7479629
Description
Flashcards by Becca Schmeidler, updated more than 1 year ago
|
|
Created by Becca Schmeidler
over 7 years ago
|
|
| Question | Answer |
| Describe the three major functions of the cardiovascular system, and give 2-3 examples of each | 1. Distribution -Oxygen, Wastes, Hormones 2. Regulation -Heat, pH, Fluid Volume 3. Protection -Protection of blood loss, Protection of infection |
| Describe the components of the cardiovascular system, including the difference between the types of blood vessels. | 1. Blood Vessels -Arteries: take oxygenated blood away from the heart TOWARD the tissues -Capillaries: smaller tubes that take blood into the tissues -Veins: take deoxygenated blood AWAY from the tissues and toward the heart 2. Heart |
| List the four major components of blood, and what percent of each you would expect to see following centrifugation of whole blood. | 1. Red Blood Cells (Erythrocytes) 45% 2. White Blood Cells (Leukocytes) <1% 3. Platelets (Thrombocytes) <1% 4. Plasma 55% |
| Describe how a person’s hematocrit is determined, what information it gives, normal hematocrit levels, and what a low hematocrit or high hematocrit might indicate. Describe the effect of blood doping on hematocrit levels, and why this is dangerous. | Hematocrit: the % of erythrocytes in a blood sample, found by centrifugation (separation by density) Ex. 25% would be 25 mL of erythrocytes in 100 mL of blood Low Hematocrit (<~35%) : anemia High Hematocrit (>~65%) usually due to dehydration: polycythemia --BLOOD DOPING--(adding more RBCs) is dangerous because it increases hematocrit levels, thus increasing the blood viscosity, making blood into a thick sludge. This sludge can cause clotting, stroke, and heart failure. |
| Describe the color of blood in different conditions (+/- oxygen). | high oxygen, low carbon dioxide: scarlet low oxygen, high carbon dioxide: dark red |
| Describe the components of blood plasma and their functions. | -90% water -6-8% proteins: -Albumin: carrier to shuttle molecules (maintains osmotic pressure of blood) -Globulins: Carrier proteins produced by liver/ immune system -Fibrinogen: clotting protein -Organic Nutrients -Electrolytes |
| Describe what is occurring during edema. | In edema, liver cirrhosis leads to low levels of albumin. Low levels of albumin result in water staying in the interstitial spaces, causing swelling |
| Describe the shape of erythrocytes, why the shape is important for their function, and what protein is responsible for maintaining their shape. | Erythrocytes are biconcave discs. This shape is important to their function because it allows them to be flexible and increases surface area when moving through thin capillaries. Spectrin is the protein responsible for maintaining their shape |
| How many erythrocytes are in the human body? | Adults have 20-30 trillion erythrocytes in their bodies |
| Describe the cell structure of erythrocytes – what is in erythrocytes? What is not in erythrocytes? What does these mean for erythrocyte function? | Erythrocytes HAVE: Hemoglobin! (iron containing proteins) Erythrocytes DO NOT HAVE: mitochondria (anaerobic, can't produce proteins), ER or Golgi (can't produce proteins) Amount of hemoglobin leaves no room for organelles, but allows the cell to carry 4 oxygen molecules! |
| Describe the breakdown of erythrocytes (specifically, hemoglobin) and what can occur (especially in infants) if this doesn’t occur as it should, and how this would be treated. | Hemoglobin is broken down into bilirubin in the liver, and then sent to the small intestine. Bacteria in the small intestine break down bilirubin into urobilin, send the urobilin back to the blood, where it is then cleared by the kidneys (giving urine its yellow color) Excess bilirubin occurs in because the baby's liver isn't mature enough to breakdown and remove the bilirubin from the bloodstream. Phototherapy uses light (not UV light) to increase the breakdown of bilirubin. |
| Describe the structure of hemoglobin. | Heme is an iron containing molecule. Globin is a protein that has 4 subunits (2 alpha, and 2 beta). Oxygen is unloaded from the cells in the tissues, and loaded back to the cells in the lungs. Each hemoglobin molecule can carry 4 oxygen molecules. |
| What is the normal amount (g/L) of hemoglobin in an adult male? Adult female? Newborn? | Adult male: 120-160 g/L Adult female: 110-150 g/L Newborn: >200 g/L |
| What type of hemoglobin is found in veins? Arteries? | Veins contain deoxyhemoglobin Arteries contain oxyhemoglobin |
| Why is blood red? | Blood is red due to iron and oxygen combining in the blood cells |
| Describe the condition of sickle cell anemia, and the standard treatment. | Under low oxygen conditions, hemoglobin chains link together, forming stiff rods that deform the erythrocyte. Blood transfusion is the standard treatment. |
| List the five types of leukocytes in order from most abundant to least abundant. | Neutrophils 65% Never Lymphocytes 25% Let Monocytes 6% Monkeys Eosinophils 3% Eat Basophils 1% Bananas |
| Describe the main function of leukocytes, and the three steps most leukocytes take to perform this function. | Main function: protection against foreign invaders 3 Steps: 1) Diapedisis: Leukocytes pass through capillary wall into interstitial space 2) Chemotaxis: Leukocytes move toward a chemical stimulus (i.e. bacteria, toxin) 3) Phagocytosis: Leukocytes engulf exotic or extraneous material, and use an intracellular enzyme to digest them. |
| Describe the identifying structures of granulocytes, and of the three types of granulocytes. | Granulocytes have granules in their cytoplasm, lobed nuclei, and are phagocytes. 1) Neutrophils: Neutral stained cytoplasm 2) Eosinophils: granules stain auburn with eosin stain 3) Basophil: stain blue with basic dyes ("base loving" basic dye binds to acidic molecules |
| Describe the structure and function of neutrophils, and the processes the neutrophils use to perform this function. | Structure: Granules are very fine (difficult to see), Nucleus has 3-5 lobes Function: attack bacteria (increase in response to infection) Granules contain defensins (antimicrobial proteins) that poke holes in a pathogen membrane. Chromosomes (DNA) in the nuclei can be expelled, forming neutrophil extracellular traps (NETs) that capture bacteria and then pull them in through phagocytosis. |
| Describe the structural difference between a neutrophil from a female and a neutrophil from a male. | Females have a "drumstick" on their nucleus. This is called the Barr Body and is actually just the X chromosome extending out of the nucleus. The males do not have this. |
| Describe the structure and function of eosinophils, and the process(es) the eosinophils use to perform this function. | Structure: Granules stain auburn, contain digestive enzymes but do not digest bacteria. Nucleus has two lobes. Function: Attack parasitic worms. The eosinophils release enzymes onto the parasite's surface, digesting it away. |
| Describe the structure and function of basophils, and the process(es) the basophils use to perform this function. | Structure: Granules stain blue, Mature nucleus has 2-3 lobes. Function: Respond to allergens. Granules contain histamine, which is an inflammatory chemical which acts as a vasodilator and attracts other white blood cells to the inflamed site. It increases mucous production to try to rid the body of the foreign substance. |
| Describe how antihistamines act to relieve allergy symptoms, and why some make you feel tired. | They block the actions of histamines (by competitively binding to their receptors), and therefore prevent many of the symptoms associated with allergies. In the brain, histamines play a role in regulating sleep, so some antihistamines can cause drowsiness. |
| Describe the structure and function of monocytes. | Structure: Agranulocytes (no granules in their cytoplasm), Kidney shaped nucleus, Largest of the leukocytes, Activate lymphocytes (immune response) Function: Convert into macrophages when they leave the bloodstream. They "eat" viruses and bacteria, they're bigger than granulocytes and have more capacity. |
| Describe the structure, function, and types of lymphocytes. | Structure: Agranulocytes, Large, spherical nucleus, only a few in the blood, most are found in the lymphoid tissues Function: recognize and destroy intruders 2 Types: B Cells (convert into plasma cells which produce antibodies) and T Cells (destroy cells that have been taken over by an intruder) |
| Where does hematopoiesis occur? What is the common precursor of granulocytes? Lymphocytes? | Hematopoiesis occurs in the red bone marrow; The common precursor of granulocytes are stem cells, but they originate from myeloblasts. Lymphocytes originate from a lymphoid progenitor. |
| Describe what occurs in the blood in leukemia, and describe the difference between myeloid and lymphocytic leukemia, and acute and chronic leukemia. What would a blood smear from a person with leukemia look like? | Blood leukemia is the overproduction of abnormal, nonfunctional leukocytes. Myeloid leukemia: abnormal leukocytes are myeloblast descendants (granulocytes) Lymphocytic leukemia: abnormal leukocytes are lymphoid descendants (lymphocytes). Acute: Quickly advancing Chronic: Slowly advancing A blood smear from a person with leukemia has a large amount of leukocytes present |
| Describe what occurs in the blood in mononucleosis. What would a blood smear from a person with mononucleosis look like? | Caused by a virus (Epstein-Barr virus). Increase in agranulocytes (monocytes and lymphocytes; "one nucleus"), most of which are atypical. A blood smear would have an increased amount of large-nucleus leukocytes. |
| Describe the formation of platelets. Where in the body does this occur? | Platelets are not cells, they are fragments of giant cells (megakaryoblasts) from the bone marrow. They are involved in hemostasis. |
| Describe the three steps of hemostasis. Explain the role of clotting factors and vitamin K. Why do babies get a shot of vitamin K after birth? | 1) Vascular Spasm: smooth muscle contracts, causing vasoconstriction 2) Platelet Plug Formation: Injury to lining of vessel exposes collagen fibers; platelets adhere; Platelets release chemicals that make nearby platelets sticky; platelet plug forms 3) Coagulation: Fibrin forms a mesh that traps red blood cells and platelets, forming the clot. Clotting factors are important because they lead to fibrin formation-Calcium and Vitamin K are necessary! Babies get a shot of vitamin K after birth because they are not able to produce much of their own vitamin K |
| Describe what occurs during hemophilia, and what treatment is used. | This is loss of one of the clotting factors, so clotting does not occur. Bleeding into the tissues can occur. Treatment can include transfusion of plasma or of the appropriate clotting factor |
| Describe the process of clot retraction, what proteins are involved, and why it is necessary. | It occurs after hemostasis, and further stabilizes the clot. Contractile proteins (actin and myosin) in platelets contract and pull the ruptured edges of the blood vessel together, and reduces clot size. |
| Describe the process of fibrinolysis, what proteins are involved, and why it is necessary. | Removal of a clot after healing has occurred (begins ~2 days after the clot is formed). Plasminogen protein is incorporated into the clot. When it gets the signal (tissue plasminogen activator, tPA) that healing has occurred, it activates to become plasmin, which digests the fibrin and breaks down the clot. |
| Which scientist identified the blood groups? | Karl Landsteiner |
| Why does agglutination occur when different blood types are mixed? | Because the different blood types contain different antibodies to foreign antigens. When the antibodies and the antigens are mixed, it can cause the cells to clump together. |
| Describe the different antigens and antibodies found in a person with type A, B, AB, or O blood. | Type A: Antigen-A, Antibody-B Type B: Antigen-B, Antibody-A Type AB: Antigen A, Antigen B, No Antibody Type O: No Antigen, Type A Antibody, Type B Antibody |
| Which blood type is the universal donor? Universal recipient? Why? | Blood Type O is the universal donor, because it has no antigens to be recognized as foreign by the recipient. Blood Type AB is the universal recipient, because it has no antibodies, so it will not try to fight off invaders. |
| How are blood types determined? | We use an antibody-antigen reaction to determine a person's blood type. Ex. If anti-A is added to blood type A, agglutination will occur. If anti-B is added to blood type A, agglutination will not occur, because the same antibody is already present in the blood |
| Describe what occurs during Rh incompatibility in a pregnant mother, and what the treatment is. | If a woman with a negative blood type is impregnated by a man with a positive blood type, the baby can have positive type blood. At birth, some of the baby's blood is transferred to the mother and her body can start to produce an antibody against the Rh antigen. If she was impregnated again by the same man, her blood cells would attack the Rh positive fetus's red blood. To prevent this from happening, RhoGAM, an immune globulin, is injected right after the birth of the first child so that the mother does not develop antibodies to Rh positive blood. |
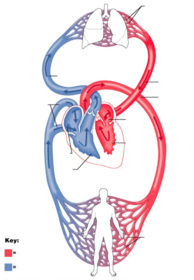
| Be able to Label Figure 16.1 | |
| Contrast the type of blood and the source of blood found in the right half of the heart compared to the left half of the heart. | -Right half: receives deoxygenated blood from tissues, pumps it into the lungs. -Left half: receives oxygenated blood from the lungs, pumps it into the tissues. |
| Describe the location of the heart. | -Extends from the second rib to the fifth intercostal space (~5 inches) -2/3 of mass is to the left of the mid-sternal line -Sits superior to the diaphragm, and deeper than the lungs |
| List the three layers of the heart and explain their function, and, if any of the layers have sublayers, identify those. | 1) Pericardium Three layers: Fibrous pericardium (protects and anchors the heart, prevents the overfilling of the heart with blood), Parietal layer of the serous pericardium, Visceral layer of the serous pericardium 2) Myocardium (muscle) 3) Endocardium (inner endothelial lining) |
| Explain the flow of blood from deoxygenated blood leaving the tissue to oxygenated blood coming back to the tissue. Be able to trace the path of blood through all the vessels and chambers, including any valves that it passes by. | 1. From tissue (deoxygenated) 2. Right atrium (deoxygenated) 3. Right ventricle (deoxygenated) 4. Lungs (deoxygenated->oxygenated) 5. Left atrium (oxygenated) 6. Left ventricle (oxygenated) 7. To tissue (oxygenated) |
| Explain the activity of valves during the cardiac cycle. What about the structure of the valves make them able to act like this? | Step 1: Blood flows into the atria, pushing the AV valves open as it flows into the ventricles. Atria contract to push blood into ventricles. Step 2: Pressure of blood in the ventricles force AV valves closed. Chordae tendineae hold the valves in place. Step 3: As ventricles contract and intraventricular pressure rises, blood is pushed up against semilunar valves, forcing them open. Step 4: As ventricles relax and intraventricular pressure falls, blood flows back from the arteries, filling the cusps of semilunar valves and forcing them to close. The cusp-shaped valves allow them to behave like this. |
| What causes the lub-dub sound of our heart beat? | LUB: Atrioventricular Valves close in S1 DUB: Semilunar Valves close in S2 |
| Why do we need coronary circulation? | Even though the heart is continuously filled with blood, the myocardium is too thick for nutrients to diffuse into it, so it needs its own blood supply |
| Is coronary circulation the same in all people? Explain. | No. For most people, blood is brought to the right atrium/ventricle by the right coronary artery, and to the left atrium/ventricle by the left coronary artery. In 15% of people though, the left coronary artery brings blood to both ventricles. (Right coronary artery still brings blood to right atrium). 4% of people have only one coronary artery that brings blood |
| How is a cardiac muscle fiber similar to a skeletal muscle fiber? How is different? | Similar: They are both striated, and both have sarcomeres (composed of actin and myosin) which are almost identical to those in skeletal muscle. Different: Cardiac muscle cells are short and fat and only have one (at most two) nuclei |
| What about the heart allows it to act as a functional syncytium? How many syncytium are in the heart? | Myocardium behaves as a single coordinated unit. There are actually two syncytium in the heart, the atria and ventricles. This allows the atria to contract slightly before the ventricles. |
| What are the two types of heart cells? | 1. Working (contractile) heart cells- contract and relax (heart pump) 2. Pacemaker cells - generate the impulse (tell the heart to contract) |
| Describe an action potential in working cardiac cells. How is it different than in skeletal muscle cells? | ???? |
| Draw an action potential of the working cardiac cells, and define and describe the four steps. How does it compare to a nerve or skeletal muscle action potential? | ???? |
| Describe what makes cardiac cells in the pacemaker special. | They are self-excitable: they demonstrate the ability to contract without stimulation from the nervous system |
| Draw an action potential of the pacemaker cells. Explain what is occurring in each of the four steps. What makes the action potential self-excitable? | Action potentials are self-excitable when they demonstrate the ability to contract without stimulation from the nervous system |
| Describe the five locations of the pacemaker cells and the function of each. Which location sets the heart rate? Why? | 1) Sinoatrial (SA) Node: Sets the pace of the heart as a whole. This is because cells here reach threshold sooner than other cells, thus causing faster action potentials. 2) Atrioventricular (AV) Node: Depolarization from SA Node travels through gap junctions to the AV Node. 3) Atrioventricular (AV) Bundle: Receives impulse from AV Node and passed it on to the ventricles 4) Right and Left Bundle Branches: Bring signal (depolarization) throughout right and left ventricles 5) Purkinje Fibers: Smaller branches that penetrate into ventricles to further transmit the signal |
| Be able to identify a normal EKG tracing, and label the PQRST peaks/valleys. What is going on at each step (P, QRS, and T)? | P: Atrial Depolarization QRS: Ventricular Depolarization T: Ventricular Repolarization |
| Normal EKG Tracing | |
| Junctional Rhythm | No P Wave, indicating that the SA Node is non-functional. AV Node paces heart (so it is slower, 40-60 beats/minute) |
| Second-Degree Heart Block | Some P waves do not result in a QRS, indicating the signal from the SA Node was not sent to the AV Node. (There are 2 P waves for every 1 QRS=2nd Degree) |
| Ventricular Fibrillation | Chaotic irregular deflections...occurs during acute heart attack and electrical shock. |
| What type of EKG would be performed to identify a possible coronary blockage? | Exercise EKGs done to check for coronary blockage, which can't be identified with normal EKGs. |
| What is the clinical use of electronic pacemakers? When are they used? | They electrically stimulate the heart muscle if the SA or AV nodes aren't working--arrhythmias. |
| Describe STAGE ONE of the cardiac cycle. Include a description of what is occurring in respect to the valves, atria/ventricles/ and blood flow. Also include where the heart sounds are made, what is occurring in an EKG tracing, and how long each step takes. | 1. Ventricular Filling A) All 4 chambers of the heart relaxed (mid to late diastole) B) Pressure in the heart is low, blood is returning to the heart C) There is rapid ventricular filling (80% of ventricular filling occurs), as blood flows passively into the atria through the open AV valves into the ventricles. (aortic and pulmonary valves (semilunar; SL) closed so blood stays in ventricles D) As ventricles fill, AV valves begin to drift toward closed position E) Atriole systole occurs as atria contract (SA Sends signal; P wave of EKG!)- blood is actively pushed into the ventricles (the remainder 20% of ventricular filling occurs now) F) AV node receives and transmits signal from SA node, and ventricle begins to depolarize (QRS complex of EKG!) **LASTS ~0.1 sec** |
| Describe the SECOND STAGE of the cardiac cycle. Include a description of what is occurring in respect to the valves, atria/ventricles/ and blood flow. Also include where the heart sounds are made, what is occurring in an EKG tracing, and how long each step takes. | 2. Ventricular Systole A) As blood fills the ventricles, it forcefully pushes the AV valves closed, causing them to snap shut (the LUB (S1) sound heard in the stethoscope) B) All valves are closed for a split second (isovolumetric contraction phase) C) Ventricles contract (systole) and ventricular pressure increases. This forces the SL valves open, and blood goes into the aorta and pulmonary trunk. **LASTS ~0.3 sec** |
| Describe the THIRD STAGE of the cardiac cycle. Include a description of what is occurring in respect to the valves, atria/ventricles/ and blood flow. Also include where the heart sounds are made, what is occurring in an EKG tracing, and how long each step takes. | 3. Isovolumetric Relaxation (Early Diastole) A) Ventricles relax as repolarization occurs (T wave of EKG) B) All four chambers are relaxed (diastole) C) Because of the loss of ventricular pressure, blood in the aorta and pulmonary valve gets trapped in the semilunar cusps, causing the valves to close (DUB sound, S2) D) All valves are closed for a split second (isovolumetric relaxation phase) E) As ventricles continue to relax, AV valves fall open, and ventricular filling begins. **LASTS ~0.4 sec (QUIESCENT PERIOD)** |
| Be able to look at an image of the heart and describe what stage the heart is in. (Ventricular Filling) | |
| Be able to look at an image of the heart and describe what stage the heart is in. (Ventricular Systole) | |
| Be able to look at an image of the heart and describe what stage the heart is in. (Isovolumetric Contraction Phase) | |
| Be able to look at an image of the heart and describe what stage the heart is in. (Isovolumetric Relaxation Phase: Early Diastole) | |
| Describe the response of the heart to sympathetic nerves and parasympathetic nerves. Include the molecular mechanism behind the responses. (ie, what neurotransmitters are involved and how they act). | Sympathetic Nerves: Increase heart rate and the force of contraction -Norepinephrine released from sympathetic nerves binds to Beta-adrenergic receptor on cells of the SA node, causing: threshold to be reached more quickly & an increase in calcium entry--Both cause the SA node to fire more rapidly. Parasympathetic Nerves: decreases heart rate during the relaxed state (after stressful situation has occurred) -Vagus nerve releases acetylcholine, which hyperpolarizes the membranes of the cells in the SA and AV nodes. This slows the heart rate because it slows down the number of signals the nodes send, which slows the heart rate. |
| Explain how cardiac output is determined. If given heart rate and stroke volume, be able to determine cardiac output. | Cardiac output = heart rate x stroke volume EXAMPLE: Avg. resting HR: 75 beats/min Avg. Stroke Volume: 70 mL/beat CO = 75 x 70 CO = 5250 mL/min CO= 5.25 L/min |
| Explain how stroke volume is determined. If given EDV and ESV, be able to determine stroke volume. Explain the determinants of EDV and ESV (for example, atrial pressure). | Stroke Volume = EDV - ESV -EDV is usually determined by how long the ventricle is relaxed for, and by venous pressure. If either increases, EDV increases. EDV is usually ~120mL -ESV is usually determined by the force of ventricular contraction, and the arterial blood pressure. If the force increases, ESV decreases. If the arterial pressure increases, ESV increases. ESV is usually ~50mL EXAMPLE: SV = 120mL - 50mL SV= 70 mL |
| Describe the four main causes of congestive heart failure. Explain what happens when just the right side of the heart stops working, and what happens when just the left side of the heart stops working. Describe some common treatments of congestive heart failure. | 1) Coronary atherosclerosis: blockage in the coronary arteries so heart doesn't get the blood (nutrients/oxygen) it needs, causing it to pump ineffectively. (Can lead to heart attack) 2) Persistent High Blood Pressure: As pressure in the aorta increases, the ventricular myocardium must exert more force to open the aortic valve. Eventually, the stress takes a toll and the myocardium weakens 3) Multiple Myocardial Infarctions: Scar tissue decreases pumping efficiency 4) Dilated Cardiomyopathy (DCM): Ventricles stretch and thin, and the myocardium deteriorates. -If the right side of the heart stops working, there is peripheral congestion. Blood backs up into your systemic system, you get edema. -If the left side fails, there is pulmonary congestion--right side sends blood to the lungs, but the left side can't send the oxygenated blood to tissues Treatments: Heart transplants or medical remedies to replace damaged heart, angioplasty and stents, bypass surgery, drugs (ex. digitoxin to increase heart contractions) |
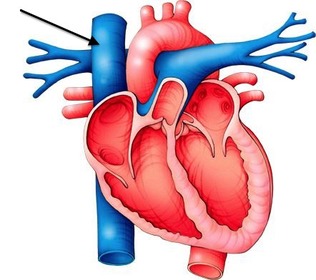
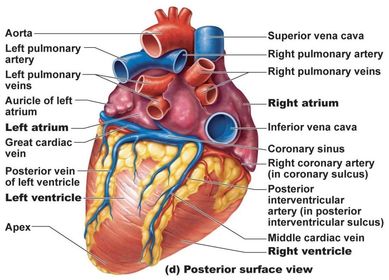
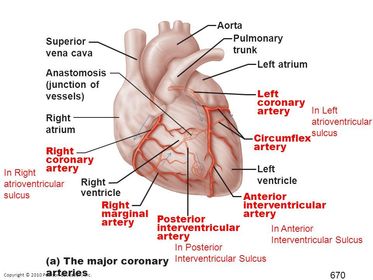
| Superior Vena Cava | |
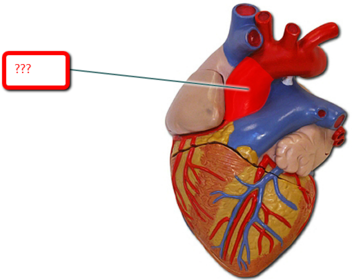
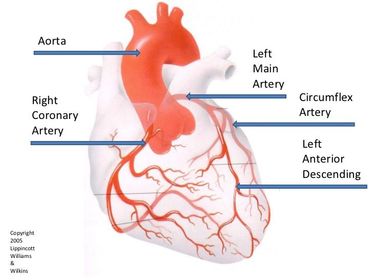
| Aorta | |
| Right Coronary Artery | RIght coronary artery |
| Right Marginal Artery | Right Marginal Artery |
| Posterior Interventricular Artery | Posterior Interventricular Artery |
| Anterior Interventricular Artery | Anterior Interventricular Artery |
| Circumflex Artery | Circumflex Artery |
| Left Coronary Artery | Left Coronary Artery |
| Describe the path of blood through the blood vessels from the heart and back to the heart. | Heart -> Artery -> (diverge) Arteriole -> Capillaries -> Venules (converge) -> Veins -> Heart |
| Describe the three layers of blood vessels. | -Tunica Intima: contains the simple squamous endothelium that line the artery lumen -Tunica Media: circular smooth muscle and elastic fibers -Tunica Externa: collagen fibers |
| Describe the structural difference between veins and arteries. | Arteries: Experience a pressure wave as blood is pumped from the heart (pulse). Because of these pressure waves, arteries need to be thick and robust (so they have a thicker tunica media). They also have a more uniform circular shape -Veins: do not experience pressure waves, so are thinner and more irregular in shape. |
| Describe the three types of arteries, including their structure, function, and where they are found. | 1) Elastic: Thick walled arteries close to the heart (aorta/pulmonary artery) Contain high amount of elastic fibers that allow the artery to stretch when the ventricle ejects blood 2) Muscular: Deliver blood to organs; have thick tunica media; Active in the process of vasodilation/vasoconstriction 3) Arterioles: Smallest; Single layer of smooth muscle cells; diameter determines the amount of blood in the capillary bed |
| Describe how the flow of blood into capillaries can be regulated. | Arteriole Diameter determines the amount of blood in the capillary bed Dilated: Heat escapes across epidermis Constricted: Heat stays in |
| Define arterial pulse, and list three arteries that can be palpated to feel the arterial pulse (“pulse points”). | -When the left ventricle contracts, it causes a pulse wave of blood through the arteries, which expands the arteries -After this expansion, the arteries will contract to push blood into the capillaries -These pulse waves can be palpated at specific sites on the body ("pulse points") EX. Carotid, Brachial, Femoral, Radial |
| Describe the function and structure of capillaries. | Very tiny branches; sometimes one cell forms the entire circumference of the capillary wall; Pericytes stabilize the capillary wall and help control what can enter and exit the capillary; Function is to exchange materials between the blood and the interstitial fluid |
| Describe the three types of capillaries, including their structure, function, and where in the body they might be found. | 1) Continuous Capillaries -most common: found in skin and muscles; is the least permeable type of capillary because the endothelial cells that line the capillary are joined by tight junctions; some areas are missing the tight junctions (intercellular clefts) and they are important for the passage of fluids and small solutes; pinocytotic vesicles shuttle fluids across the capillary wall 2) Fenestrated: Have fenestrations (pores); found at site of active absorption/filtration (intestines, kidney, endocrine gland) 3) Sinusoid: most permeable; lots of fenestrations and few tight junctions; large intercellular clefts; Found in liver, bone marrow, and spleen; Large gaps allow blood cells and bacteria to pass through; macrophages and other phagocytes just sit outside of the capillaries and remove foreign invaders |
| Describe the structure of veins, and describe the importance of venous valves. | Large lumens (interiors) and thinner walls; therefore, they can hold a lot of blood; large lumens allow blood flow with little resistance; more superficial than arteries |
| Describe two conditions that can occur if venous valves don’t work correctly. | If venous valves don't work correctly, you can get varicose veins, or deep vein thrombosis (clots in the deep veins) |
| Define blood pressure and its unit of measurement. | The measurement of the force the blood exerts on the inner walls of the blood vessels; measured in mmHg |
| Describe the difference between systolic blood pressure and diastolic blood pressure. | Systolic: maximum pressure in the arteries (occurs when ventricles are contracted) Diastolic: minimum pressure in the arteries (occurs when ventricles are relaxed) |
| Describe the two main variables in determining blood pressure. Include three sources of resistance that affect blood pressure. | 1) Cardiac Output (CO): the volume of blood pumped out by the heart 2) Peripheral Resistance: the amount of friction the blood encounters as it passes through the vessels 3 sources of resistance: 1) Blood viscosity: thickness of blood 2) Total blood vessel length: longer vessel = greater resistance 3) Blood vessel diameter: greater diameter = lesser resistance |
| Describe how baroreceptors affect blood pressure (and where baroreceptors are found). | Stretch receptors located in the carotid sinuses (dilations in the carotid arteries), in the aorta, and the large arteries in the neck and chest. They respond to increased blood pressure. |
| Describe how chemoreceptors affect blood pressure. | Respond to low blood pressure |
| Describe how hormones affect blood pressure. | 1) Epinephrine/Norepinephrine: Increase CO and promote vasoconstriction 2) Angiotensin II: responds to low blood pressure, kidney releases renin; stimulates vasonconstriction |
| Describe how blood pressure is measured. | -Cuff blocks blood flow -First sound heard as systolic pressure forces the artery open -Artery closes again as heart relaxes (because cuff is still putting some pressure on artery) -Point when diastolic blood pressure is strong enough to keep the artery open |
| Describe how hypertension affects the heart, and how exercise helps prevent hypertension. | -Chronically elevated blood pressure (over 140/90) -Heart must work harder to pump against that increased resistance -90% of people, there is no one specific underlying cause, but lots of risk factors: Heredity, diet, obesity, age, diabetes, stress, smoking Exercise causes the cells that line the blood vessel to release nitric oxide (NO) which dilates the blood vessel |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.