2593390
Description
Flashcards by Jo Gledhill, updated more than 1 year ago
|
|
Created by Jo Gledhill
about 9 years ago
|
|
| Question | Answer |
| Describe the health and social care act of 2012? | Most extensive reorganisation of the NHS to date Primary Care Trusts (PCTs) and Strategic Health Authorities (SHAs) abolished Clinical Commissioning Groups (CCGs) have been established from April 1st 2013 PCTs used to control 80% of the NHS budget, this will now be controlled by CCGs CCGs include all GP practices as well as other health professionals A CCG can commission care from any service that meets NHS standards and costs (i.e. private health care may gain NHS business) Health and Wellbeing Boards act as a forum for local commissioners Public Health England will provide national leadership and expert services to support public health |
| What is the National Institute for Health and Clinical Excellence (NICE)? | Provides guidance; Sets quality standards; Manages database to improve peoples’ health and prevent and treat ill health; Makes recommendations to NHS on: a) new and existing medicines, treatments and procedures; b) treating and caring for people with specific diseases and conditions Cost saving gained through recommendation NICE approved psychological therapies; Making available: CBT, Counselling, Interpersonal therapy |
| Lord Layard-Health Economist- 2005 influential paper- reasoned that funding by DoH could...? | improve provision of psychological therapies for treatment of anxiety and depression positively impacting on number of people fit for work reduce benefits, improve mental health and wellbeing. Economic, moral and clinical arguments used. |
| What is the favored model of mental health care delivery? | Stepped care: Begins with self help, self directed interventions, CCBT, brief therapy, graduate to more complex input only if required. Approach should alleviate pressure on existing mental health services in theory. |
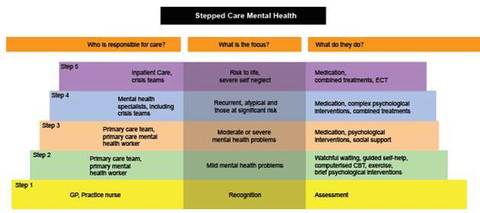
| Describe the Improving access to psychological therapies, IAPT, stepped care model | |
| Give arguments against IAPT and Layard's report | depression and anxiety are viewed as discrete conditions that will get better with the right treatment. Layard writes about people being ‘cured’, implying that these conditions are similar to illnesses like measles that can reliably diagnosed and simply treated. Yet There is considerable evidence that social and economic factors – taking poverty as only one – are significant contributory factors to both depression and anxiety. Are people really ill or are they responding to the realities of stressful and difficult lives? |
| Clinical psychologists often work in multidisciplinary teams (MDTs) in the NHS These include other disciplines including..? | Team manager – organises and manages the team Medical doctors – psychiatrists or other medical doctors Nurses – mental health or clinical specialist nurses Social workers – professionals that focus on social care needs Occupational therapists – clinicians who specialise in occupational and daily living skills Community support workers – people without a professional qualification who work with clients and may have an NVQ Secretarial and support staff – responsible for administration Psychotherapists, counsellors and counselling psychologists – other professionals who can provide psychological therapy Other specialist disciplines – physiotherapists, prison staff etc. |
| What is a MDT? | Two or more professions make their respective contributions Each contribution can stand on its own or work with others The team have a shared objective Information should be consistent from all team members |
| Outline the benefits of MDTs | Continuity of care Comprehensive view of patients’ needs Application of a range of skills Mutual professional support and education A better and more coherent sense of care for the patient Quick and easy communication between professions |
| what are the key factors in team working? | Agreed goals Agreed plans Effective communication styles Clear team roles Competent leadership Mutual respect Shared responsibility Healthy team dynamics |
| what are some possible challenges involved in MDTs | Working with different models Psychological formulation Medical model Social care needs Working with different professionals Stereotyping of the roles of different professions Lack of recognition for individual’s background and expertise Concerns over status and pay differences Working with different people Different beliefs and experiences Different personality types Different ideas about teams |
| Outline the background to Shafran, Layard & Clark (2013) | The English Improving Access to Psychological Therapies (IAPT) initiative aims to make evidence-based psychological therapies for depression and anxiety disorder more widely available in the National Health Service (NHS). 32 IAPT services based on a stepped care model were established in the first year of the programme. We report on the reliable recovery rates achieved by patients treated in the services and identify predictors of recovery at patient level, service level, and as a function of compliance with National Institute of Health and Care Excellence (NICE) Treatment Guidelines. |
| Describe the method used by Shafran, Layard and Clark (2013) | Data from 19,395 patients who were clinical cases at intake, attended at least two sessions, had at least two outcomes scores and had completed their treatment during the period were analysed. Outcome was assessed with the patient health questionnaire depression scale (PHQ-9) and the anxiety scale (GAD-7). |
| What did Shafran, Layard and Clark (2013) find? | Data completeness was high for a routine cohort study. Over 91% of treated patients had paired (pre-post) outcome scores. Overall, 40.3% of patients were reliably recovered at post-treatment, 63.7% showed reliable improvement and 6.6% showed reliable deterioration. Most patients received treatments that were recommended by NICE. When a treatment not recommended by NICE was provided, recovery rates were reduced. Service characteristics that predicted higher reliable recovery rates were: high average number of therapy sessions; higher step-up rates among individuals who started with low intensity treatment; larger services; and a larger proportion of experienced staff. |
| The Improving Access to Psychological Therapies (IAPT) programme was established to treat people with ---- and not ---- | people with mild to moderate depression and anxiety people with intellectual disabilities |
| the Positive Practice Guide for people with intellectual disabilities was published in? | 2009 |
| Outline the three steps of the original Stepped Care Approach (Dodd et al, 2011) | Step 1 is conceived of as recognition of the problem. Step 2 is seen as the low-intensity service which can include guided self-help, computerised CBT, psychoeducation groups, and behavioural activation and exercise. Step 3 is high-intensity service and involves delivery of evidence-based psychological therapies such as cognitive behaviour therapy (CBT), eye movement desensitisation and reprogramming (EMDR), interpersonal therapy (IPT), behavioural activation, counselling and couples therapy |
| What does IAPT say about people with intellectual disabilities? (Dodd et al, 2011) | The Positive Practice Guide for People with Learning Disabilities was published in January 2009 (IAPT, 2009). It says that IAPT services may have to take a flexible approach to providing psychological therapies that are effective for people with intellectual disabilities, including offering: materials in easy-to-understand formats assessments and NICE-approved psychological interventions which have been adapted to meet the needs of people with intellectual disabilities appointments at specific times or specific dates, perhaps coinciding with individual needs or carer availability longer sessions than usual to take account of the person’s varying levels of understanding and need additional support from therapists or requiring the presence of a carer or independent advocate engagement (where possible with strategic primary health care facilitators) for people with intellectual disabilities to support access to assessment and services engagement with community intellectual disability team (community learning disability team – CTLD) |
| what did Dodd et al (2011) conclude? | Plans are under way for full roll-out of IAPT services, yet little attention has been paid to the needs of people with intellectual disabilities. It is unclear how effective clearly structured pathways or stepped care approaches are for people with intellectual disabilities. Current IAPT services have set requirements that may prevent people with intellectual disabilities from initially accessing the service, and meeting its requirements in terms of the usability and pace of the service. IAPT services will need to think carefully about selecting people who can use their service, and the adaptations required if they want to meet the needs of the selected people with intellectual disabilities in terms of staff training, approach, pace and the effect that it might have on contract performance. Audit and research are needed on how IAPT services have responded to the needs of people with intellectual disabilities and their effectiveness for this group of people. |
| What barriers to successful MDTs are outlined in Fleissig et al's 2006 review | A number of empirical studies have emphasised problems in attendance.58, 60, 65, 66 and 76 Attendance at colorectal MDMs is variable with many core members, especially gastroenterologists and oncologists, participating infrequently.66 A survey of 136 surgeons examined attendance levels at MDMs by different members of the breast cancer team,60 and found that over 95% of surgeons and breast care nurses and 90–95% of radiologists and pathologists were present for the whole meeting. By contrast, only 70% of clinical oncologists and 44% of medical oncologists attended the entire meeting. Another problem that is frequently identified in empirical studies is the absence of clerical support for MDT working. A study of colorectal cancer teams66 revealed that 62% (102 of 165) had difficulty running their MDM, and of these, 32% (33 of 102) did not have a dedicated MDT clerk. As a result, specialist nurses often had to organise meetings instead of carrying out their own work. |
| Outline Brown et al (2000) | This paper reports on an investigation of three interdisciplinary mental health teams. The discussion of the responses highlights the boundaries that exist between different professional roles and areas of responsibility. Whereas there is some evidence of role blurring, which was welcomed by a few respondents, others sought to preserve their own professional identity within the multidisciplinary environment. In a paradoxical sense, the lack of managerial direction and the encouragement of generic working seemed to make some respondents all the more insistent on separate professional identities. We conclude that, far from being a relic of the past or a product of ‘ingrained attitudes’, boundaries between professions are actively encouraged by the experience of interdisciplinary modes of working |
| What exactly do psychologists do? | Work with individuals and families: Provides individual psychological care to patients and families Provides psychometric testing using standardised tests Offers a psychological perspective to the team, MDT meetings, Reflective practice groups, Consultation to team members Offers psychological support to the team Reflects on how the team is working as a system, provides a safe space for team members if necessary, models compassionate and sensitive team working Research knowledge and skills Produces evidence based reviews of pertinent issues Conducts service related research projects (e.g. audit) Teaching and training Provides teaching on psychology related issues Increasingly psychologists are asked to support team members by offering consultation This can support the team member’s own work using psychological theory and approaches. This can be done with individual team members or through groups such as reflective practice groups |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.