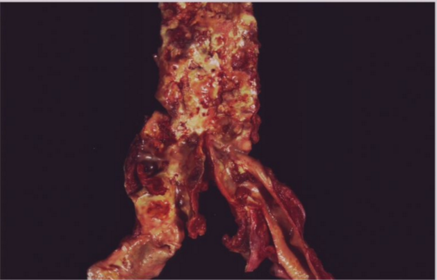
| What is the most common cause of thrombi? | Changes in vessel wall - atherosclerosis |
| Fatty deposits and atheroma - dark red = thrombi stuck to walls. | |
| What does 'changes in blood constituents' refer to? | Increased platelets (increased coagulation factors), increased activity of coagulation factors and fibrin concentration. |
| What are platelets? | Circulating anuclear fragments of cytoplasm of megakaryocytes (largest cell found in the bone marrow, multi-nucleated with large cytoplasm). Each megakaryocytes can produce 2000-4000 platelets |
| What causes platelet concentration to increase? What does this result in? | 1) Injury 2) Increased risk of thrombosis |
| What is the normal concentration of platelets? Abnormal? | 1) 200-400 X 10^9/L 2) 900-1200 X 10^9/L |
| What is the diameter of a platelet? Life span? | 1) 3um 2) 10 day life splan |
| What do platelets contain? | 1) Alpha granules 2) Dense bodies - unique to platelets |
| What do alpha granules contain? (3) | 1) Coagulation factors 2) Platelet derived growth factor (PDGF) 3) Fibrinogen (proto - fibrin) |
| What do dense bodies contain? | 1) Adenine nucleotides (ADP) 2) 5 Hydroxytryptamine (Serotonin) 3) Calcium |
| How does PGl2 interact with platelets? | Prevents them from adhering to vessel walls and releasing granules. |
| What does granule release result in? | Further activation of platelets (conformational change and activation of other downstream factors of the clotting cascade) |
| Describe the steps of platelet activation. (3) | 1) Adhesion: Rapid adherence to collagen exposed by endothelial damage 2) Platelet Release Reaction: Degranulation of platelets 3) Platelet Aggregation: Platelets rapidly clump together to cover the area of endothelial cell loss - change shape to fit the hole better. |
| What mediates platelet aggregation? | ADP and Ca2+ |
| What do platelets generate which opposes PGl2? | Thromboxane (TXA2) - constricts vessels and aggregates platelets. |
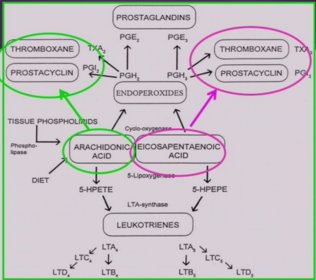
| What do prostaglandin and thromboxane derive from? What enzyme is used to produce them? | 1) Arachidonic acid and eicosapentaenoic acid 2) Cyclo-oxygenase |
| What are the products from arachidonic acid? Eicosapentaenoic acid? | 1) PGl2 and TXA2 2) TXA3 and PGl3 |
| What is the key difference between the products of arachidonic acid and eicosapentaenoic acid? | TXA3 (Thromboxane 3) has little or no pro-thrombotic effect compared to TXA2 - TXA3 decreases risk of thrombosis. PGl3 still has much as an effect as PGl2 |
| X | |
| What diet can decrease risk of thrombosis? | Diet which increases EPE (Eicosapentaenoic acid). Oily fish and primrose oil have anti-thrombotic effect by increase the proportion of TXA3 to TXA2. |
| What is the second part of virchow's triad? | Coagulative qualities of blood |
| What does increasing the coagulation factors result in? What are the two coagulation pathways? | Sequential activation of the clotting factors leading to enormous amplification of the initial signal. Extrinsic and in |
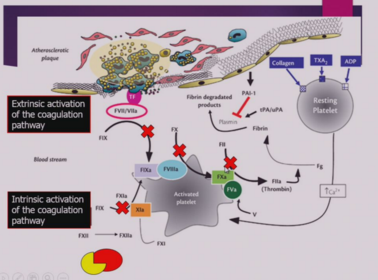
| What is the control factor for coagulation? | Anticoagulation - enhances the action of antithrombin 3 by adding heparin. Also reduces number of coagulation factors. |
| Two pathways - both result in fibrin, interlink. Result from factors released by damaged endothelium or from platelet cells themselves. | |
| What are the different ways of preventing fibrin formation? | 1) tPA converts plasminogen to plasmin to degrade fibrin 2) Antithrombin factors/heparin prevent the conversion of thrombin at many levels. |
| X | |
| What is the genetic abnormality which results in a factor which is more resistant to degradation? | Factor V (Leiden factor) - 2-15% of caucasians have genetic heterozygous factor which means their coagulation is more resistant to degradation by protein C. Harder to degrade this factor. |
| What are the risks associated with this abnormality? | 1) Heterozygous - slight increase of thrombosis risk (roughly 5 fold). 2) Homozygous - 50X higher risk |
| What number of people who involved in a thrombotic event had a factor V abnormality? | 50% |
| What other disorder can result in an increased thrombotic risk? Where is it prevelant? | Homocystinuria - cystathionine beta synthase (CBS) deficiency. Inherited disorder of the metabolism of the amino acid methionine. South Eastern population. |
| How can you decrease the risk of thrombosis after surgery? | 1) Mobilisation of patient soon after surgery 2) Treat with heparin |
| Why do you see turbulence in blood? | 1) Vessel changes in size 2) Bifurcate to a different angle 3) Blood is a complex fluid |
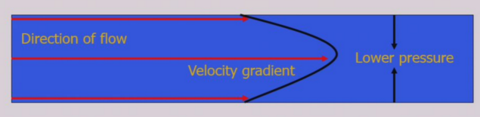
| Describe laminar flow | 1) Minimal mixing between layers 2) Cellular component of the blood moves in the fast flowing lower pressure zone in the centre of the vessel - platelets have less contact with endothelium |
| X | |
| What does turbulent flow result in? What is likely to cause an increase in turbulent flow? | 1) Increased platelet contact with vessel wall 2) Atherosclerosis (vessel damage), specific anatomical locations (sites of bifurcation) are more likely to have turbulent flow and platelet-vessel interaction. |
| What are the most common arterial sites of thrombosis? What are the risk factors particularly in the arteries? | 1) Atheromatous plaque - coronary arteries and aorta 2) Endocardium - mural thrombus. Atherosclerosis and vasculitis |
| Why do (mural) thrombi form in the heart? | Generally turbulent flow but mural thrombi also form following myocardial infarction, infection (endocarditis) and malformation. |
| Where do thrombi in the venous circulation form? | 1) Deep veins the leg 2) Pelvic veins Can occur in surface varicose veins but have less of a systemic/dangerous effect |
| What is one of the secondary dangerous things which result from a thrombus? | Embolism |
| What are the possible events following a thrombus? | 1) Dissolve - physiological factors work in the first few hours (only) to clear thrombus 2) Occlusion of vessel - can damage downstream tissue depending on location 3) Keeps growing in direction of heart 4) Embolism - fragments of thrombus breaks off |
| What are the differences in arterial and venous thrombi? | 1) Arterial thrombi move to periphery ie the brain, limbs etc 2) Venous thrombi move from the periphery to the centre can occlude lungs and heart. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.