Types of Croup: Laryngotracheobronchitis (LTB = Most Common/Viral), Bacterial Tracheitis (Viral), Acute Epiglottitis (Bacterial/Haemophilus influenzae type b (Hib)
Symptoms:
"Barking" Seal Cough
Musical breathing = STRIDOR
Tachypnea (Fast Breathing)
Retractions
Steeple Sign (In LTB) = Subglottic [below vocal chords] narrowing
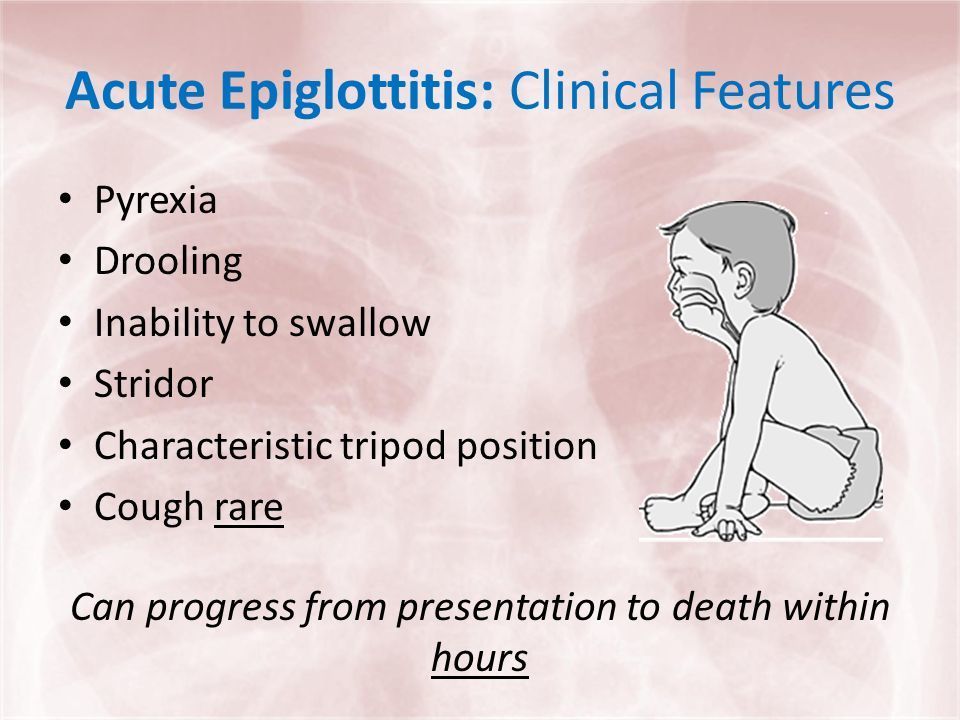
Tripod Position - Requires IMMEDIATE attention
Coughing at night
Treatment:
Increase fluids (IV Therapy), Oxygen, Can be treated at home, artificial airway, Racemic epinephrine , provide a cool humidified environment (Night Air), keep calm crying aggravates the airway.
Caption: : The hallmark sign of croup is a harsh “barky” or “seal”-like cough.
Slide 2
1. Acute Spasmodic Laryngitis = Viral & Subglottic
2. Acute Laryngotracheobronchitis (LTB) = Viral & Subglottic
3. Acute Epiglottitis = Supraglottic (above vocal cords)/ Bacterial (caused by Haemophilus influenzae type b (Hib)
Parainfluenza virus is the most common cause of croup!
1.) Racemic Epinephrine Nebulized with oxygen - to decrease demand and bronchospasms.
2.) Dexamethasone - Given PO, IV or IM to decrease airway inflammation.
3.) Antibiotics - For bacterial croup infections only!
4.) Acetaminophen may be given to reduce fever.
Slide 4
Hospitalization
For children with severe symptoms (progressively worsening stridor, cyanosis, decreased oxygen saturation, retractions), hospitalization is necessary. Humidified oxygen and IV fluids are given until respiratory distress subsides and the child can take adequate fluids by mouth. Hospitalized children may also receive racemic epinephrine, and/or dexamethasone.
Provide cool humidified mist / Night Air = Most Relief for Croup
Intercostal Retractions = Means respiratory distress is getting worse!
Emphasize hand washing to stop the spread of infection.
Slide 5
Epiglottis - Bacterial Form of Croup
Signs of Epiglottitis—Four D’s
Drooling
Dysphagia (difficulty swallowing)
Dysphonia (difficulty talking)
Distressed inspiratory efforts
Also Includes:
High Fever
Epiglottis is edematous and cherry red
Caused by: Haemophilus influenzae type b (Hib)
Be on the Look out for the 4 Signs: Drooling, Dysphagia (Difficulty swallowing), Dsyphonia (Difficulty speaking), Distressed Inspirations
Slide 7
Signs of Epiglottis Require Immed. Atten!
A 5-year-old child brought to the emergency department with signs of apprehension and whose voice is thick and muffled also has drooling, agitation, and no spontaneous cough. What is the most effective nursing intervention?
Have the child seen by a primary care provider immediately.
In this case, the child needs immediate medical intervention, because the symptoms are rapidly progressive. Otherwise give IV antibiotic therapy.
Meds: Vancomycin (Adv. Reac. - Rash)
Slide 8
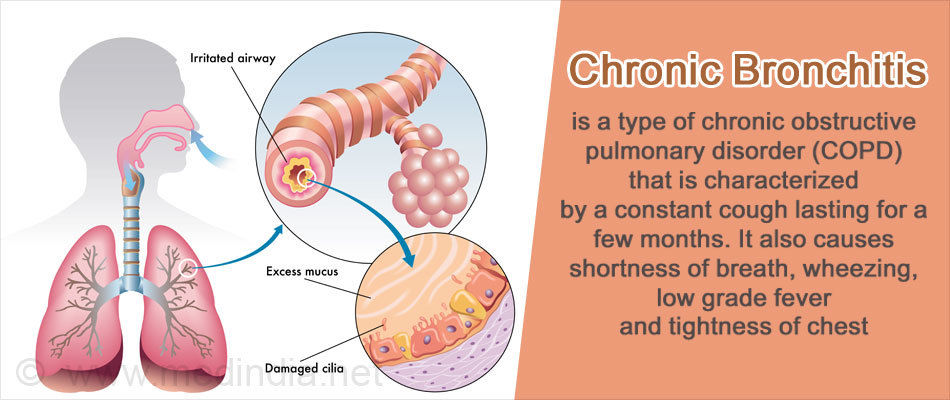
Bronchitis
Inflammation of the bronchi.
Rarely exists by itself, occurs wth a common cold.
Signs & Symptoms:
Fever
Persistant Cough
Wheezing
Rhonchi
Crackles in Lung
Prolonged expiration
Acute bronchitis is usually viral in origin.
More common in boys and winter months.
AVOID
Antihistamines should be avoided because of their drying effect on secretions.
Cough suppressants are not recommended unless the cough interferes with the child’s ability to rest.
Exposure to cigarette smoke should be avoided
GIVE
Antibiotics should be given only if a bacterial infection is confirmed by culture or if the clinical findings support the diagnosis.
Encourage fluids
Acetaminophen is administered for an elevated temperature (usually above 38.3° C [101° F])
Quiet activities should be provided for diversion
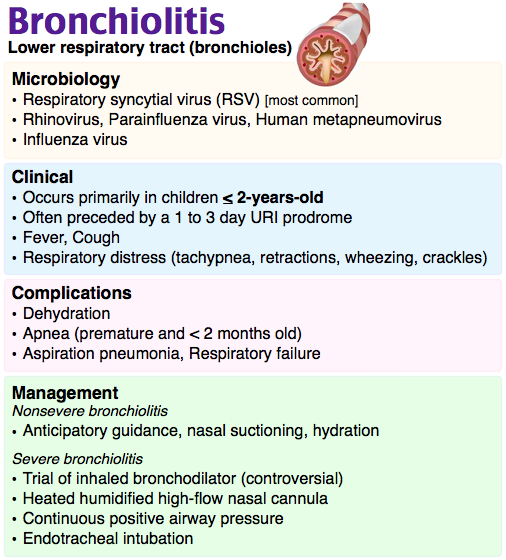
Respiratory syncytial virus (RSV) is the causative agent in more than half of cases.
A mild upper respiratory tract infection usually precedes the development of bronchiolitis.
• Tachypnea—respiratory rates of 60 to 80 breaths/min
• Tachycardia—heart rate greater than 140 beats/min
• Wheezing, crackles, or rhonchi
• Intercostal and subcostal retractions with or without nasal flaring
• Cyanosis
Feeding may be difficult because of increased respirations, which interfere with sucking and swallowing. The body temperature varies from hypothermic to as high as 41° C (105.8° F).
Slide 11
RSV prevention = Intramuscular palivizumab (Synagis) administered monthly throughout the RSV season
Parenteral administration of fluids may be necessary for acutely ill infants who are dehydrated from tachypnea or poor intake
Cool, humidified oxygen is delivered if the oxygen saturation decreases to less than 90% on room air to relieve dyspnea, hypoxemia, and insensible water loss from tachypnea
The infant should be positioned with the head and chest at a 30- to 40-degree angle and the neck slightly extended to maintain an open airway and decrease pressure on the diaphragm.
Isolate the infant with RSV infection in a single room or place the infant in a room with other RSV-infected infants. Meticulous hand hygiene is imperative. Nurses caring for these infants should not care for other high-risk children. Maintaining Contact Precautions (i.e., wearing a gown and gloves) reduces nosocomial transmission of RSV.
Treatment
Slide 12
Pertussis (Whooping Cough)
Symptoms:
Runny nose
Fever / Chronic cough
Violent and uncontrollable coughing (Paroxysms)
Place on droplet precaution
Prevented by a TDap shot
The drug clarithromycin, which is an antibiotic to treat pertussis, should be administered to the child.
Provide humidified oxygenation and suction.
Give fluids
The child should be placed on his or her side
Mumps
Influenza
Pertussis
* Remember M.I.P = Most Important Person *
Slide 14
Asthma
Corticosteroids are the first-line therapy for inflammation in children with asthma.
WHEEZING = Asthma
The normal respiratory rate for newborns is 30 to 60 breaths/min
Status Asthmaticus can be described as constant and unrelieved by bronchodilators.
Short acting Vs Long acting bronchodilators
The possible side effects of short-acting inhaled beta agonists include a fast heartbeat, nervousness and tremors/ shakiness, which usually pass quickly when the medicine is inhaled.
EXAMPLES - ENDINGS OF "ROL"
Albuterol (Ventolin®, Proventil®, Airet®)
Albuterol sulfate (ProAir HFA®)
Levalbuterol (Xopenex®)
Metaproterenol sulfate (Alupent®, Arm-a-Med®, Metaprel®)
Pirbuterol acetate (Maxair®)
Terbutaline sulfate (Brethair®, Brethine®, Bricanyl®)
Bitolterol mesylate (Tornalate®)
SHORT ACTING (QUICK RELIEF)
Slide 16
LONG ACTING (ASTHMA CONTROL)
Taken everyday, even when symptoms are not present.
Do not show immediate results, but work slowly over time
Used together with a steroid medication
Examples
Serevent® (salmeterol)
Foradil® (formoterol)
Slide 17
Parts of the Lower Airway
Bronchi
Bronchioles
Alveoli
Slide 18
if PCo2 levels are greater than 45mmHg = Respiratory Acidosis
{kind=link}
{kind=link}
{kind=link}
{kind=link}