Description
|
|
Created by Sarah-Jean Edmonds
almost 9 years ago
|
|
Page 1
Blood Administration
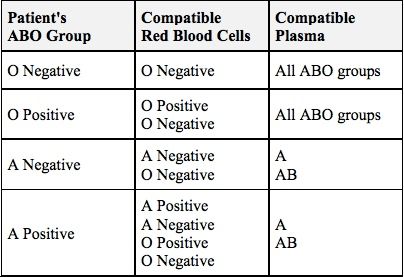
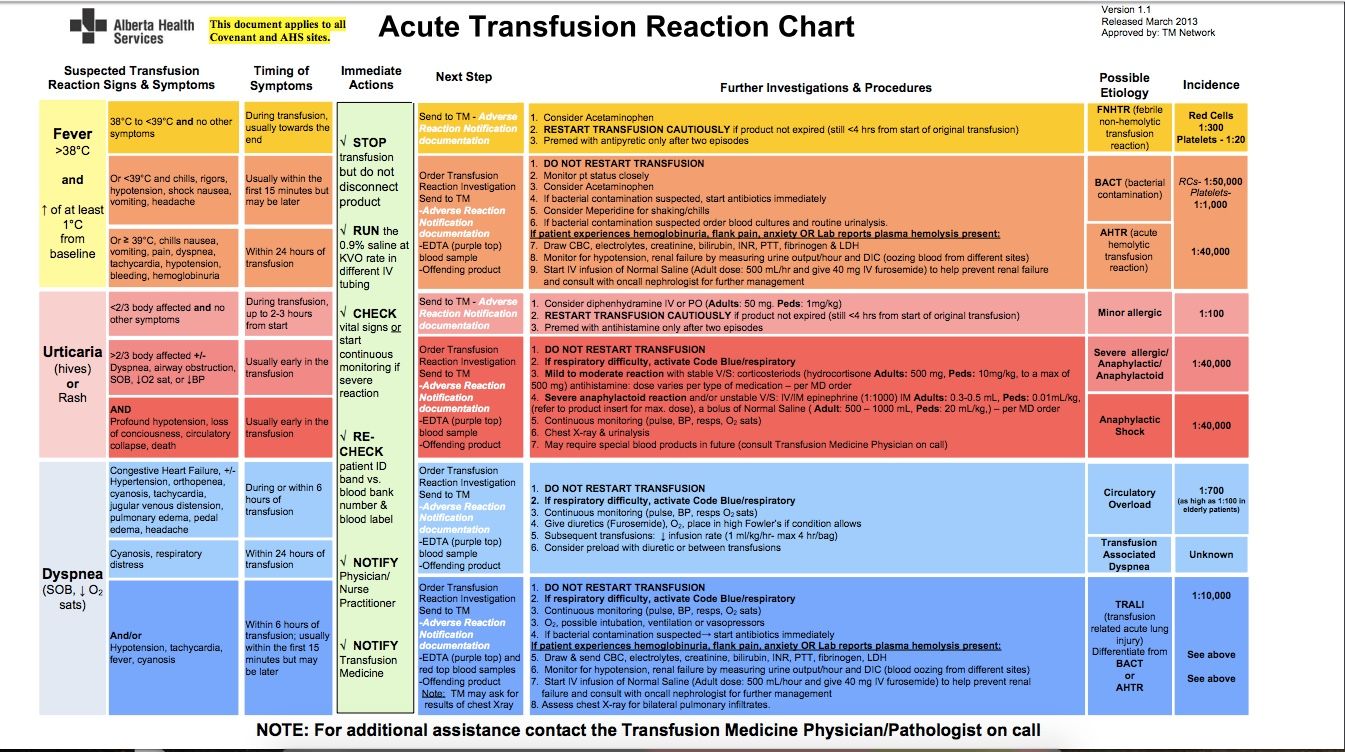
Blood products used and the conditions they treat: Red Blood CellsSymptomatic anemiaHemoglobin level of 7–8 g/dL in stable, hospitalized patientsHemoglobin ≤8 g/dL in the presence of clinical symptoms for patients with cardiovascular disease PlasmaReplacement of clotting factors in patients with a demonstrated deficiency or for single-factor deficiency when concentrate not availableCorrect coagulation deficienciesBefore an invasive procedureBurn victims PlateletsAcute thrombocytopenia:Platelet count <10,000/μLStable patients with chronic thrombocytopenia: 5000/μLFever or recent hemorrhage (with bleeding controlled): 10,000/μLPatients with coagulopathy, on heparin, or with anatomic lesion likely to bleed: 20,000/μL Procedure for blood administration: Confirm consent Verify the order assess for 18-20 gauge catheter of needle inserted into vein assess baseline vital signs, oxygen saturation and lung sounds assess blood type and check label prior to administration perform double check of blood product/patient monitor transfusion of blood/components and monitor for complications identify and use appropriate infusion tubing to deliver blood/components with. 170 to 260 micron filter; tubing is good for 8 hours and as many infusions as can be done in that time sideline solution container of .9% normal saline. The use of dextrose in water or hypotonic solutions can cause RBC hemolysis as a result of cell swelling. Lactated Ringer’s solution is not recommended because it contains enough ionized calcium to overcome the anticoagulant effect of CPDA-1 and allows small clots to develop. transfuse blood/blood components at appropriate ratesVitals taken in first 15 minutes1ml/min for the first 15 minutes, look for anaphykaxis, do not leave Transfusion must be complete within 4 hours dispose of blood bag and tubing properly. (biohazard) A note on cross-match: Lab comes to draw, need two people to identify patient. Cross match is good for 72 hours, but can be extended if there’s no transfusion in the first 72 hours. Cross match takes 30 minutes for someone who hasn’t gotten a transfusion before. 10 hours for Denane’s dad. The more transfusion a pt has, the longer it takes to cross match because they make more and more antibodiesType O: no ABO Antigens on Red Cells; anti-A and anti-B Antibodies in Plasma Type A: A antigens on red cells, anti-B antibodies in plasmaType B: B antigens on red cells; anti-A antibodies in plasmaType AB: A+B antigens on red cells; no antibodies in plasma
{kind=link}
{kind=link}
Want to create your own Notes for free with GoConqr? Learn more.