Page 1
Allergic Rhinitis
{kind=link}
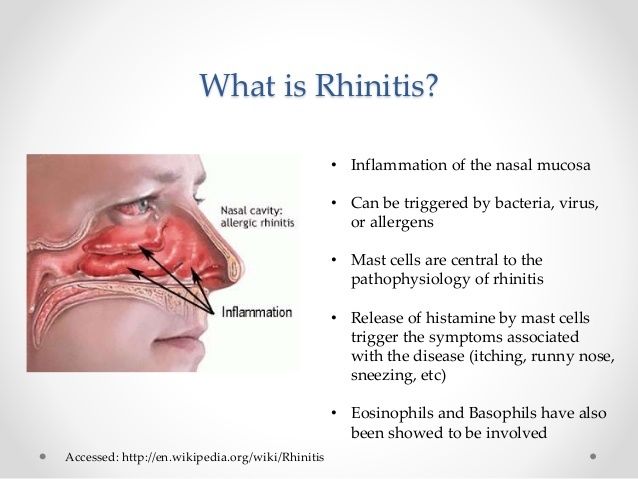
Definition: Allergic rhinitis is inflammation of the nasal mucosa in response to a specific allergen. Signs: Allergic Shinners - Caused by nasal congestion (stuffy nose). Allergic rhinitis can be classified according to the causative allergen (seasonal or perennial) or the frequency of symptoms (episodic, intermittent, or persistent). Episodic refers to symptoms related to sporadic exposure to allergens not typically encountered in the patient's normal environment, such as exposure to animal dander when visiting another person's home. Intermittent means that the symptoms are present less than 4 days a week or less than 4 weeks per year. Persistent means that symptoms are present more than 4 days a week and for more than 4 weeks per year. Seasonal rhinitis usually occurs in the spring and fall, and is caused by allergy to pollens from trees, flowers, grasses, or weeds. The typical attack lasts for several weeks during times when pollen counts are high; then it disappears and recurs at the same time the following year. Perennial rhinitis occurs year round from exposure to environmental allergens, such as animal dander, dust mites, cockroaches, fungi, and molds. Both seasonal and perennial rhinitis can be classified as episodic, intermittent, or persistent, depending on the duration and frequency of symptoms. Clinical Manifestations Manifestations of allergic rhinitis are initially sneezing; watery, itchy eyes and nose; altered sense of smell; and thin, watery nasal discharge that can lead to a more sustained mucus production and nasal congestion. The nasal turbinates appear pale, boggy, and swollen. The turbinates may fill the air space and press against the nasal septum. Patient & Caregiver Teaching Avoiding Allergens in Allergic Rhinitis Include the following instructions when teaching a patient or caregiver about allergic rhinitis. What to AvoidSpecific Approaches House dust • Focus on the bedroom. Remove carpeting. Limit furniture. • Put the pillows, mattress, and springs in airtight vinyl bags or containers. • Limit clothing in the bedroom to items used frequently. Place clothing in airtight, zipper-sealed vinyl clothes bags. • Install an air filter. Close the air conditioning vent into room. Use blinds rather than draperies. House dust mites • Wash bedding in hot water (130o F [54o C]). • Wear a mask when vacuuming. Install a filter on the outlet port of vacuum cleaner. • Avoid sleeping or lying on upholstered furniture. • Keep house temperature and conditions cool and dry. Pet allergens • Remove pets from interior of home. • Clean living area thoroughly. • Do not expect instant relief. Symptoms usually do not improve significantly for 2 months after pet removal. Mold spores • The three Ds that promote growth of mold spores are darkness, dampness, and drafts. • Ventilate closed rooms and open doors. Consider adding windows to dark rooms. Consider keeping a small light on in closets. • Basement light with a timer that provides light several hours a day may decrease mold growth. • Avoid places where humidity is high (e.g., basements, clothes hampers, greenhouses, barns). Dehumidifiers are rarely helpful. Pollens • Stay inside with closed doors and windows during high-pollen season. • Install an air conditioner with a good air filter. Wash filters weekly during high-pollen season. • Put the car air conditioner on “recirculate” when driving. • Avoid having plants, especially in the bedroom. Smoke • Presence of a smoker will sabotage the best of all possible symptom reduction programs. Medications: Corticosteroids - Inhibits inflammatory response of allergic rhinitis. At recommended dose, systemic side effects are unlikely because of low systemic absorption. Systemic effects may occur with higher than recommended doses. Ex.) beclomethasone budesonide (Rhinocort) ciclesonide (Omnaris) flunisolide fluticasone (Flonase) fluticasone furoate (Veramyst) mometasone (Nasonex) triamcinolone Antihistamines • First-generation antihistamines (e.g., chlorpheniramine [Chlor-Trimeton]) can cause drowsiness and sedation. • Warn patients that operating machinery and driving may be dangerous because of the sedative effect. Pseudoephedrine (Sudafed) • Large doses may produce tachycardia and palpitations, especially in patients with cardiac disease. • Overdose in those over 60 years of age may result in central nervous system depression, seizures, and hallucinations. Nursing and Interprofessional Management: Acute Viral Rhinitis Interventions are directed at relieving symptoms. Rest, oral fluids, antipyretics, and analgesics are recommended. Warm salt water gargles, ice chips, lozenges, or sprays may help alleviate a sore throat. Petroleum jelly soothes a raw nose. Saline nasal spray reduces nasal congestion. Antihistamine and decongestant therapy reduces postnasal drip and significantly decreases the severity of cough, nasal obstruction, and nasal discharge. Caution patients to use intranasal decongestant sprays for no more than 3 days to prevent rebound congestion from occurring. Cough suppressants, such as dextromethorphan, and expectorants, such as guaifenesin, may be used. Complications of acute viral rhinitis include pharyngitis, sinusitis, otitis media, tonsillitis, and lung infections. Unless complications are present, antibiotic therapy is not indicated. Antibiotics have no effect on viruses. If symptoms remain for 10 to 14 days with no improvement, an HCP should be consulted. Teach the patient to recognize the manifestations of secondary bacterial infection, such as a temperature higher than 103° F (39.4° C); tender, swollen glands; severe sinus or ear pain; or significantly worsening symptoms. Green, purulent nasal drainage during the later stages of a cold is not uncommon and is not always indicative of bacterial infection. In the patient with pulmonary disease, signs of infection often include a change in consistency, color, or volume of the sputum. Because infection can progress rapidly, teach the patient with chronic respiratory disease to immediately report sputum changes, increased shortness of breath, and chest tightness. During the cold season, advise patients with a chronic illness or a compromised immune system to avoid crowded situations and other individuals who have obvious cold symptoms. Frequent hand washing and avoiding hand-to-face contact can help prevent direct spread.
Page 2
Otitis Media
{kind=link}
Causes: Eustachian tubes are shorter & horizontal, Middle Ear infections You known an infant has an ear ache: Baby pulls on ear. Surgery: Myringotomy with insertion of tympanostomy tubes - Avoid blowing nose for 7-10ays - Tubes fall out in 6 -12 months (1) Acute otitis media is an infection of the tympanum, ossicles, and space of the middle ear. Antibiotics are used if an infection is present. Surgical intervention is generally reserved for the patient who does not respond to medical treatment. A myringotomy involves an incision in the tympanum to release the increased pressure and exudate from the middle ear. (2) Otitis media with effusion is an inflammation of the middle ear with a collection of fluid in the middle ear space. This problem commonly follows upper respiratory tract or chronic sinus infections, barotrauma (caused by pressure change), or otitis media. Complaints include a feeling of fullness of the ear, a “plugged” feeling or popping, and decreased hearing. The patient does not experience pain, fever, or discharge from the ear. It is common to have otitis media with effusion for weeks to months after an episode of acute otitis media. It usually resolves without treatment but may recur. (3) Chronic Otitis Media and Mastoiditis Chronic otitis media is characterized by a purulent exudate and inflammation that can involve the ossicles, auditory tube, and mastoid bone. It is often painless. Hearing loss, nausea, and episodes of dizziness can occur. Culture and sensitivity tests of the drainage are necessary to identify the organisms involved so that appropriate antibiotic therapy can be prescribed. The audiogram may demonstrate a hearing loss as great as 50 to 60 dB if the ossicles have been damaged or separated. Sinus x-rays, MRI, or a CT scan of the temporal bone is done to assess for bone destruction and the presence of a mass. Interprofessional Care Chronic Otitis Media Diagnostic Assessment • History and physical examination • Otoscopic examination • Culture and sensitivity of middle ear drainage • Mastoid x-ray Management • Ear irrigations • Otic, oral, or parenteral antibiotics • Analgesics • Antiemetics • Surgery • Tympanoplasty • Mastoidectomy
Page 3
Tonsilitis [Maternity/Peds]
{kind=link}
{kind=link}
{kind=link}
Page 4
Tonsilitis Cont... [Maternity/Peds]
Assessment: Preoperative Period A complete history is taken, with special attention given to allergy symptoms, difficulty swallowing, or airway obstruction. The child is assessed for signs of active infection (fever, elevated white blood cell [WBC] count) and redness and presence of exudate in the throat. The child should be questioned about the presence of pain in the throat or ears. Because the tonsillar area is so vascular, any bleeding history must be recorded and communicated to the primary physician. Laboratory results (prothrombin time, partial thromboplastin time, platelet count, hemoglobin, hematocrit, urinalysis) are reviewed, and the child should be checked for loose teeth to decrease the risk for aspiration during surgery. A complete current medication list should be reviewed as well. Assessment: Postoperative Period Immediately after surgery, high temp is expected at 101.5 for the first 24hrs. The child should be assessed for bleeding and ability to swallow secretions. Postoperative hemorrhage is a dangerous complication that will need immediate attention. If bleeding occurs, the child is returned to surgery for recauterization. The rate and quality of respirations and breath sounds should be assessed. Vital signs, including blood pressure, should be monitored frequently until discharge. Suction equipment should be available, but do not suction unless there is airway obstruction. The child is assessed for bleeding (frequent swallowing; restlessness; a fast, thready pulse; or vomiting bright red blood). When visually assessing the site for clots or bleeding, use a flashlight for illumination and avoid using a tongue depressor if at all possible. If a tongue depressor is necessary, use a sterile tongue depressor and keep it as far forward in the mouth as possible. Caring for the Child Who Has Had a Tonsillectomy Assessing the child for postoperative bleeding is most important. Because the operative site is not as readily visible as other sites, the nurse needs to look for the following: • Excessive swallowing • Elevated pulse; decreasing blood pressure • Signs of fresh bleeding in the back of the throat • Vomiting bright-red blood • Restlessness that does not seem to be associated with pain No red food should be given, nothing to hot or too cold. Interventions: Postoperative The child should be placed in a prone or side-lying position to facilitate drainage. Although not all clinicians are in agreement, straws and forks may be withheld to prevent trauma to the surgical site. If bleeding occurs, the child is turned to the side and the physician notified. Vomiting of old blood (“coffee grounds” emesis) is common. Antiemetics are given as ordered to decrease throat pain caused by retching. If vomiting occurs, keep the child on NPO status for 30 minutes and then resume clear liquids. Nonaspirin analgesics (e.g., acetaminophen, ibuprofen) are given as ordered. Adequate analgesia increases fluid intake. It is common to prescribe the analgesic every 4 hours (or every three hours if alternating acetaminophen with ibuprofen) for the first 24 hours because throat discomfort is expected. An ice collar can be applied for comfort. Provide clear, cool liquids when the child is fully awake. Avoid citrus drinks, carbonated drinks, and extremely hot or cold liquids because they may irritate the throat. Milk and milk products (puddings, ice cream) can coat the throat, causing a need to clear the throat, and thus, increasing the risk for bleeding. Adequate fluid intake promotes healing and maintains hydration. The nurse teaches the parents the principles of home management and ensures that the child is retaining fluids before discharging the child from the surgical unit. Be sure to tell the parent to monitor the child for postoperative bleeding both within the first 24 hours and again 7 to 10 days after surgery
Page 5
Croup[Maternity/Peds]
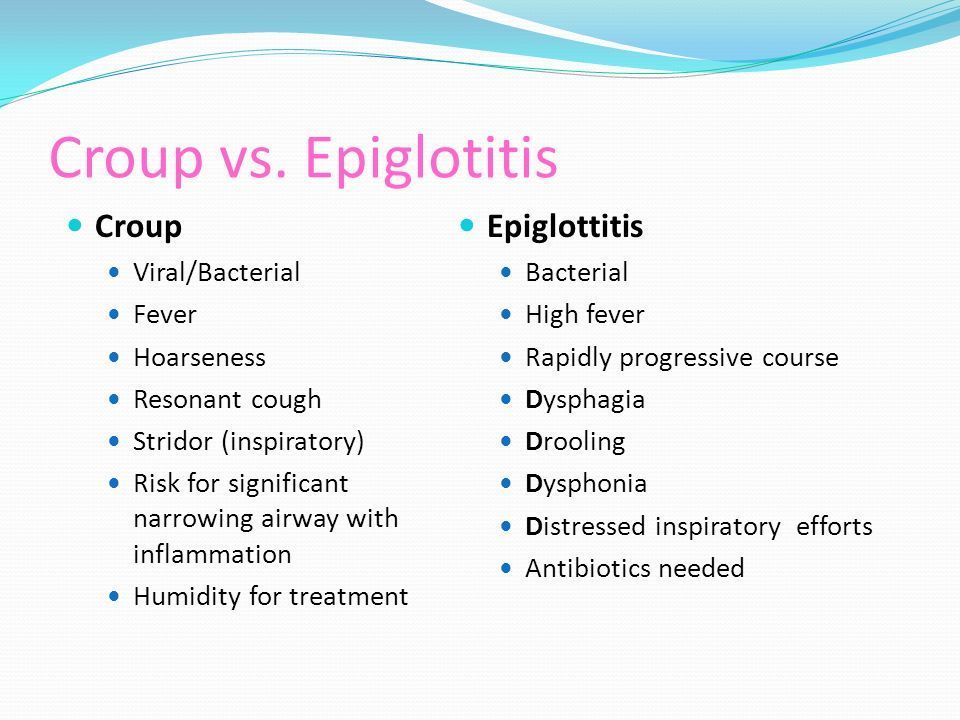
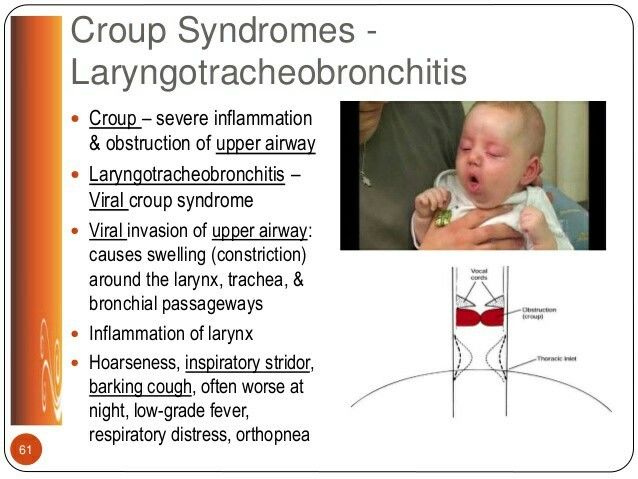
Croup occurs as a result of an upper airway infection. The infection causes swelling around the larynx, trachea, and bronchi. In all forms of croup, mucosal inflammation and edema cause narrowing of the airway Air is usually much drier at night, and as the child lies down, blood flow to the respiratory systems changes. These factors likely explain why symptoms are usually worse during this time and may recur for several nights. Crying aggravates the airway obstruction associated with croup. Retractions and flaring are NEGATIVE. 4L of oxygen maximum by nasal cannula. Drooling indicates being unable to swallow. Croup refers to a group of conditions characterized by inspiratory stridor, a harsh (brassy or croupy) cough, hoarseness, and varying degrees of respiratory distress. Croup is a viral infection of the upper airway. Laryngotracheobronchitis, the most common form of croup, usually affects infants and toddlers; it is one cause of airway obstruction in children ages 6 months to 6 years. In all forms of croup, mucosal inflammation and edema cause narrowing of the airway. This narrowing is more dangerous in infants and young children than in adults because of their small airway diameter and flexible larynx, which is more susceptible to spasm. Symptoms are usually worse at night and better in the day; they may recur for several nights. Croup usually lasts 3 to 4 days. Assessment A nursing history typically reveals a recent upper respiratory tract infection. Assess the child for inspiratory stridor, barking cough, hoarseness, and increased heart and respiratory rates. Record any signs of respiratory distress, such as the use of accessory muscles; substernal, intercostal, and suprasternal retractions; nasal flaring; restlessness and irritability; and pallor or cyanosis. Cyanosis, increased heart rate and respiratory rate, extreme restlessness, or evidence of fatigue or listlessness are signs of hypoxia and should be reported to the physician immediately (Nierengarten, 2015). The lungs should be auscultated for adventitious breath sounds or areas of decreased breath sounds. Temperature and hydration status should also be assessed. Labs A croup score is often used to describe the severity of respiratory distress. Arterial blood gas values or pulse oximetry readings may be monitored to detect decreased PaO2 levels. Manifestations Croup often begins at night and may be preceded by several days of symptoms of upper respiratory tract infection. The child with laryngotracheobronchitis may have a gradual onset and a fever along with other signs and symptoms; occasionally the fever is as high as 40° C (104° F). Children with spasmodic croup do not have a fever. Other manifestations include the following: • The sudden onset of a harsh, metallic barky cough; sore throat; inspiratory stridor; and hoarseness • The use of accessory muscles (substernal, intercostal, suprasternal retractions) to breathe • Frightened appearance • Agitation • Cyanosis Therapeutic Management The goal of treatment is to maintain a patent airway. Children with acute spasmodic croup can usually be cared for at home. Treatment for acute spasmodic croup includes a calm approach and increased oral fluid intake if the child is not in respiratory distress. Taking the child out into the cool, humid night air may relieve mucosal swelling (Roosevelt, 2016). Crying aggravates the airway obstruction. The child should be kept as quiet as possible because crying can aggravate laryngospasm and increase hypoxia. Children who develop stridor at rest, cyanosis, severe agitation, fatigue, moderate to severe retractions, or are unable to take oral fluids should be seen in the emergency department. For mild croup, oral dexamethasone in a single dose of 0.15 to 0.6 mg/kg or inhaled budesonide decreases airway inflammation and reduces the necessity for hospitalization for many children. For children with more severe symptoms (progressively worsening stridor, cyanosis, decreased oxygen saturation, retractions), hospitalization is necessary. Humidified oxygen and intravenous (IV) fluids are given until respiratory distress subsides and the child can take adequate fluids by mouth. Sedatives are contraindicated because they depress respirations and could mask restlessness, an early sign of hypoxia. Medicine Croup symptoms can reoccur after approximately 2 hours, so children who receive epinephrine should be observed in the emergency department for at least 3 hours after treatment and should not be discharged if stridor or retractions are present. Antibiotics are not indicated unless a bacterial infection is present. Acetaminophen is given to reduce fever. Interventions Facilitate airway clearance - The nurse monitors the child's breathing continuously for signs and symptoms of increased respiratory distress (increased respiratory rate, stridor at rest, nasal flaring, retractions, cyanosis, changes in level of consciousness or increased irritability, decreased or adventitious breath sounds, tachypnea). A child with respiratory distress should never be left alone. Fluid Balance - Tachypnea causes insensible water loss, and difficulty swallowing leads to decreased intake. Therefore, the nurse monitors the child's hydration status with intake and output and urine specific gravity measurements. Check mucous membranes, skin turgor, and presence of tears. Weigh the child daily on the same scale and at the same time of day. Offer the child clear, room temperature liquids as tolerated when the child no longer exhibits signs of respiratory distress. Observe the child's ability to swallow because tachypnea and laryngospasm often cause dysphagia. IV fluids are administered in the acute phase of croup because oral fluids are contraindicated in the setting of severe respiratory distress that heightens the risk for aspiration. The child's temperature is taken every 4 hours, and acetaminophen is administered as ordered. Decreasing Fear - Caring for a child in the hospital is exhausting for parents, and fatigue magnifies feelings of anxiety and helplessness. Therefore, provide parents with breaks as needed and assure them that their child will be cared for in their absence. Allow the child to keep a favorite toy or blanket and use developmentally appropriate communication techniques (e.g., play, puppets) when explaining treatments and procedures. Allow the child and parents to ask questions and to discuss fears and concerns, because croup symptoms can be frightening and parents sometimes feel guilty for not having brought the child in for treatment sooner.
Page 6
Epiglottis [Maternity/Peds] - Life Threatening Symptoms
{kind=link}
Epiglottitis is a bacterial form of croup. spasmodic croup may have a genetic predisposition The epiglottis and surrounding structures become inflamed as bacterial infection invades the soft tissue. The epiglottis becomes edematous and cherry red and may become so swollen that it completely covers the glottis and obstructs the airway. Secretions pool in the hypopharynx and larynx. As the disease rapidly progresses, swelling becomes so severe that the child is unable to swallow and begins to drool. The child's voice is muffled, and the throat is very sore. Inspiratory stridor, cough, and irritability are present. Complete airway obstruction can occur rapidly, resulting in hypoxia, acidosis, and death. Treatment Throat and blood specimens are obtained for culture after the child is intubated. Antipyretics are given for fever. Antibiotics are administered IV until the child is extubated. Usually the child improves dramatically after 48 hours of antibiotic therapy and can be extubated at this time. Administration of antibiotic [Amoxicillin] is a priority intervention for a child, and it will be administered by IV route Manifestations The most reliable diagnostic sign of epiglottitis is an edematous, cherry-red epiglottis The onset of epiglottitis is usually sudden and often accompanied by a high fever. The child may have had symptoms of a mild upper respiratory tract infection for a few days before symptoms began. Children with epiglottitis can progress from well-appearing to complete airway obstruction within two to six hours. Unlike croup, epiglottitis has an abrupt onset with rapid progression of symptoms. Often parents report that the child was put to bed well and awakened with a severe sore throat and difficulty swallowing. The child demonstrates a high fever (39° C to 40° C [102.2° F to 104° F]) and appears to be in a toxic condition and very ill. The accompanying sore throat can progress to acute respiratory distress in a few hours. The child appears anxious and frightened and may be irritable or lethargic. One of the classic signs of epiglottitis is that the child insists on sitting upright, often in a tripod position (leaning forward supported on the arms), with the chin thrust out and the mouth open. Respiratory symptoms include nasal flaring; suprasternal, substernal, and intercostal retractions; pale skin color to cyanosis (depending on the degree of airway obstruction); and tachycardia. The epiglottis appears edematous and cherry red. Nursing Considerations The nurse should continuously assess for signs of respiratory distress (stridor, nasal flaring, tachypnea, tachycardia, retractions, drooling, changes in level of consciousness, cyanosis). A sudden decrease in respiratory effort may be a sign of exhaustion and impending respiratory arrest. Arterial blood gas values and pulse oximetry findings are monitored. On pulse oximetry, the oxygen saturation should remain above 95%, with the PaO2 between 80 and 100 mm Hg. Maintenance of a patent airway is essential. The nurse should also keep the child as calm and quiet as possible. If temperature is taken, it 1047should be by the axillary or tympanic route rather than the oral route. The child should be supported in a position of comfort, usually sitting straight up (orthopneic); never force the child to lie down. Children who are anxious and in respiratory distress are often less fearful sitting on their parents' laps. Parents should be encouraged to hug and comfort their child. The parents' anxiety level must be assessed and controlled because their anxiety is easily transferred to the child. Humidified oxygen is delivered in high concentrations. Oxygen therapy is usually less upsetting if the parent holds the oxygen tubing in front of the child's face. All procedures are explained to the parent and child clearly, calmly, and according to the child's level of understanding. Emergency intubation equipment (i.e., oxygen, laryngoscope, endotracheal tube, suction equipment) should be immediately available in case of complete airway obstruction. Worsening of the child's condition should be reported to the physician immediately. Antipyretics are given rectally for fever. Because of the risk for aspiration, the child is kept on NPO status, and fluids are given intravenously. The nurse must closely monitor the ordered IV rate and the urine specific gravity and other indicators of hydration. IV antibiotics are administered as ordered. Cardinal Signs and Symptoms of Epiglottitis Drooling - Indicates being unable to swallow. Child will take on a Tri-pod position. Dysphagia (difficulty swallowing) Dysphonia (difficulty talking) Distressed inspiratory efforts Do not examine or obtain material for culture from a child's throat if epiglottitis is suspected because any stimulation with a tongue depressor or culture swab could trigger complete airway obstruction. Do not leave a child with epiglottitis unattended.
Page 7
Pneumonia
Pneumonia is an inflammation of the lung parenchyma that can occur as a primary or a secondary disease. The two most common types of infectious pneumonia are viral and bacterial. Viruses are the most common causative agents in infants and children younger than 5 years old Interventions For the hospitalized child, elevating the head of the bed and changing the child's position every 2 hours assist respiratory effort and promote pulmonary drainage. Older children may assume a position of comfort but still must change their position every 2 hours. The use of infant seats should be avoided because pressure may be placed on the diaphragm, thus actually decreasing lung expansion. The older child should be assisted with coughing and deep breathing and splinting as necessary to ease discomfort. Oxygen should be humidified and monitored. Pulse oximetry aids in monitoring oxygen saturation and the adequacy of air exchange. A cardiorespiratory monitor is used when available. Oral or IV fluids are given as ordered. IV fluids may be indicated when oral intake increases the stress put on an already compromised body. The nurse monitors intake and output and observes for signs of dehydration (oliguria, poor skin turgor, dry mucous membranes, sunken fontanels, weight loss). Weight should be measured daily. The specific gravity of urine also is checked to monitor hydration status. Because conserving energy aids oxygenation, nursing care is planned to provide for periods of rest. Quiet diversional activities, such as reading, puzzles, videos, and board games, are suggested. The nurse maintains a quiet and cool environment and limits visitors to allow the child maximum rest. Visits by anyone with an infection should be restricted. Administer antipyretics, antibiotics, and analgesics as ordered. Normal breathing may cause discomfort. If an analgesic is not ordered, the physician should be notified of any discomfort the child has. Splinting of the affected side by lying on that side may decrease discomfort. Diversional activities and manipulation of the environment are often effective for pain relief. Assessment Every 2 hours, or more frequently depending on the severity of respiratory distress, assess the child's breath sounds, respiratory rate and rhythm, color, vital signs, and degree of restlessness. Immediately report any signs of increased respiratory distress, including dyspnea, tachypnea, cyanosis, use of accessory muscles of breathing, diminished breath sounds, and crackles. Also note any fever, tachycardia, malaise, anorexia, discomfort, and changes in condition. Nursing Diagnosis and Planning The nursing diagnoses and expected outcomes that may be appropriate for the child with pneumonia and the child's family are as follows: • Ineffective Airway Clearance related to bronchial obstruction. Expected outcome. The child will have clear airways, as evidenced by the absence of abnormal breath sounds and dyspnea. • Ineffective Breathing Pattern related to increased mucus production and pain with inspiration. Expected outcome. The child will demonstrate effective breathing, as evidenced by respiratory rate and rhythm within normal limits for age and absence of retractions. • Impaired Gas Exchange related to increased mucus and accumulation of exudate. Expected outcome. The child will maintain adequate gas exchange, as evidenced by decreased restlessness, appropriate 1051oxygen saturation, and improved mucous membrane and nail bed color. • Deficient Fluid Volume related to fever, decreased intake, and tachypnea. Expected outcome. The child will maintain fluid balance, as evidenced by moist mucous membranes, good skin turgor, urine output appropriate for age, and maintenance of age-appropriate weight. • Deficient Knowledge related to the disease process and home care. Expected outcome. The parents will explain the disease process and describe the child's care. • Anxiety (parental) related to infant's dyspnea and hospitalization. Expected outcome. The parents will show a decrease in anxiety, as evidenced by decreased irritability and increased periods of rest. The parents will verbalize and demonstrate comfort and ease when caring for the child. • Acute Pain related to coughing and difficulty breathing secondary to disease process. Expected outcome. The child will have decreased pain, as evidenced by less irritability, verbalization of increased comfort (if age appropriate), and a relaxed body posture.
Page 8
Apnea [Maternity/Peds]
Apnea is the cessation of breathing for a period of 20 seconds or LESS but accompanied by bradycardia or cyanosis. Heart rate will be normal but respiratory rate and pulse ox will flat line. True apnea differs from periodic breathing, which might be seen in premature infants. In periodic breathing, there is a shift from regular rhythmic breathing to brief episodes of apnea. This type of breathing pattern consists of three or more respiratory pauses of longer than 3 seconds, with less than 20 seconds of respiration between pauses. Rarely, periodic breathing is associated with changes in heart rate or color. Periodic breathing is common in premature infants and decreases as the infant's gestational age increases. The cause is unknown; periodic breathing may be a normal event. Apnea of Prematurity Most common type of apnea; occurs in neonates of 24-32 wk of gestational age, with onset usually within first 1 wk of life. It usually resolves by 37 wk. Although neonate age may be similar to the age at greatest risk for SIDS, apnea of prematurity is not considered to predict risk for SIDS. Infant Apnea Most infant apnea has no known cause. Underlying conditions such as cardiac abnormalities, gastroesophageal reflux, seizures, hypoglycemia, respiratory infection, environmental exposures (e.g., cigarette smoke), or child abuse should be ruled out. Stimulate the infant by touching their back. Assessment The hospitalized infant's heart rate and respirations are monitored continuously. The nurse should ascertain that the alarms on the cardiorespiratory monitor are set to avoid false alarms. Resuscitative equipment should be available. If an apneic episode is observed, the nurse should record the time and duration of the episode, the skin color change, heart rate, and oxygen saturation. The nurse should also describe what the infant was doing before the episode and any actions the nurse took to stimulate breathing. Nursing Diagnosis and Planning The nursing diagnoses and expected outcomes that may be appropriate for the infant with apnea and the family are as follows: • Ineffective Breathing Pattern related to apnea secondary to prematurity of respiratory control mechanisms (premature infant) and related to apnea of known or unknown etiology (term infant). Expected outcome. The infant will have regular breathing patterns, as evidenced by respiratory rate and rhythm within normal limits for age. • Anxiety (parental) related to the possibility of the infant's death. Expected outcome. The parents will verbalize feelings concerning the infant's periods of apnea. • Deficient Knowledge (parental) related to unfamiliarity with apnea monitoring equipment and cardiopulmonary resuscitation (CPR). Expected outcome. The parents will learn how to perform infant CPR and how to operate the apnea monitor. Interventions The nurse sets the heart rate parameters of the cardiorespiratory monitor according to the infant's age and the respiratory pause at greater than 15 seconds. Resuscitative equipment should be available, and the nurse should be proficient in using it. The apneic infant can be stimulated by gently tapping the infant's foot or trunk or turning the infant over. The infant should not be shaken vigorously. If breathing does not resume, institute bag-and-mask ventilation. Maintain a neutral thermal environment while the infant is hospitalized and avoid suctioning if possible. Several studies have shown that feeding affects ventilation. Therefore, infants should be monitored closely when being fed. Home apnea monitoring remains controversial, and there are few clear guidelines related to which infants would benefit most from home monitoring. If home apnea monitoring is ordered, the family should be instructed in the use of the monitor and in CPR before the infant is discharged
Page 9
S.I.D. (Sudden Infant Death Syndrome)(Peds)
Defined as the sudden and unexplained death of an infant younger than 1 year. There is no single cause of S.I.D.S., it is not contagious, hereditary or caused by child abuse. There ARE measures that can be taken to prevent S.I.D.S. Manifestations The principal manifestation of SIDS is silent death. The child may be found in any position and may be clutching bedding. Diagnostic Evaluation Diagnosis is confirmed through autopsy. A medical history of the infant and family should be taken. The infant is examined for signs of illness or trauma. The death scene is also investigated. Nursing Care The Family of the Infant Who Has Died of SIDS Assessment The nursing care involved in a SIDS case is family-centered, not patient-centered. When an infant is brought into the emergency department with suspected SIDS, the family is often confused. If resuscitation was begun at home, they may assume that it was effective and that their infant is alive. Assessment of the family's understanding of the situation is necessary to plan for teaching and support. The nurse should assess the family's emotional status and coping strategies. The nurse interviews the family in a calm, slow, and nonthreatening manner. Questions should not imply negligence or any involvement in the death. Parents need to be given time to think before they answer questions. Because the parents will be overwhelmed, questions may need to be repeated for clarity.
Page 10
Asthma
A condition in which a person's airways become inflamed, narrow and swell, and produce extra mucus, which makes it difficult to breathe. An asthma episode can be triggered by a variety of stimuli, including cold air, smoke, allergens (e.g., pollen, dander, cockroach droppings, dust, mold), viral infection, stress, exercise, odors, and environmental pollutants. Manifestations The manifestations of asthma vary. A child with an asthma episode may have only a dry cough. Wheezing is a classic sign of asthma, but other signs can be present, including shortness of breath, cough, or dyspnea on exertion. Other manifestations may have a sudden or insidious onset: • Retractions, nasal flaring, or stridor • Nonproductive cough (with or without wheezing) that later becomes productive • Tachypnea, orthopnea • Restlessness, apprehension, diaphoresis • Abdominal pain resulting from the strain placed on the abdominal muscles during labored breathing • A hunched-over sitting position with arms braced (tripod position) • Fatigue and difficulty performing simple tasks such as eating, walking, or even talking, because of shortness of breath • A feeling of chest tightness followed by a dry cough, wheezing, and dyspnea • Worsening of symptoms after the child goes to bed at night because of increased narrowing of the airways at night and pooling of secretions Labs Chest radiographs are usually normal except in cases of severe asthma, in which hyperinflation of the airways can be seen. Pulmonary function tests reveal a decreased forced expiratory volume in 1 second, increased residual volume from air trapping, and decreased vital capacity (the maximum amount of air exhaled after a maximum inhalation). Other pulmonary function test results might be altered as well. The peak expiratory flow rate (PEFR) is used to monitor children with chronic asthma. Treatment A bronchodilator, usually a short-acting beta2-adrenergic agonist (SABA) such as albuterol, is administered by a powered nebulizer or metered-dose inhaler (MDI) as often as every 20 minutes for 1 hour or continuously. Oxygen is administered as well. Close monitoring of the child's respiratory status after each course of medication assesses resolution of the episode. Once the child is hospitalized, humidified oxygen is administered at 30%, either by nasal prongs or by facemask, to keep the oxygen saturation at 95% or greater. Increasingly severe asthma that is unresponsive to vigorous treatment measures is termed status asthmaticus. Status asthmaticus is a medical emergency that can cause respiratory failure and death. Hospitalization, usually in an intensive care unit, is indicated. The child is placed on a continuous cardiorespiratory monitor and continuous pulse oximeter. Blood gas and serum electrolyte values are monitored, as is fluid status. In addition to the previously discussed measures, the child may receive continuous nebulized albuterol and ipratropium bromide every 6 hours. If the child's condition does not respond to these medications, oral or IV steroids are then administered. Routine medications. Additional medications are recommended for long-term asthma control: • Inhaled corticosteroids: Beclomethasone, budesonide, fluticasone, flunisolide, and triamcinolone acetonide deliver topical antiinflammatory action directly to the airway. • Long-acting beta2-adrenergic agonists (LABAs): Salmeterol (Serevent) and formoterol (Foradil). • Combination medications: budesonide and formoterol (Symbicort, a combination inhaled corticosteroid and LABA), fluticasone and salmeterol (Advair, a combination inhaled corticosteroid and LABA) • Leukotriene blockers: Montelukast diminishes the mediator action of leukotrienes. Montelukast is available in sprinkles and chewable tablets and can be given to children as young as 1 year old. • Anti-immunoglobulin E (anti-IgE) antibody: Omalizumab (Xolair) for allergic-type moderate to persistent asthma is approved for use in children older than 12 years. It is administered subcutaneously every 2 to 4 weeks. Emergency Asthma Management The following symptoms indicate the need for emergency treatment of asthma: • Worsening wheeze, cough, or shortness of breath • No improvement after bronchodilator use • A peak flow rate that decreases or does not change (even after use of an inhaled beta2-adrenergic agonist) or that is less than 60% of the child's predicted baseline level or personal best • Difficulty breathing (the child's chest and neck are pulled in with each breath, or the child hunches over or struggles to breathe) • Trouble with walking or talking • Discontinuation of play without the ability to resume activity • Listlessness and weak cry in an infant; refusal to suck bottle or breast • Gray or blue lips or fingernails (in which case the child needs emergency treatment immediately!)
Page 11
Cystic Fibrosis [Maternity/Peds]
{kind=link}
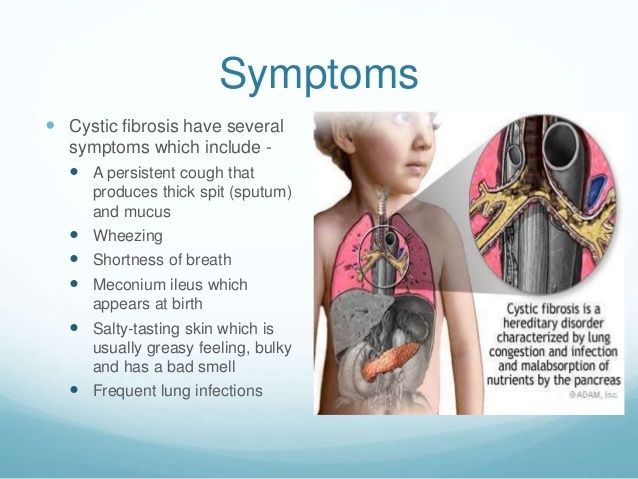
Cystic fibrosis (CF), the most common lethal genetic disease in Whites, is a chronic multisystem disorder affecting the exocrine glands. CF is transmitted as an autosomal recessive trait, which means that both parents must carry the gene for the child to be affected. Cystic fibrosis (CF) affects the exocrine glands throughout the body and causes respiratory, digestive, integumentary, and reproductive dysfunction and damage Signs and symptoms **Clubbing** Include wheezing and a dry, nonproductive cough (earliest pulmonary manifestations), repeated bouts of bronchiolitis, pneumonia and bronchitis, and purulent and copious sputum accompanying chronic bacterial infections. The cough at this stage is wet and paroxysmal and may be followed by vomiting. As the disease progresses, symptoms include crackles, wheezes, diminished breath sounds, accessory muscle use, retractions, hypoxia, and cyanosis. Spontaneous pneumothorax or hemoptysis (blood-stained sputum) is seen in later stages as well. Nasal polyps, sinusitis, digital clubbing and a barrel chest. Blocked by thick mucus, the pancreatic ducts are unable to secrete trypsin, amylase, and lipase into the small intestine. Without these digestive enzymes, proteins, carbohydrates, and fats are poorly absorbed. Digestive system involvement is marked by steatorrhea (frothy, foul-smelling stools two to three times bulkier than normal) and flatus. Malnutrition and growth failure may be evident despite normal caloric intake; deficiencies in the fat-soluble vitamins A, D, E, and K are caused by an inability to absorb fats. Rectal prolapse and intussusception can also occur. Ninety-five percent of males with CF are sterile because of obstruction of the deferent ducts and seminal vesicles. Involvement of the reproductive system is marked by an average 2-year delay in the development of secondary sex characteristics. Females with CF may have difficulty becoming pregnant because of the thick cervical mucus, which acts as a barrier to sperm Respiratory assessment. The child may have had frequent episodes of pneumonia or bronchitis. Auscultate the chest to detect any crackles, wheezes, areas of diminished breath sounds, or a prolonged expiratory phase of respiration. Note signs of long-standing respiratory difficulty, such as barrel chest or digital clubbing. The respiratory status is assessed by noting the rate, depth, and ease of respirations; the color of the nail beds and mucous membranes; and pulse oximetry. The characteristics of the child's cough and the color, amount, and quality of sputum should be documented, along with any fever. Exercise tolerance and the child's ability to sleep lying down at night should also be assessed. Digestive assessment. The nurse weighs and measures the child, plotting the results on a standardized growth chart. Signs of malabsorption (e.g., steatorrhea; loose, bulky stools; protuberant abdomen with thin extremities) should be noted. A diet history is useful in assessing the child's caloric intake. The use of vitamins and dietary supplements should be recorded. Determining the number and consistency of stools assesses the adequacy of intestinal enzyme replacement. Because ulcers and intestinal obstruction often accompany CF, complaints of abdominal pain, blood in the stools, and constipation should be noted. Use of antacids, H2-receptor blockers, or antireflux medications should also be assessed. Reproductive assessment. Girls should be assessed for vaginal itching or drainage, which may indicate a vaginal infection. Contraception should be discussed with affected sexually active adolescents. Nursing Diagnosis and Planning The nursing diagnoses and expected outcomes that often apply to children with CF are as follows: • Ineffective Airway Clearance related to increased pulmonary secretions. Expected outcome. The child will be able to remove secretions from the airway. • Impaired Gas Exchange related to air trapping within the alveoli secondary to obstruction of the airways by thick mucus. Expected outcome. The child will maintain an oxygen saturation level of greater than 95%. • Risk for Infection related to tenacious secretions and altered body defenses. Expected outcome. The child will remain free of infection. • Imbalanced Nutrition: Less Than Body Requirements related to poor intestinal absorption of nutrients. Expected outcome. The child's nutritional status will improve, and the child will exhibit normal growth; the child's stools will be of normal consistency, frequency, and color. • Activity Intolerance related to pulmonary congestion and poor absorption of nutrients. Expected outcome. The child will rest comfortably and will engage in age-appropriate activities. • Situational Low Self-Esteem related to physical changes from chronic illness. Expected outcome. The child will demonstrate a positive self-concept and feelings of independence, as demonstrated by participating in self-care and in age-appropriate activities. • Ineffective Coping (individual) and Compromised Family Coping related to chronic illness. Expected outcome. The child and family will adhere to the treatment regimen, verbalize feelings about the impact of the illness on their lives, and use available support systems and community resources. • Anticipatory Grieving related to a potentially fatal diagnosis. Expected outcome. The child and family will make realistic plans for the future and will be able to discuss feelings about the child's prognosis. Interventions Facilitating airway clearance and gas exchange. Perform CPT two or three times a day and as needed; perform treatments at least 1 hour before or 2 hours after meals to reduce gastrointestinal upset Children with CF are prone to respiratory infection, especially airway colonization with P. aeruginosa, and oral or inhaled antibiotic therapy may be routine. IV antibiotics may be required during acute exacerbations Provide a well-balanced diet that is high in calories, protein, and carbohydrates and includes the child's favorite foods. Oral or enteral high-calorie supplements can increase the child's calorie intake. The child needs to take pancreatic enzymes (which come as enteric-coated capsules containing the enzyme beads) as ordered within 30 minutes of eating all meals and snacks.
Page 12
Laryngotracheobronchitis (LTB) [Maternity/Peds]
The most common type of croup. usually affects infants and toddlers; it is one cause of airway obstruction in children ages 6 months to 6 years. The incidence of croup is higher in boys than in girls, and the disease occurs more often during the winter than in other season Cause: Usually viral but may be bacterial Assessment: Gradual onset, usually at night. Child awakens with harsh cough and inspiratory stridor Ages: 3moth - 3yrs
{kind=link}
{kind=link}
Page 13
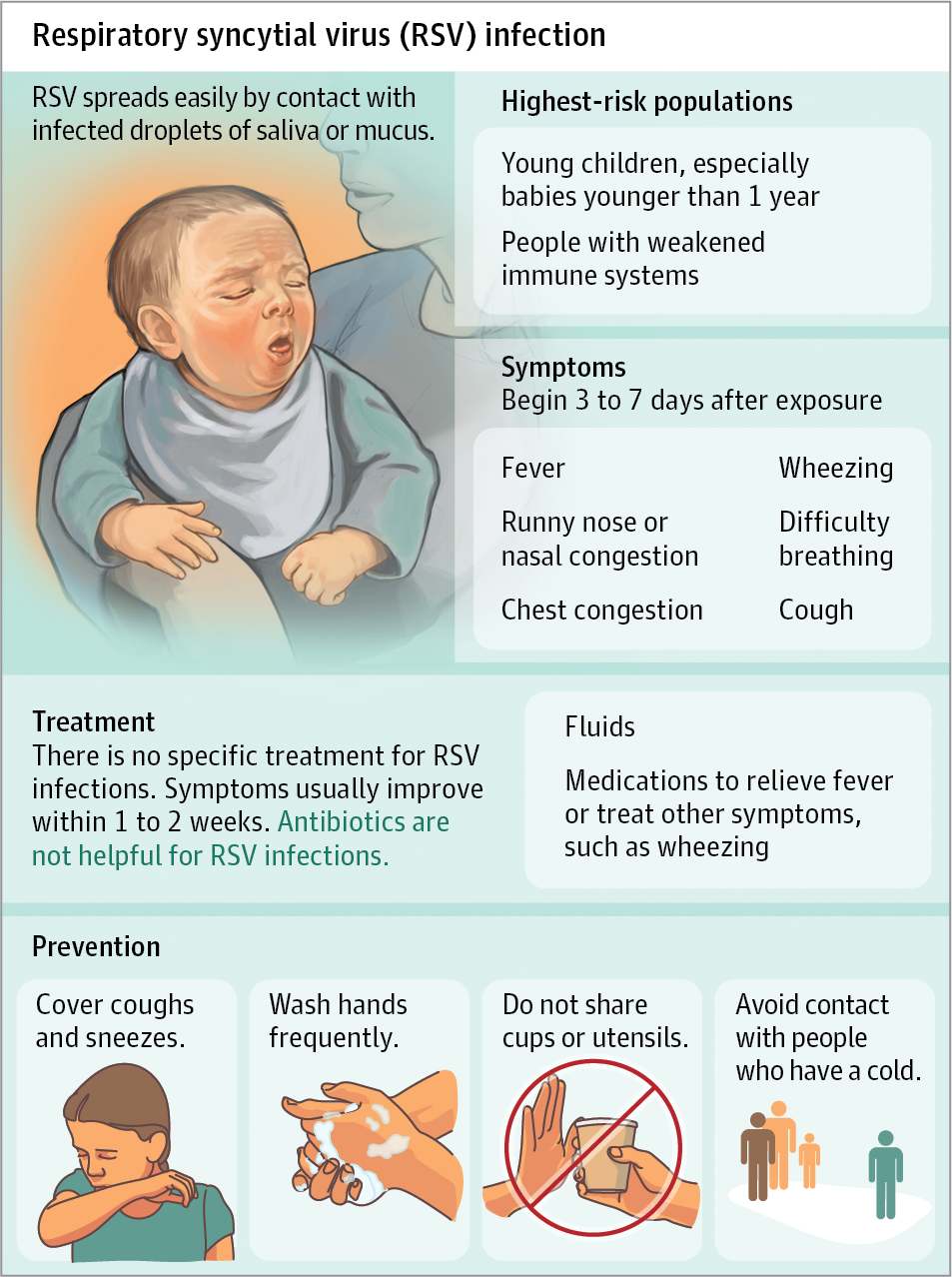
Respiratory syncytial virus (RSV) [Maternity/Peds]
Bronchiolitis, or inflammation of the bronchioles, is a significant cause of hospitalization in infants younger than 1 year. Respiratory syncytial virus(RSV) is the causative agent in more than half of cases. Etiology and Incidence Infants usually acquire the disease from an older child or adult, particularly a family member or daycare contact, who has a minor respiratory illness. RSV infection is easily communicable and is acquired mainly through contact with contaminated surfaces and hand-to-hand transmission. Nosocomial outbreaks in pediatric hospitals are common. RSV can live on skin or paper for up to 1 hour and on cribs and other nonporous surfaces for up to 6 hours. Although it is not airborne, it is highly communicable. It is usually transferred by inadequately washed hands. Meticulous hand hygiene decreases the spread of organisms. Pathophysiology In bronchiolitis, edema and the accumulation of mucus and cellular debris cause obstruction of the bronchioles. Infants' bronchioles are very small and can become obstructed quickly. Airway resistance is increased during the inspiratory and expiratory phases of respiration because of the small air passages. Hyperinflation of the lungs results from air trapping because the bronchioles constrict during expiration. Atelectasis can occur if obstruction becomes complete and trapped air is absorbed. Normal gas exchange is impaired, and the infant becomes hypoxic. Some infants have mild respiratory alkalosis; more frequently, metabolic acidosis is observed. The child with bronchiolitis is most acutely ill during the first 48 to 72 hours after the onset of the disease. Improvement usually occurs in a few days. Symptoms may last for 10 to 14 days. Manifestations A mild upper respiratory tract infection usually precedes the development of bronchiolitis. Serous nasal drainage, sneezing, low-grade fever, and anorexia are present for several days, followed by the onset of acute respiratory distress, manifested by the following signs and symptoms: • Tachypnea—respiratory rates of 60 to 80 breaths/min • Tachycardia—heart rate greater than 140 beats/min • Wheezing, crackles, or rhonchi • Intercostal and subcostal retractions with or without nasal flaring • Cyanosis Feeding may be difficult because of increased respirations, which interfere with sucking and swallowing. The body temperature varies from hypothermic to as high as 41° C (105.8° F). Management Give Synagis shot to prevent RSV. Infants with mild bronchiolitis can be treated at home with fluids, humidification, and rest. Infants with respiratory distress are hospitalized for supportive treatment. Cool, humidified oxygen is delivered if the oxygen saturation decreases to less than 90% on room air to relieve dyspnea, hypoxemia, and insensible water loss from tachypnea. Nursing Diagnosis and Planning The diagnoses and expected outcomes that may be appropriate for the infant with bronchiolitis and the infant's family are as follows: • Impaired Gas Exchange related to airway edema and increased mucus. Expected outcome. The infant will have adequate gas exchange, as evidenced by oxygen saturation above 95% on room air. • Ineffective Airway Clearance related to increased secretions. Expected outcome. The infant will exhibit clear breath sounds and normal respiratory rate, depth, and rhythm. • Deficient Fluid Volume related to decreased intake and insensible loss. Expected outcome. The infant will maintain adequate hydration, as evidenced by moist mucous membranes, a flat fontanel, urine output normal for age, and stable weight. • Ineffective Thermoregulation related to illness. Expected outcome. The infant will demonstrate a body temperature within normal limits. • Anxiety related to hospitalization and the child's dyspnea. Expected outcome. The infant will demonstrate decreased anxiety, as evidenced by adequate sleep and stable vital signs. The parents will verbalize understanding of the infant's condition and be able to participate appropriately in the infant's care.
{kind=link}
{kind=link}
Page 15
Bronchiolitis [Maternity/Peds]
Number one prevention is hand washing!! Considered a viral infection Most cases of bronchiolitis are caused by the respiratory syncytial virus (RSV). Severe symptoms are usually only evident in young infants One of its symptoms is trouble breathing Contact Precautions - From respiratory secretions / Mask How many wet diapers has the child had? - Looks into urine output in relation to dehydration. Priority Assessments in Order: Apply 02 Reassess 02 Administer antibiotics Provide oral fluids Do not give ampicillin (A type of antibiotic) with viral infections!!
{kind=link}
Page 16
Laryngomalacia
Weakness of the airway walls above the vocal chords = FLACCIDITY A common birth defect of the larynx. Symptoms Acyanotic - lacking a blue appearance of the skin and mucous membranes. Stridor Retractions Symptoms get worse when infant cries or is supine. Laryngomalacia is a congenital softening of the tissues of the larynx (voice box) above the vocal cords. This is the most common cause of noisy breathing in infancy. The laryngeal structure is malformed and floppy, causing the tissues to fall over the airway opening and partially block it
Want to create your own Notes for free with GoConqr? Learn more.