4639391
Description
Quiz by Rachael Eleanor Alexandra, updated more than 1 year ago
|
|
Created by Rachael Eleanor Alexandra
about 8 years ago
|
|
Question 1
Question
Is this impacted canine palatal or buccal to the centrals?
{kind=link}
Answer
-
palatal
-
buccal
Question 2
Question
Is this impacted canine palatal or buccal to the arch?
{kind=link}
Answer
-
Palatal
-
Buccal
Question 3
Question
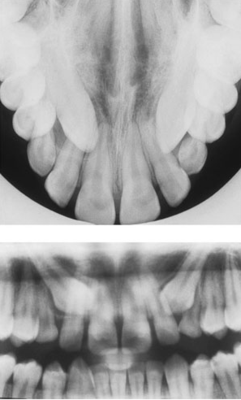
Are these impacted canines palatal or buccal to the arch?
{kind=link}
Answer
-
Palatal
-
Buccal
Question 4
Question
1. Gain [blank_start]consent[blank_end]. Check for [blank_start]latex[blank_end] allergies, explain to patient the procedure and why we need the rubber raincoat.
2. Select clamp - [blank_start]DW[blank_end] for primary molars and premolars, [blank_start]FW[blank_end] for partially erupted molars, [blank_start]BW[blank_end] for permanent molars.
3. Tie [blank_start]floss[blank_end] around clamp before application
4. Rubber dam must be pre-[blank_start]punched[blank_end]. 3 overlapping holes for [blank_start]single[blank_end] tooth, 5-6 overlapping holes for [blank_start]trough[blank_end]
5. Clamp applied [blank_start]first[blank_end] without rubber dam
6. Apply rubber dam when clamp is [blank_start]secure[blank_end] - rock [blank_start]lingually[blank_end], then [blank_start]buccally[blank_end].
7. [blank_start]Frame[blank_end] attached to support dam
8. [blank_start]Trough[blank_end] isolation required dam to be stretched to include all required teeth
9. Apply wedget or wedge to [blank_start]mesial[blank_end] aspect of most mesial isolated tooth.
Answer
-
consent
-
latex
-
DW
-
FW
-
BW
-
floss
-
punched
-
single
-
trough
-
first
-
secure
-
lingually
-
buccally
-
Frame
-
Trough
-
mesial
Question 5
Question
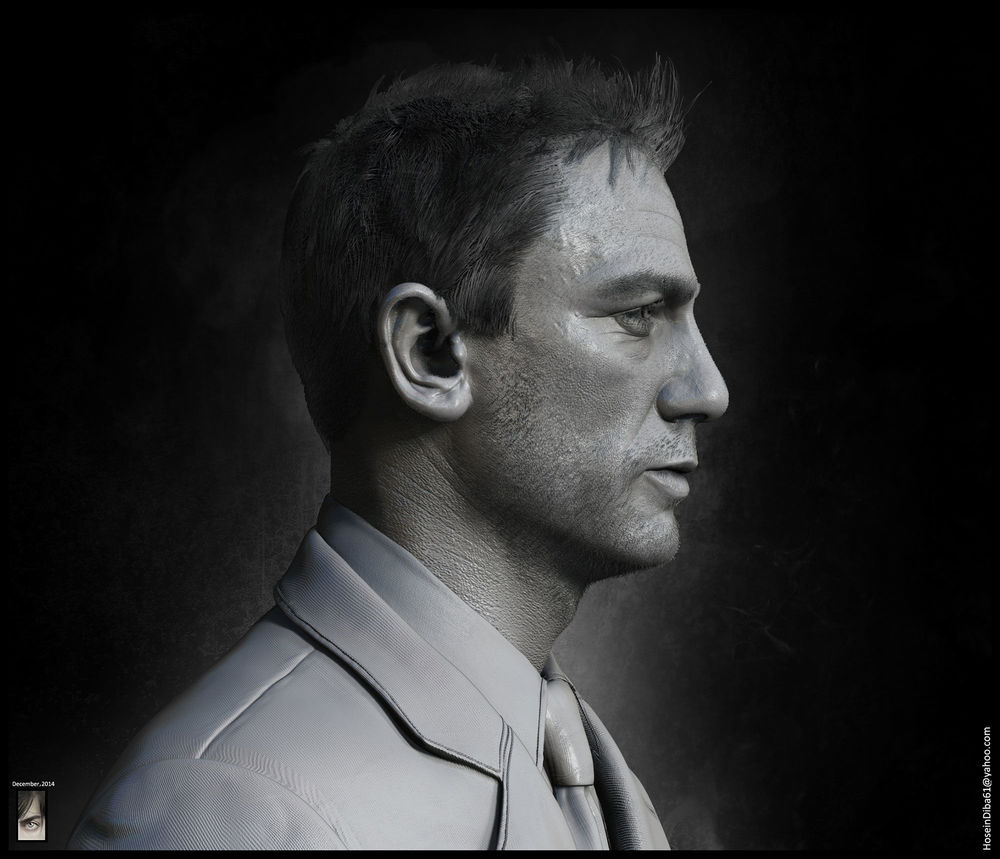
Label the image with different aspects required for an extra oral examination.
{kind=link}
Answer
-
Facial appearance
-
Skin
-
Eyes
-
Ears
-
Neck
-
TMJ
-
MoM
-
Facial appearance
-
Skin
-
Eyes
-
Ears
-
Neck
-
TMJ
-
MoM
-
Facial appearance
-
Skin
-
Eyes
-
Ears
-
Neck
-
TMJ
-
MoM
-
Facial appearance
-
Skin
-
Eyes
-
Ears
-
Neck
-
TMJ
-
MoM
-
Facial appearance
-
Skin
-
Eyes
-
Ears
-
Neck
-
TMJ
-
MoM
-
Facial appearance
-
Skin
-
Eyes
-
Ears
-
Neck
-
TMJ
-
MoM
-
Facial appearance
-
Skin
-
Eyes
-
Ears
-
Neck
-
TMJ
-
MoM
-
Facial appearance
-
Skin
-
Eyes
-
Ears
-
Neck
-
TMJ
-
MoM
-
Thyroid
-
Thyroid
-
Thyroid
-
Thyroid
-
Thyroid
-
Thyroid
-
Thyroid
-
Thyroid
Question 6
Question
Label the correct lymph nodes for an EO exam from the dropdown menus
{kind=link}
Answer
-
Preauricular
-
Mastoid (posterior auricular)
-
Occipital
-
Parotid
-
Submandibular
-
Submental
-
Preauricular
-
Mastoid (posterior auricular)
-
Occipital
-
Parotid
-
Submandibular
-
Submental
-
Preauricular
-
Mastoid (posterior auricular)
-
Occipital
-
Parotid
-
Submandibular
-
Submental
-
Preauricular
-
Mastoid (posterior auricular)
-
Occipital
-
Parotid
-
Submandibular
-
Submental
-
Preauricular
-
Mastoid (posterior auricular)
-
Occipital
-
Parotid
-
Submandibular
-
Submental
-
Preauricular
-
Mastoid (posterior auricular)
-
Occipital
-
Parotid
-
Submandibular
-
Submental
-
Deep cervical chain
-
Supraclavicular
-
Deep cervical chain
-
Supraclavicular
-
Deep cervical chain
-
Supraclavicular
-
Deep cervical chain
-
Supraclavicular
-
Deep cervical chain
-
Supraclavicular
-
Deep cervical chain
-
Supraclavicular
-
Preauricular
-
Mastoid (posterior auricular)
-
Occipital
-
Parotid
-
Submandibular
-
Submental
-
Deep cervical chain
-
Supraclavicular
-
Preauricular
-
Mastoid (posterior auricular)
-
Occipital
-
Parotid
-
Submandibular
-
Submental
-
Deep cervical chain
-
Supraclavicular
Question 7
Question
Label the image with muscles of mastication you should palpate during EO exam.
{kind=link}
Answer
-
Temporalis
-
Trapezius
-
Masseter
-
Sternocleidomastoid
-
Temporalis
-
Masseter
-
Trapezius
-
Sternocleidomastoid
-
Temporalis
-
Masseter
-
Trapezius
-
Sternocleidomastoid
-
Temporalis
-
Masseter
-
Trapezius
-
Sternocleidomastoid
Question 8
Question
During a TMJ examination, you should stand behind the patient and palpate both joints [blank_start]simultaneously[blank_end]. The patient should be asked to [blank_start]open[blank_end] and close their mouth, and move their jaw [blank_start]laterally[blank_end]. You should note any clicking, [blank_start]locking[blank_end] (trismus), grinding or grating ([blank_start]crepitus[blank_end]), limited [blank_start]opening[blank_end], deviation, and pain.
Answer
-
simultaneously
-
open
-
laterally
-
locking
-
crepitus
-
opening
Question 9
Question
For an ID block you should do the following:
1. Explain what you are going to do; gain [blank_start]consent[blank_end]. Numbness will last for around [blank_start]2[blank_end] or [blank_start]3[blank_end] hours and patient should avoid hot drinks and [blank_start]biting[blank_end] their lip
2. Check for any [blank_start]allergies[blank_end] or contraindications. LA contains [blank_start]vasoconstrictors[blank_end] and an additive called [blank_start]sodium[blank_end] metabisulphate that could cause a reaction.
3. Check the [blank_start]expiry date[blank_end] on the cartridge, check your choice of [blank_start]vasoconstrictor[blank_end], check it has no [blank_start]air bubbles[blank_end].
4. Dry mucosa and apply [blank_start]topical[blank_end] anaesthetic - xylonor gel contains [blank_start]xylocaine[blank_end].
5. Put the needle together - long needles are coloured [blank_start]yellow[blank_end] and short needles [blank_start]blue[blank_end].
6. Check the [blank_start]bung[blank_end] is orientated correctly!
7. Patient should open their mouth [blank_start]wide[blank_end] so you can visualise anatomical landmarks. Ensure you have the operating [blank_start]light[blank_end] on to visualise tissues for the block.
8. Palpate the [blank_start]coronoid process[blank_end] with your thumb at the greatest depression - known as the coronoid [blank_start]notch[blank_end]
9. Slide your thumb [blank_start]posteriorly[blank_end] until you can palpate the [blank_start]internal oblique ridge[blank_end].
10. The syringe is positioned between the [blank_start]premolars[blank_end] on the opposite side and needle inserted at the level of the thumb.
11. The injection site is 1cm above the [blank_start]occlusal[blank_end] plane of the molars and medial to the thumb, lateral to the [blank_start]pterygomandibular[blank_end] raphe.
12. The needle is advanced around 2.5cm. [blank_start]Bone[blank_end] should be contacted to ensure correct position.
13. When the needle meets the middle section of the rams, withdraw slightly by 1 or 2 mm so that the needle is not [blank_start]subperiosteal[blank_end]
14. Make sure you [blank_start]aspirate[blank_end] at this point.
15. Inject [blank_start]slowly[blank_end] - 1.5ml or 2/3rds of a cartridge. This improves patient comfort and you can assess any patient [blank_start]reactions[blank_end] to the solution before you inject too much.
16. The rest of the cartridge is injected as you [blank_start]withdraw[blank_end] the needle to block the [blank_start]lingual[blank_end] nerve.
17. Double click the syringe and dispose in the [blank_start]sharps bin[blank_end]
18. Remove gloves and apply alcohol gel.
Answer
-
consent
-
2
-
3
-
biting
-
allergies
-
vasoconstrictors
-
sodium
-
expiry date
-
vasoconstrictor
-
air bubbles
-
topical
-
xylocaine
-
yellow
-
blue
-
bung
-
wide
-
light
-
coronoid process
-
notch
-
posteriorly
-
internal oblique ridge
-
premolars
-
occlusal
-
pterygomandibular
-
Bone
-
subperiosteal
-
aspirate
-
slowly
-
reactions
-
withdraw
-
lingual
-
sharps bin
Question 10
Question
What must you ensure you do after extracting a tooth? (check all that apply)
Answer
-
Allow socket to bleed freely
-
Give post operative instructions
-
Write notes on the computer
-
Compress socket with fingers
-
Get patient to bite down on rolled gauze
-
Allow patient to rinse socket with water
-
Allow patient to leave immediately
-
Check for haemostasis
-
Dispose of tooth immediately
-
Check for apices of tooth
Question 11
Question
How long should a patient NORMALLY take to achieve haemostasis post-extraction?
Answer
-
<5 minutes
-
<10 minutes
-
<20 minutes
-
>1 hour
Question 12
Question
How long should a patient wait before coming back to the LDI with a non healing socket or continued symptoms?
Answer
-
5 days
-
3 days
-
7 days
-
10 days
-
2 weeks
Question 13
Question
How many times daily should a patient carry out salty mouth rinses on the day after an extraction?
Answer
-
Once
-
Twice
-
Three times a lady
-
Ten
Question 14
Question
What is the correct secondary movement for extraction of an UL5?
Answer
-
Palatal
-
Buccal and palatal
-
Rotational
-
Down
Question 15
Question
What is the primary movement for all dental extractions?
Answer
-
Apical
-
Buccal
-
Rotational
-
Coronal
Question 16
Question
What is the secondary movement for a LR2 extraction?
Answer
-
Rotational
-
Palatal
-
Lingual
-
Buccal
Question 17
Question
What movement is more likely to result in root fracture during extraction of upper molars?
Answer
-
Rotational
-
Palatal
-
Buccal
-
Apical
Question 18
Question
Luxators are used to: (tick all that apply)
Answer
-
Sever the periodontal ligament attachment
-
Expand the socket
-
Lever the tooth from the socket
Question 19
{kind=link}
Answer
-
Luxator
-
Elevator
-
Forceps
Question 20
{kind=link}
Answer
-
Luxator
-
Elevator
-
Forceps
Question 21
Question
Which forceps would you most likely use for a lower premolar extraction?
Answer
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Question 22
Question
Which forceps would you use for an upper left lateral incisor extraction?
Answer
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Question 23
Question
You've just given a patient a new set of dentures and are giving them some advice. You advise them:
- Leave dentures in for at least [blank_start]24[blank_end] hours initially
- Feeling of compaction and excess [blank_start]saliva[blank_end] will [blank_start]decrease[blank_end] with time
- There may be [blank_start]sore[blank_end] spots to begin with
- Their lips will [blank_start]relax[blank_end] with time
- Eat [blank_start]small[blank_end] sized pieces of food and eat [blank_start]evenly[blank_end] on [blank_start]both[blank_end] sides of mouth
- Avoid [blank_start]sticky[blank_end] foods
- [blank_start]Muscles[blank_end] need to be re educated to accommodate dentures
- [blank_start]Clean[blank_end] denture using a soft nylon brush with [blank_start]soap[blank_end] over the sink. They can use [blank_start]disclosing[blank_end] solutions to help them clean.
- Soak dentures overnight in denture cleanser ([blank_start]hypochlorite[blank_end] solution)
- Clean mouth with warm [blank_start]salt[blank_end] water [blank_start]twice[blank_end] daily
Answer
-
24
-
saliva
-
decrease
-
sore
-
relax
-
small
-
evenly
-
sticky
-
both
-
Muscles
-
Clean
-
soap
-
disclosing
-
hypochlorite
-
salt
-
twice
Question 24
Question
Unerupted incisors have several possible causes, these tend to be either [blank_start]hereditary[blank_end] or environmental in origin.
Environmental causes include:
1. Trauma - [blank_start]avulsion[blank_end] or intrusion of the primary teeth that causes damage to the permanent tooth. This may include the root/crown axis to deviate, known as [blank_start]dilaceration[blank_end]. The permanent tooth may also become [blank_start]ankylosed[blank_end] to the bone. In these cases [blank_start]extraction[blank_end] may be required and tooth replacement options considered.
2. [blank_start]Retained[blank_end] primary teeth causing [blank_start]delayed[blank_end] eruption - this may cause a physical [blank_start]obstruction[blank_end] to the path of eruption of the permanent tooth. The most straightforward option here would be [blank_start]extraction[blank_end] of the primary tooth if there is no other obstruction and the teeth are close to [blank_start]eruption[blank_end].
Hereditary causes may include the presence of [blank_start]supernumerary[blank_end] teeth in the arch, [blank_start]cleft[blank_end] lip or palate, abnormal tooth/tissue ratio or other rarer conditions such as [blank_start]cleidocranial[blank_end] dysostosis.
The other option is that the permanent teeth may be congenitally [blank_start]absent[blank_end]!
According to the RCS guidelines, we should start monitoring unerupted incisors when:
1. [blank_start]Contralateral[blank_end] teeth erupted more than 6 months ago
2. Both centrals are unerupted and the lowers erupted more than [blank_start]12[blank_end] months ago
3. Deviation in the normal sequence of eruption
During an intra oral examination, you may find that:
- The primary teeth have been retained beyond normal [blank_start]exfoliation[blank_end] dates (which is [blank_start]6[blank_end] or [blank_start]7[blank_end] years for upper centrals, [blank_start]7[blank_end] or [blank_start]8[blank_end] years for upper laterals)
- There may be buccal or palatal [blank_start]swellings[blank_end] on palpation
- Note the space available for incisors - [blank_start]9[blank_end]mm for centrals and [blank_start]7[blank_end]mm for laterals
You may wish to take some [blank_start]radiographs[blank_end] to determine the cause of the unerupted teeth. The [blank_start]parallax[blank_end] technique can locate the position of impacted teeth.
Answer
-
hereditary
-
avulsion
-
dilaceration
-
ankylosed
-
extraction
-
Retained
-
delayed
-
obstruction
-
extraction
-
eruption
-
supernumerary
-
cleft
-
cleidocranial
-
absent
-
Contralateral
-
12
-
6
-
7
-
7
-
8
-
exfoliation
-
swellings
-
9
-
7
-
radiographs
-
parallax
Question 25
Question
The upper canines usually erupt around [blank_start]11[blank_end] or [blank_start]12[blank_end] years of age. [blank_start]Congenitally[blank_end] absent canines is rare 0.3%. [blank_start]Impaction[blank_end] of canines is more common, and is usually bilateral. You should be able to [blank_start]palpate[blank_end] maxillary canines around 9 years of age in the buccal [blank_start]sulcus[blank_end].
Causes of impacted maxillary canines may be due to the:
- [blank_start]Long[blank_end] path of eruption
- [blank_start]Short[blank_end] rooted or [blank_start]absent[blank_end] upper lateral incisors ([blank_start]peg[blank_end] laterals)
- Crowding
- [blank_start]Retention[blank_end] of primary canine (an indicator rather than a cause!)
- [blank_start]Genetic[blank_end] factors. It may run in the [blank_start]family[blank_end].
- It should also be noted that impacted canines is associated with other dental anomolies
You should first assess the child [blank_start]clinically[blank_end] to see if you can tell where the tooth is displaced. If you suspect displacement you may wish to take some [blank_start]radiographs[blank_end].
The radiographs most commonly used for assessing ectopic canines are [blank_start]panoramic[blank_end] radiographs, upper [blank_start]occlusal[blank_end] radiographs, lateral [blank_start]cephalometric[blank_end] (for more accurate localisation), [blank_start]cone beam[blank_end] computerised tomography, and periodicals (useful for prognosis of retained deciduous canines).
Management depends on wether the teeth are [blank_start]buccally[blank_end] or [blank_start]palatally[blank_end] displaced.
Buccal displacements are usually due to [blank_start]crowding[blank_end], so relief of [blank_start]crowding[blank_end] is usually the option
Palatal displacements may require surgical [blank_start]exposure[blank_end] with orthodontic [blank_start]alignment[blank_end], or surgical [blank_start]removal[blank_end] of the impacted canine.
Occasionally unerupted canines can cause [blank_start]resorption[blank_end] of adjacent lateral incisor roots and possibly the centrals. In this case intervention should be done swiftly.
Answer
-
11
-
12
-
Congenitally
-
Impaction
-
palpate
-
sulcus
-
Long
-
Short
-
absent
-
peg
-
Retention
-
Genetic
-
family
-
clinically
-
radiographs
-
panoramic
-
occlusal
-
cephalometric
-
cone beam
-
buccally
-
palatally
-
crowding
-
crowding
-
exposure
-
alignment
-
removal
-
resorption
Want to create your own Quizzes for free with GoConqr? Learn more.