Page 1
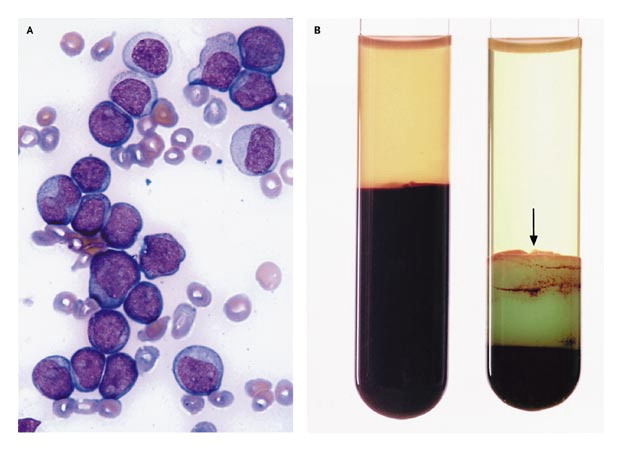
Definition:WBC > 100
{kind=link}
Leukapheresis treatment for extreme cases lots of risks: electrolyte imbalance, hemorrhage, respiratory failure, renal failure, allergic reactionneed to be in ICU setting, pheresis trained nurse, central line, blood bank
INTERVENTIONS-close monitoring-fluids at 1.5-2x maintenance-avoid PRBCs if possible-give platelets, FFP, cryo PRN-treat/monitor tumor lysis-start chemo as soon as possible-leukapheresis
More common in AML & infants
Affects overall prognosis, if symptomatic - higher risk of M&M
{kind=link}
POSSIBLE COMPLICATIONS-neuro: stroke, headache, blindness, decreased LOC-respiratory: hypoxia, dyspnea-hemorrhage-renal failure-tumor lysis syndrome
Result of the rapid destruction of malignant cells in bulky, rapidly proliferating tumors or in highly chemo-sensitive disease
Causes electrolyte imbalances1. Elevated Uric Acid >82. Elevated Phosphorus >2.13. Elevated Potassium >64. Decreased Calcium
{kind=link}
Cell damage = release of nucleic acid (which eventually is converted into uric acid)Rapid release of phosphates as malignant cells have as much as 4x the amount of phosphate compared to normal cellsCan cause precipitation in the renal tubules, which can lead to renal failure
RISK FACTORS-Diagnosis: Burkitt's leukemia & lymphoma, ALL, other lymphomas-Increased LDH-bulky disease-initial WBC >25K-uric acid >8-serum creatnine 1.5x upper normal limit
COMPLICATIONSRenal Insufficiency Cardiac ArrhythmiasSeizures
Clinical Manifestations-Usually occur 12-72 hours after first chemonausea, vomitingdecreased urine outputedema, fluid overloaddysrhythmias congestive heart failurelethargymuscle crampingtetany
Supportive Care for Prevention & Treatment of TLS IV Hydration Baseline lab work; if abnormalities noted or high risk factors, repeat Q4-6 hours Weight monitoring, fluid balance Severe cases may require dialysis
****Best to use GFR or creatinine clearance as an indicator of acute renal failure****
ALLOPURINOL-xanthine oxidase inhibitor-reduces uric acid production-give 10 mg/kg/day divided every 8-24 hours-used in low-moderate risk patients as prevention
RASBURICASE-enzyme found in other mammals but not humans-catabolizes existing uric acid to allantoin (much more soluble)-0.05-0.2 mg/kg for single dose-very expensive
HypErleukocytosis
Tumor lysis syndrome
Want to create your own Notes for free with GoConqr? Learn more.