7187207
Description
Flashcards by Liam Musselbrook, updated more than 1 year ago
|
|
Created by Liam Musselbrook
over 7 years ago
|
|
| Question | Answer |
| What is the difference between subjective and objective tinnitus? | Subjective: perception of sound in the absence of an acoustic stimulus, only heard by patient Objective: noise generated by structures near the ear, can sometimes be heard by examiner, uncommon |
| What are the causes of subjective tinnitus? | Disrupted auditory pathway -> abnormal neuronal activity in the auditory cortex Aucoustic trauma, Presbycusis Ototoxic drugs Meniere's disease Infections and CNS lesions Sometimes causes of conductive hearing loss |
| What are the causes of objective tinnitus? | Turbulent flow of blood through Vascular middle ear tumour Dural arteriovenous malformations Muscle spasms/myoclonus of palatal or middle ear muscles |
| Otitis media with effusion (OME/'glue ear'): what is it? | Sterile collection of fluid in middle ear Results in conductive hearing loss and flat tympanogram May follow an URTI and resolve spontaneously in a few weeks Most common in children |
| Treatment of OME | Re-evaluate child at 3 months If glue still present grommets are inserted Grommets last on average 9 months Adenoidectomy reduces risk, not usually performed at 1st grommet insertion |
| Acute Suppurative Otitis Media | Bacterial infection of middle ear Pus formation Painful outward bulging of eardrum Rutures and pus drains out of ear, eardrum heals within 4-5 days |
| Treatment of Acute Suppurative Otitis Media | 1st line: Co-amoxiclav Myringotomy is required if failure to resolve or if facial nerve palsy/other neuro-otological complications develop |
| What is a cholesteatoma? | Pouch formed in tympanic membrane filled with keratinising squamous epithelium. Gets infected with anaerobic bacteria and produce enzymes which can erode through local structures |
| Clinical features of cholesteatoma | Main features = foul smelling discharge and hearing loss Other features are determined by local invasion: - vertigo - facial nerve palsy - cerebellopontine angle syndrome |
| What can a cholesteatoma erode through and what are the results from this? | Ossicles - conductive deafness Lateral semicircular canal - vertigo Facial nerve - facial palsy Cochlea - sensorineural deafness Tegmen - intracranial abscess or sepsis Sigmoid sinus - thrombosis |
| What is tympanosclerosis? | Calcification of collagenous scar tissue on tympanic membrane |
| What is otosclerosis? | Familial condition Spongy bone formation around the oval window - as it grows it fuses with the stapes -> conductive deafness Treat by replacing stapes with prosthesis or hearing aid |
| Management of Chronic Suppurative Otitis Media | Confined to middle ear - myringoplasty Involvement of mastoid - cortical mastoidectomy + myringoplasty |
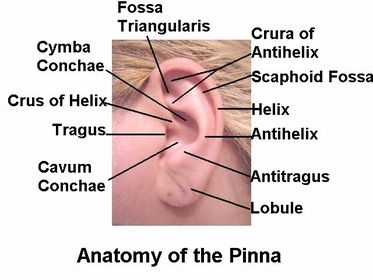
| Pinna anatomy | |
| Noise-induced hearing loss | Temporary threshold shift - cochlear fatigue, reversible hearing loss within 2hrs of exposure Further exposure -> permanent shift Usually notch at 4Khz, 6Khz |
| What is obscure auditory dysfunction? | Difficulty in understanding speech in the presence of noise, with clinically normal hearing thresholds and the absence of any obvious cause |
| How can Menieres disease present? | Triad of: 1)Fluctuating and progressive sensorineural hearing loss 2) Tinnitus (louder in affected ear) 3) Recurrent vertigo (15mins-24hrs) Horizontal nystagmus, N+V |
| Management of Meniere's disease | Inv: Pure tone audiometry + MRI Acute phase: Bucastem and rest Prophylaxis: Salt restriction and bendroflumethiazide Surgery: chemical neurectomy, vestibular nerve section, labyrinthectomy |
| Presbyacusis | Sensorineural, progressive, high frequency hearing loss due to ageing Wear and tear on outer hair cells Usually bilateral and symmetrical Removes consonants from heard speech -> non-intelligible |
| What is an acoustic neuroma and how can it initially present? | Vestibular schwannoma Benign NF2 is a risk factor Unexplained unilateral hearing loss and tinnitus, and vestibular (disequilibrium) symptoms |
| Management of acoustic neuroma | Early as possible referral and treatment Inv: Pure tone audiometry and MRI/CT T: Gamma knife radiosurgery |
| What are the 3 types of otitis externa? | Diffuse Furuncle Malignant |
| Features suggestive of severe inflammation in otitis externa | - Red, oedematous ear canal which is narrowed and obscured by debris - Conductive hearing loss - Discharge - Regional lymphadenopathy - Cellulitis spreading beyond the ear fever |
| Diffuse Otitis Externa | Generalized inflammation of ear canal Symptoms: pruritis, otalgia, swelling, otorrhoea, deafness (occlusion) Generalized (eczema, psoriasis) or localized (trauma) |
| Infective causes of Otitis Externa | Bacterial: Pseudomonas (secondary colonisation), Staph aureus Fungal: Candida, Aspergillus Viral: Herpes zoster |
| Management of mild otitis externa | (mild cases = mild discomfort and/or pruritus; no deafness or discharge) Topical acetic acid 2% spray |
| Management of more severe otitis externa | 7 days of a topical antibiotic with or without a topical steroid |
| Furuncle | Infection of hair follicle of the outer 1/3 of the the EAM Usually Staph. Red swelling from one aspect of the outer wall |
| Malignant Otitis Externa | Aggressive Pseudomonas aeruginosa More common in diabetics or immunocompromised Spreads to the bone ->osteitis -> pain and VII, IX, X and XI cranial nerve palsies High dose IV antibiotics |
| Chondrodermatitis Nodularis Helicis (CNH) | Painful, inflamed nodule of the ear, involving the cartilage and skin of the pinna Usually apex of helix |
| Management of CNH | Biopsy to exclude carcinoma Conservative - reduce pressure on lesion Topical nitroglycerin and steroids, Cryotherapy Surgery |
| What is Ramsey-Hunt syndrome? | Condition where reactivation of pre-existing Varicella Zoster virus occurs in the geniculate ganglion |
| How can Ramsey-Hunt syndrome present? | Auricular pain is often the first feature Facial nerve palsy Vesicular rash around the ear Other features include vertigo and tinnitus |
| Management of Ramsey-Hunt syndrome? | Oral aciclovir and corticosteroids |
| Above what value on an audiogram is considered 'normal'? | 20dB |
| Cause of referred otalgia | Due to one of five neural pathways (cranial nerve V, cranial nerve VII, cranial nerve IX, cranial nerve X, and via the second and third spinal segments, C2 and C3). |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.